Article Text

Abstract
Background It is uncertain whether mechanical thrombectomy (MT) increases the probability of a good outcome (modified Rankin Scale (mRS) 0–2) in patients with Alberta Stroke Program Early CT Score (ASPECTS) 0–6.
Objective To assess the impact of MT in patients with pretreatment ASPECTS 0–6.
Methods According to PRISMA guidelines, we performed a systematic search of three databases for series of patients with ASPECTS 0–6 treated by MT. Random-effects meta-analysis was used to pool the following: rate of mRS 0–2 at 3 months follow-up, symptomatic intracranial hemorrhage (sICH), and mortality rates.
Results We included 17 studies and 1378 patients with ASPECTS 0–6 (1194 MT, 184 medical management). The rate of mRS 0–2 was 30.1% and 3.2% after MT and medical management, respectively. MT gave higher odds of mRS 0–2 (OR 4.76, p=0.01). Patients with ASPECTS 6 and 5 had comparable rates of good outcome (37.7% and 33.3%, respectively). Overall, the rate of mRS 0–2 was 17.1% in patients with ASPECTS 0–4: 22.1% and 13.9% of patients with ASPECTS 4 and 0–3 were functionally independent, respectively. Successful recanalization (Thrombolysis in Cerebral Infarction grade 2b–3) gave higher odds of mRS 0–2 than unsuccessful reperfusion (OR 5.2, p=0.001). The MT group tended to have lower odds of sICH compared with the controls (OR 0.48, p=0.06). Patients aged <70 years had higher rates of mRS 0–2 than those aged >70 years (40.3% vs 16.2%).
Conclusions Patients with ASPECTS 0–6may benefit from MT. Successful reperfusion increases the probability of 3-month functional independence without increasing the risk of sICH. Patients with ASPECTS 5 and 6 have comparable outcomes. MT can still enable approximately one in four patients with ASPECTS 4 to be independent, whereas only 14% of subjects with ASPECTS 0–3 regain a good functional outcome.
- stroke
- thrombectomy
- thrombolysis
Statistics from Altmetric.com
Introduction
In 2015 several randomized trials showed the superiority of mechanical thrombectomy (MT) combined with IV thrombolysis (IVT) over IVT alone for stroke patients with a large vessel occlusion.1–5 However, selection of the patients with acute ischemic stroke who may benefit from MT is a complex process involving several variables6: the severity of symptoms (scored with the National Institutes of Health Stroke Scale, NIHSS), time of onset, baseline modified Rankin Scale (mRS) score, comorbidities, and extension of the early ischemic changes defined as CT or DWI-ASPECTS (Alberta Stroke Program Early CT Score)7 for anterior circulation occlusions, in combination with the assessment of collaterals and/or perfusion imaging. Growing evidence suggests that MT may be offered to patients with large vessel occlusion who do not meet current top-tier evidence recommendations.8 Large initial infarct volume has been described as an independent factor of poor outcome,9 and ASPECTS ≤6 has been used as the exclusion threshold in most randomized trials. Consequently, the overall treatment effect was likely driven by a cohort of patients with ASPECTS ≥7 .3–5 10–12 Therefore, it is still debatable whether patients with ASPECTS 0–6 may benefit from endovascular thrombectomy. The American Heart Association/American Stroke Association (AHA/ASA) guidelines recommended MT as reasonable treatment for patients with ASPECTS <6, but the class of recommendation was weak (IIb) with a moderate level of evidence derived from non-randomized studies.6 Accordingly, the results of randomized trials such as the ongoing TENSION (NCT03094715) and IN EXTREMIS trials are awaited to clarify the benefit of MT among these patients. Our meta-analysis, which pooled a large number of patients, aimed to investigate the outcomes of patients with ASPECTS 0–6 and subcategories of ASPECTS 0–3, 4, 5, and 6 undergoing MT.
Methods
Literature search
A comprehensive literature search of PubMed, Ovid EMBASE, and SCOPUS was conducted for studies published from January 2000 to June 2019. PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses13) guidelines were followed. The key words and detailed search strategy are shown in online supplemental table 1, and the studies included in our review are shown in online supplemental table 2. The inclusion criteria were as follows: (1) studies reporting series of patients with anterior circulation acute ischemic stroke and low ASPECTS (defined as ASPECTS ≤6) treated by MT; and (2) studies reporting outcome comparison between patients with low ASPECTS undergoing MT (cases) and medical treatment (controls). Exclusion criteria were as follows: (1) case reports; (2) review articles; (3) studies published in languages other than English; (4) in vitro/animal studies; and (5) studies reporting patients with ASPECTS >6. Because of the use of older devices, the IMS-III trial14 does not reflect the modern treatment management of acute ischemic stroke so this study was not included in our analysis. In cases of overlapping patient populations, only the series with the largest number of patients or most detailed data were included. Two independent readers screened articles in their entirety to determine eligibility for inclusion. A third author solved discrepancies.
Supplemental material
Data collection
We extracted the following: (1) rate of mRS 0–2 (good outcome) at 90 days; (2) mortality rate at 90 days; (3) symptomatic intracranial hemorrhage (sICH) rate; and (4) proportion of Thrombolysis in Cerebral Infarction (TICI) 2b–3 after thrombectomy. The rate of mRS 0–2 was analyzed based on patient age (<70 years vs ≥70 years) and based on the subgroups of low ASPECTS: very low (≤4), low (5), and intermediate (6). In addition, the very low ASPECTS subgroup was dichotomized into ASPECTS 0–3 and ASPECTS 4.
Outcomes
The primary objective of this study was to analyze the rate of mRS 0–2 at 3 months after MT of patients with acute ischemic stroke and low ASPECTS. For studies comparing MT and medical treatment among patients with low ASPECTS, we estimated the OR for good outcome at 3 months. The secondary objectives were to define: (1) mortality rate; (2) sICH rate; (3) proportion of TICI 2b–3; and (4) the influence of age, subgroups of low ASPECTS, cardiovascular risk factors, symptom onset to reperfusion time, and IVT on the rate of mRS 0–2.
Quality scoring
The Newcastle–Ottawa Scale15 was used for quality assessment of the included studies (see online supplemental table 3). The quality assessment was performed by two authors independently, and a third author solved discrepancies.
Statistical analysis
We estimated from each cohort the cumulative prevalence (percentage) and 95% CI for each outcome. Heterogeneity of the data was assessed by the Higgins index (I2) and subsequently the DerSimonian and Laird random-effects model was applied. Graphical representations were shown as forest plots. To evaluate the heterogeneity and bias, the subgroup analysis and funnel plot followed by Egger’s linear regression test were performed, respectively. To verify the consistency of outcome meta-analysis results, the influence of each individual study on the summary effect estimate was assessed by the sensitivity analysis (‘leave-one-out’ approach). Weighted random effects meta-regression analysis was performed to assess the influence of potential effect modifiers: we tested the relationship between the proportion of diabetes, hypertension, and dyslipidemia among patients with MT and the rate of mRS 0–2 at 3 months. In addition, meta-regression was used to test the association between the proportion of patients with IVT and the rate of mRS 0–2, as well as the relationship between the mean symptom onset to reperfusion time and the rate of good outcome. To compare the percentages of each group and to calculate the p values, the z-test was used when appropriate (see online supplemental table 4). Statistical significance was set at p<0.05. Meta-analysis was performed with ProMeta-2 (Internovi, Cesena, Italy) and OpenMeta (Analyst).
Results
Literature review
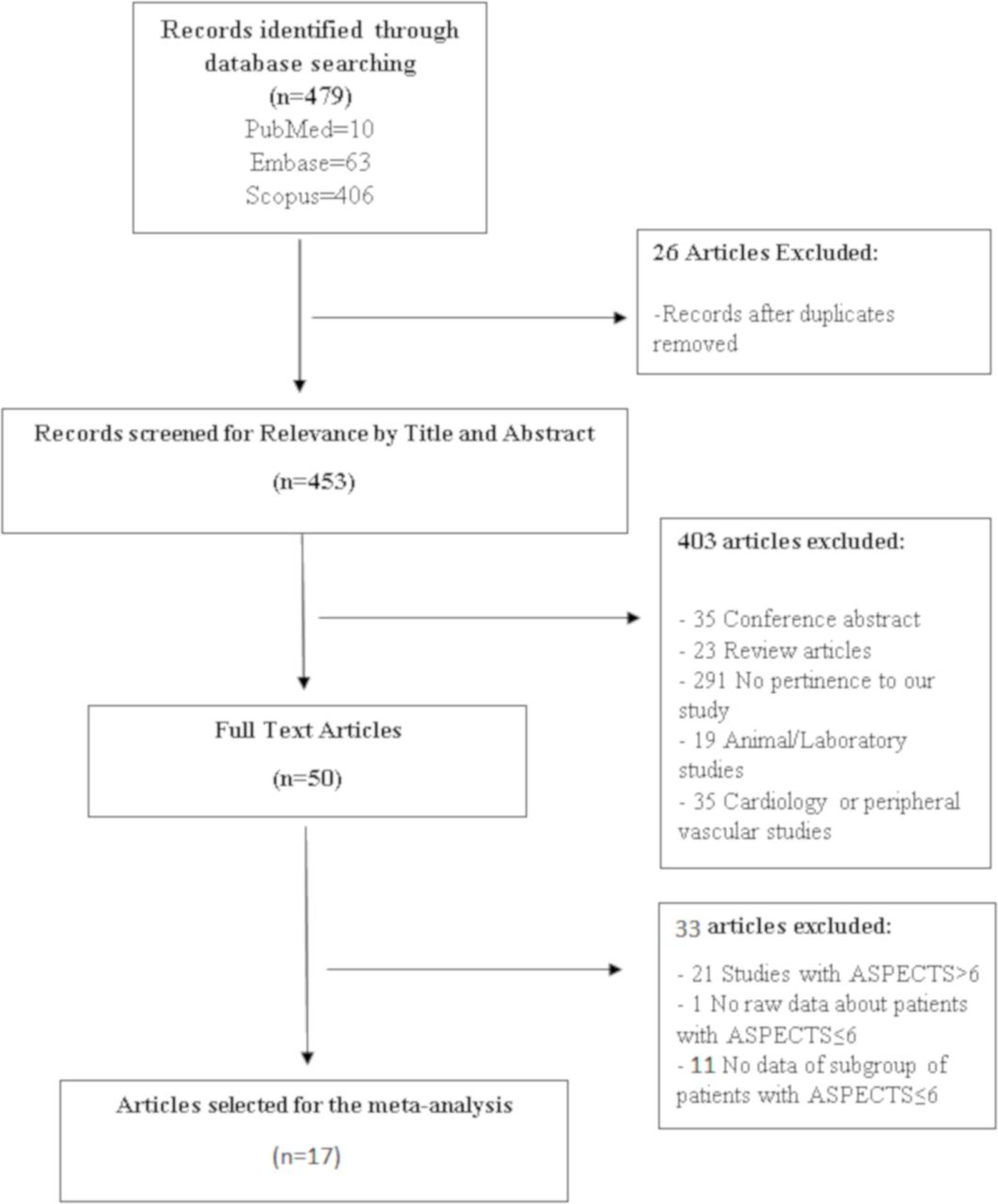
The studies included in our meta-analysis are summarized in online supplemental table 2. The search flow diagram is shown in figure 1.
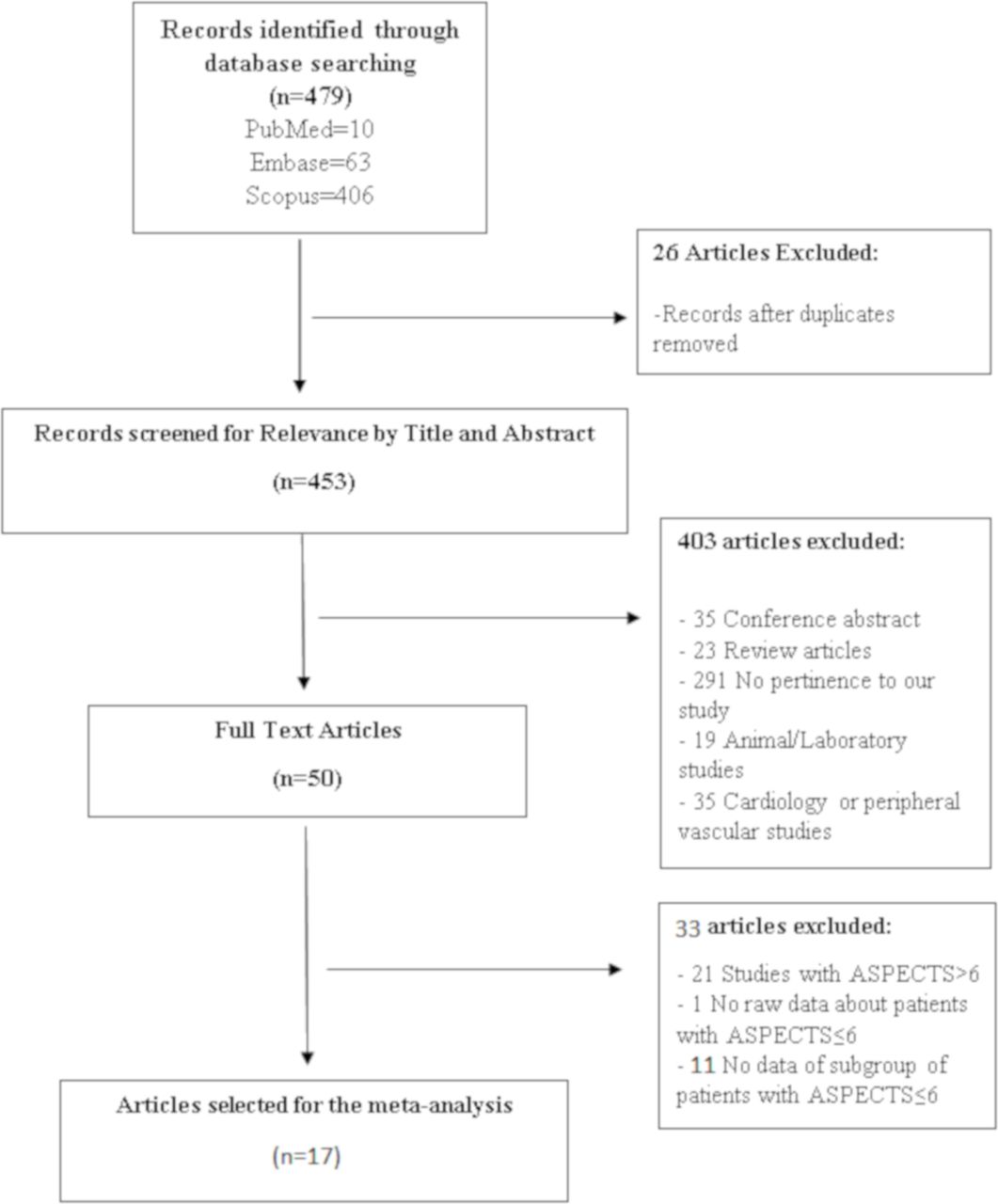
PRISMA diagram detailing the specifics of the systematic literature review. ASPECTS, Alberta Stroke Program Early CT Score.
A total of 17 studies and 1378 patients with acute ischemic stroke and ASPECTS ≤6 were included in our review. Overall, 1194 patients (cases) underwent MT (stent retriever, aspiration-first thrombectomy or combined techniques), whereas 184 patients (controls) were treated with medical therapy (IVT for eligible patients or conservative management). Five studies16–20 compared outcomes between the MT group and the medical treatment group whereas 12 studies21–32 reported series of patients with low ASPECTS exclusively treated with MT.
Quality of studies
Nine studies were retrospective series17–19 23 25 27–30 and eight studies had a prospective design.16 20–22 24 26 31 32 Two included series were prospective randomized trials.16 20 Overall, 11 articles (prospective studies16 20–22 24 26 31 32 and series with cases and controls16–19) were rated as high-quality studies based on the Newcastle–Ottawa quality assessment criteria (see online supplemental table 3).
Patient population
Mean age, sex, hypertension, and initial NIHSS scores were comparable in the MT and medical treatment groups (p>0.05), whereas dyslipidemia, diabetes and the proportion of patients treated with IVT were higher in the MT group. The most common location of the occlusion was M1 and carotid T in both groups (see online supplemental table 4).
The mean symptom onset to admission time was 115 min (range 10–380) and 130 min (range 37–642) in the MT and control groups, respectively (p=0.7). In the MT group the mean symptom onset to groin puncture time was 271.6 min (range 164–329) and the mean symptom onset to recanalization time was 286 min (range 153–370).
Clinical outcomes after mechanical thrombectomy and medical treatment among patients with ASPECTS ≤6
Proportion meta-analysis
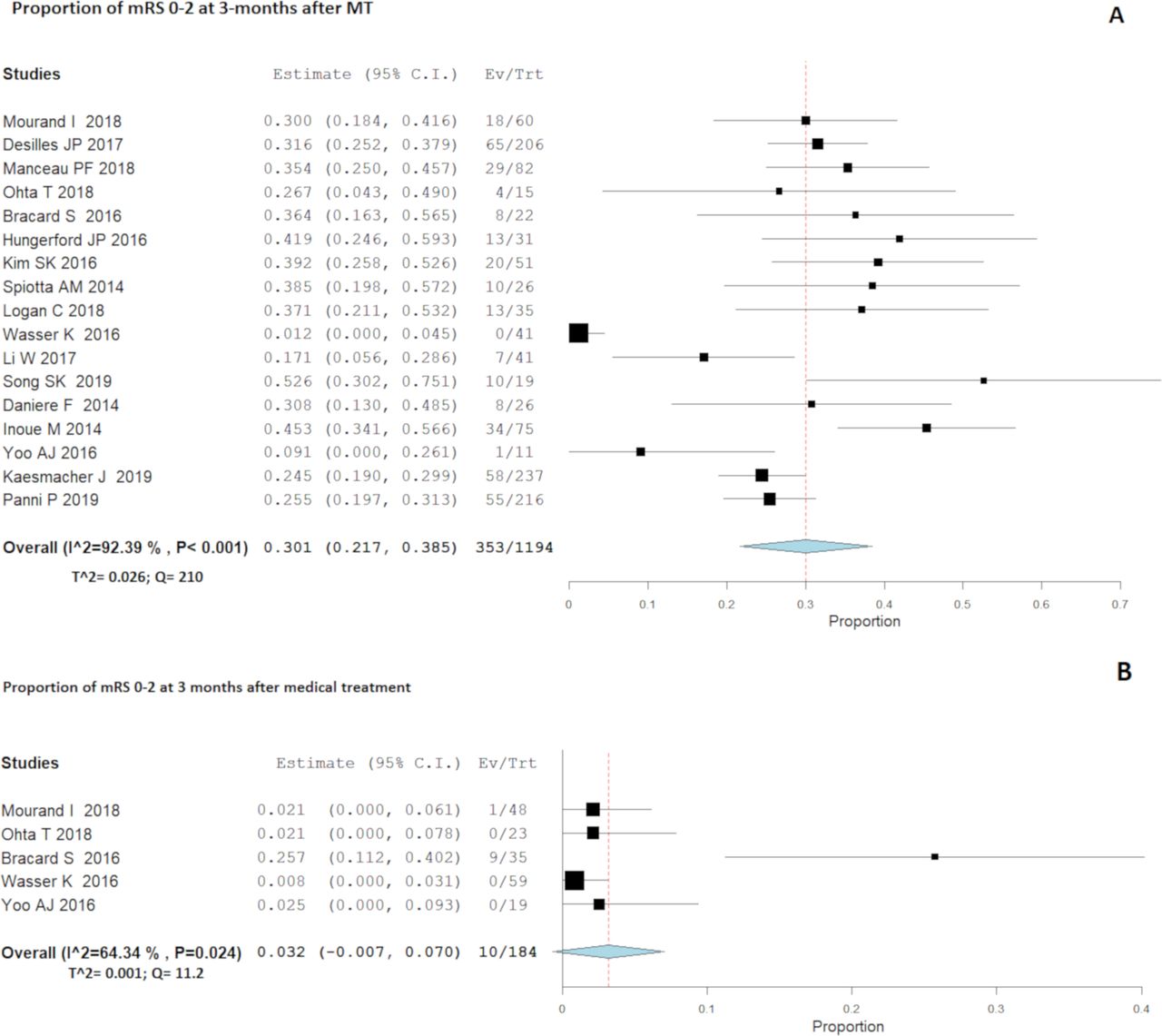
The investigated outcomes were analyzed with random-effect meta-analysis because this model incorporates heterogeneity among studies (figure 2). Overall, the rate of mRS 0–2 at 3 months was 30.1% (353/1194; 95% CI 21.7% to 38.5%, I2=92.4%) and 3.2% (10/184; 95% CI 0.7% to 7%, I2=64.3%) after MT and medical management, respectively (table 1). The funnel plot, followed by Egger’s linear regression test, excluded publication bias (p=0.5) (see online supplemental figure 1A). Meta-regression showed a non-significant variation of the effect size (p=0.2) over the investigation period (see online supplemental figure 1B). The sensitivity analysis showed that no individual study significantly influenced the rate of mRS 0–2 after MT among patients with low ASPECTS (see online supplemental figure 1C).
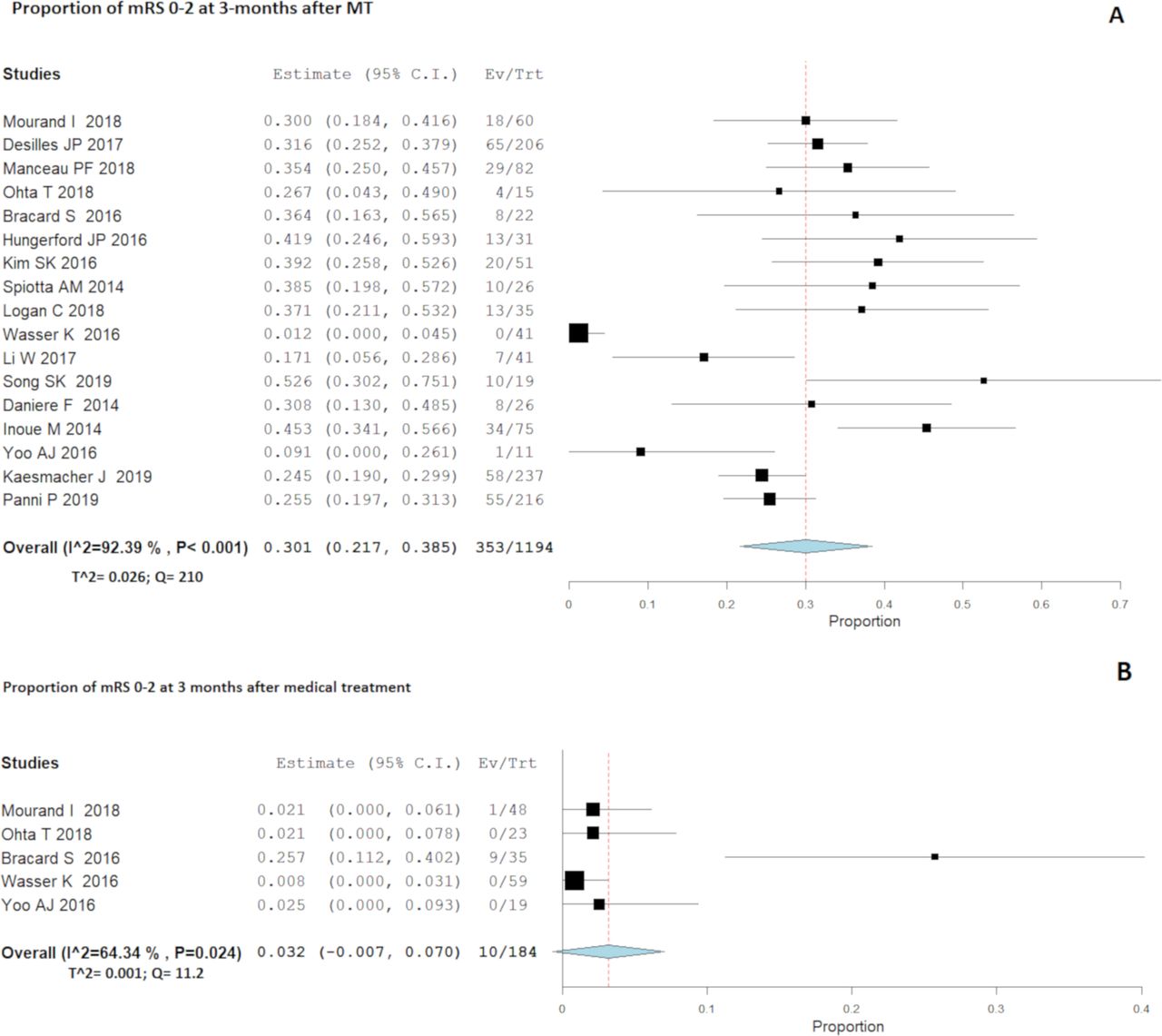
(A,B) Forest plot with random-effect model demonstrating the overall proportion of patients with Alberta Stroke Program Early CT Score (ASPECTS) 0–6 with modified Rankin Scale (mRS) score 0–2 at 3 months after (A) mechanical thrombectomy (MT) and (B) medical management .
Outcomes after mechanical thrombectomy (MT) and medical management of acute ischemic stroke patients with Alberta Stroke Program Early CT Score (ASPECTS) ≤6
The overall rate of mortality was 33.8% (406/1146, 95% CI 21% to 45%, I2=94%) and 47.7% (77/149, 95% CI 32.3% to 63%, I2=72%) after MT and medical management, respectively. Symptomatic ICH was lower in the MT group (254/1146=20%, 95% CI 11% to 28%, I2=95%) than in the control group (61/149=31.7%, 95% CI 9% to 72%, I2=98%). The rate of TICI 2b–3 revascularization after MT was 69.5% (673/978, 95% CI 56% to 80%, I2=94%).
OR meta-analysis
Five studies compared MT (cases) and medical management (controls) among patients with low ASPECTS (0–6); for this group of studies, meta-analysis results were expressed as OR for binary outcomes. Patients in the MT group had higher odds of a good outcome at 3 months compared with patients treated with medical therapy (OR 4.76, 31/149 vs 10/184, 95% CI 1.3 to 16.8, I2=31%) (p=0.01). Patients treated with MT showed a trend towards lower odds of sICH compared with the control group (OR 0.48, 32/127 vs 61/149, 95% CI 0.22 to 1.05, I2=0%) (p=0.06). The MT group had lower odds of mortality compared with the medical treatment group. However, this result was not statistically significant (OR 0.86, 58/127 vs 77/149, 95% CI 0.2 to 3.4, I2=79%) (p=0.8).
After MT, successful recanalization (TICI 2b–3) had significantly higher odds of mRS 0–2 than unsuccessful recanalization (OR 5.3, 197/535 vs 30/274, 95% CI 2.7 to 10, I2=49%) (p=0.001). The rate of sICH after MT was comparable among recanalized and non-recanalized patients (OR 0.77, 96/344 vs 65/200, 95% CI 0.48 to 1.2, I2=12%) (p=0.2).
Subgroup analysis: subcategories of low ASPECTS and patient age
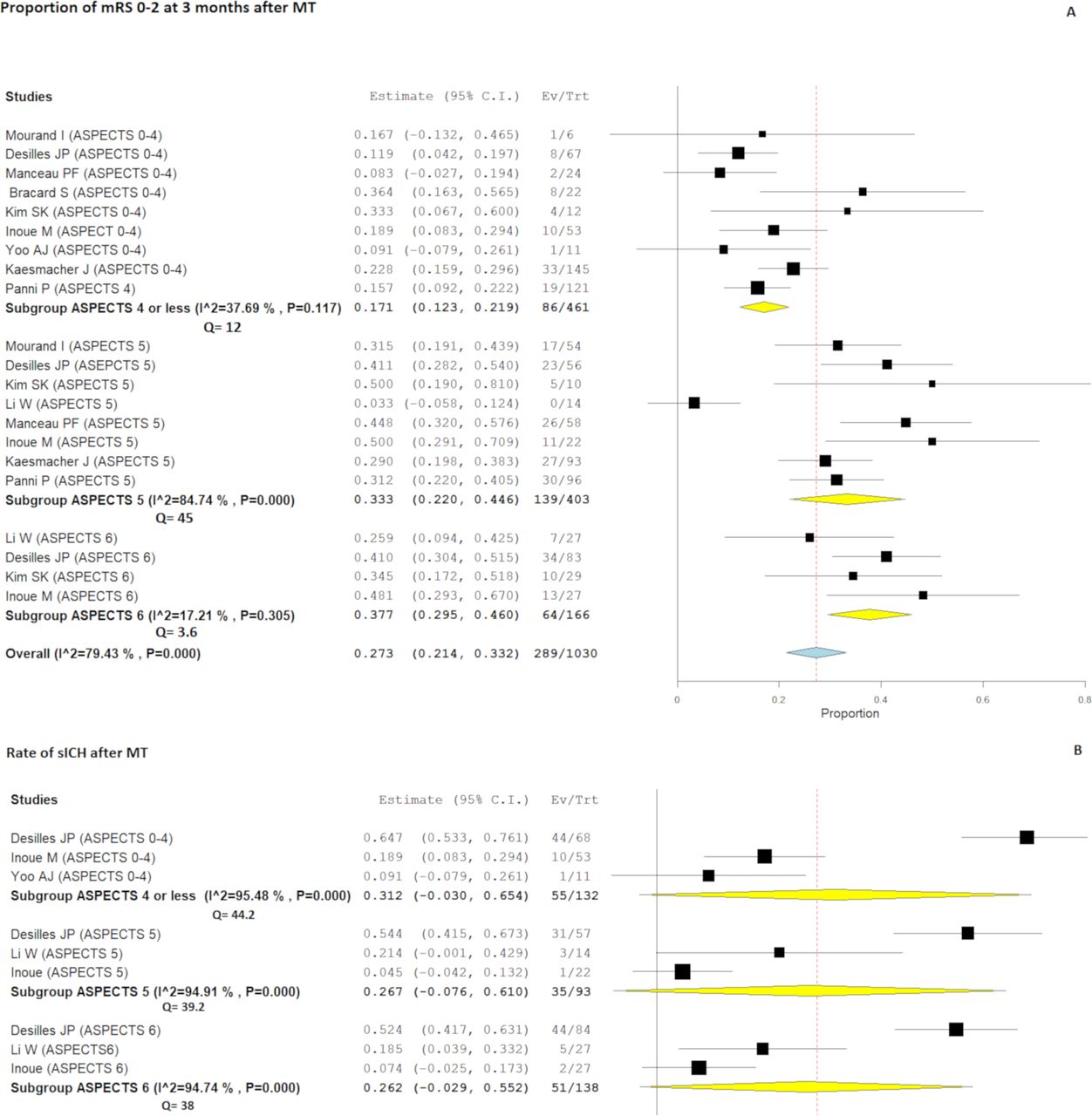
Series reporting clinical outcomes after MT were trichotomized as follows: very low ASPECTS (0–4), low ASPECTS (5), and intermediate ASPECTS (6) (figure 3A). The subgroup meta-analysis showed that patients with ASPECTS 6 and 5 had higher rates of good outcomes (64/166=37.7%, 95% CI 29.5% to 46%, I2=17.2% and 139/403=33.3%, 95% CI 22% to 44.6%, I2=84.7%, respectively), whereas subjects with very low ASPECTS (0–4) had a good outcome rate of 17.1% (86/461, 95% CI 12.3% to 21.9%, I2=37.6%). In the very low ASPECTS subgroup, patients with ASPECTS 4 had a 22.1% rate of good outcome (36/154, 95% CI 14.9% to 29.4%, I2=15.9%) whereas subjects with ASPECTS 0–3 had a 13.9% rate of mRS 0–2 (35/237, 95% CI 9.2% to 18.5%, I2=10.6%) at 3 months (see online supplemental figure 2).

{kind=link}
{kind=link}
{kind=link}
(A,B) Forest plot with random-effect model after tricotomization into ASPECT 0–4, 5, and 6. (A) Proportion of patients with mRS 0–2 at 3 months after mechanical thrombectomy (MT) based on ASPECTS subcategories. Proportion of symptomatic intracranial hemorrhage (ICH after MT based on the ASPECTS subcategories.
The rate of sICH after MT was 31.2% among the subgroup of patients with very low ASPECTS (55/132, 95% CI 3% to 6.5%, I2=95.4%), whereas it was lower among patients with ASPECTS 5 (35/93=26.7%, 95% CI 7.6% to 61%, I2=94.9%) and ASPECTS 6 (51/138=26.2%, 95% CI 2.9% to 55%, I2=94.7%) (figure 3B).
Patients younger than 70 years had higher rates of mRS 0–2 at follow-up compared with patients older than 70 years (36/88=40.3%, 95% CI 29.1% to 51.4%, I2=15.1% vs 18/95=16.2%, 95% CI 7.7% to 24.6%, I2=22.9%, respectively) (see online supplemental figure 3).
Meta-regression analysis: factors associated with mRS 0–2 at 3 months after MT
To assess the influence of potential effect modifiers on the rate of mRS 0–2 after MT, meta-regression analyses were conducted to test the relationship between potential pre-specified confounding variables. Overall, meta-regression showed no relationship between the proportion of patients with good outcome at follow-up and the following variables: proportion of patients with diabetes, IVT, dyslipidemia, and hypertension. In our study, only the mean symptom onset to recanalization time was significantly associated with the proportion of patients showing functional independence at follow-up after MT (p=0.03) (see online supplemental figure 4).
Study heterogeneity
Substantial heterogeneity (>50%) was noted for the following outcomes: overall rate of mRS 0–2, mortality, and sICH rates. Heterogeneity was also noted for the rate of TICI 2b–3 after MT. In the subgroup analysis, heterogeneity was lower after analysis of the subcategories with low ASPECTS and after dichotomization between older and younger patients. However, the subgroup of patients with ASPECTS 5 still showed high heterogeneity, which was likely related to the study by Li et al 26 which had a significantly lower rate of mRS 0–2 (figure 3).
Discussion
Our meta-analysis of nearly 1400 acute ischemic stroke patients with ASPECTS ≤6 showed that MT was associated with a higher rate of mRS 0–2 at 3-month follow-up compared with medical/conservative management. In addition, successful reperfusion (TICI 2b–3) increased the rate of favorable clinical outcome without impacting the risk of sICH. The ASPECTS 5 and 6 subgroups had comparable rates of favorable outcome. However, the rate of favorable outcome was noticeably reduced among patients with higher stroke volumes (ASPECTS 0–4), although the rate of ICH was not markedly increased. The effect of MT on the rate of favorable outcome was higher among younger patients.
In general, patients with pretreatment ASPECTS 0–6 have been under-represented in the most important MT trials due to the commonly accepted lower efficacy of reperfusion on the rate of favorable clinical outcome.9 10 Margerie-Mellon et al 33 found that a DWI-ASPECTS ≥7 was strongly associated with an ischemic infarct volume <70 mL. The EXTEND-IA5 and SWIFT PRIME4 trials excluded patients with infarct core volumes >70 mL and >50 mL, respectively; the ESCAPE trial10 excluded patients with ASPECTS <6, and the REVASCAT trial3 excluded those with ASPECTS <7 or DWI-ASPECTS <6. Recently, the DAWN11 and DEFUSE 312 trials showed the efficacy of MT after 6 hours in selected patients, including only patients with an ischemic core volume <51 mL and <70 mL, respectively. In the subgroup analysis of MR CLEAN,20 patients with non-contrast CT ASPECTS 0–4 represented 6% (30 patients) of the population, so no definite conclusions were given because the analysis was likely to be underpowered for this subgroup of patients with low ASPECTS.
Our meta-analysis, the largest to date, showed that MT for patients with ASPECTS 0–6 gave a higher rate of favorable functional outcome at 3-month follow-up compared with medical management (30% vs 3%). MT significantly impacted the final rate of good outcome (OR 4.76, 95% CI 1.3 to 16.8, p=0.01), especially among patients who experienced TICI 2b–3 recanalization (OR 5.2, 95% CI 2.7 to 10, p=0.001), without increasing the rate of mortality (OR 0.86, 95% CI 0.2 to 3.4, p=0.8). In the last individual patient data meta-analysis, the HERMES collaborators34 reanalyzed all imaging studies from seven randomized clinical trials, pooling 1764 patients with acute ischemic stroke. Overall, after MT, mRS 0–2 at 90 days was achieved in 48% of cases and in 25% of the 126 patients with ASPECTS 0–4 (adjusted OR 2.7, 95% CI 0.89 to 8.3). Similarly, our ASPECTS subgroup meta-analysis, pooling a relatively large number of patients, underlined a dramatic decrease in the favorable outcome among 461 patients with ASPECTS 0–4 (17%) compared with those with ASPECTS 5 and 6 (33% and 38%, respectively). In addition, MT can still allow approximately one in four subjects with ASPECTS 4 to regain independent function at 3 months; only 14% of ASPECTS 0–3 patients reached a good functional outcome after endovascular treatment. In a very recent multicenter study pooling seven institutional prospective registries, Kaesmacher et al 31 reported rates of 18% and 28% for 3-month mRS 0–2 among patients with ASPECTS 4 and ASPECTS 0–3, respectively. Similarly, the studies by Mourand et al 17 and Inoue et al 24 showed rates of favorable outcome between 16% and 20% in patients with ASPECTS 0–3 after MT. The HERMES meta-analysis reported no benefit of MT among subgroups of ASPECTS 0, 1, and 2, although the number of patients was too small (37 subjects) to provide definitive results.34 Ongoing clinical trials such as IN EXTREMIS and TENSION (NCT03094715) are needed to conclusively establish the efficacy of MT among patients with extremely low ASPECTS.
Our study, in line with other series of low ASPECTS patients treated endovascularly,17 21 25 27 showed that MT did not significantly increase the rate of sICH among both recanalized (TICI 2b–3) and non-recanalized patients. Although it was slightly higher among patients with ASPECTS 0–4, the rate of sICH was reasonably comparable among all three ASPECTS subcategories. On the other hand, the HERMES study showed the rate of sICH in patients with ASPECTS 0–434 to be four times higher.
Another important finding in our study is the impact of age on favorable outcome after MT in patients with a large ischemic core. Choosing a limit of 70 years, we reported higher rates of mRS 0–2 in younger patients than in older patients (40% and 26%, respectively). Older patients with low ASPECTS are likely to have a lower probability of being independent at 3 months; as reported in a previous analysis, age remains a strong predictor of the final outcome.10 However, our rate of functional outcome was quite comparable to that reported in a recent meta-analysis of MT in older patients10 35 or in a series of octogenarians with ASPECTS >6 undergoing endovascular thrombectomy.36
Finally, in our study shorter time of reperfusion was directly associated with a higher probability of functional independence after MT for patients with ASPECTS 0–6 (see online supplemental figure 4). This is in line with the generally accepted view that the absolute treatment effect of endovascular reperfusion decreases over time,37 highlighting the critical importance of reducing delays in time to MT also for patients with low ASPECTS.
Limitations
Our study has limitations. Only two of the available studies were randomized trials and only five studies compared MT and medical management. Accordingly, most of the data derived from series without control groups. The heterogeneity was quite high for most of the investigated outcomes. However, publication bias was reasonably excluded, and our study is the largest to date investigating endovascular thrombectomy among patients with ASPECTS 0–6 and relative subgroups.
Conclusions
Our results suggest that acute ischemic stroke patients with ASPECTS 0–6 may benefit from endovascular treatment. Successful reperfusion is likely to increase the probability of functional independence at 3-month follow-up without increasing the risk of sICH. The treatment outcomes are reasonably comparable between patients with ASPECTS 5 and 6, who are more likely to benefit from MT. Almost one in four patients with ASPECTS 4 can regain independent function at follow-up, whereas only 14% of subjects with a larger infarct volume (ASPECTS 0–3) benefit from MT. Future randomized trials are needed to confirm our results, especially among patients with very low ASPECTS.
References
Footnotes
Contributors Substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work: FC, ID, CD, P-HL, GG, CR, AB, VC. Drafting the work or revising it critically for important intellectual content: FC, ID, VC. Final approval of the version to be published: FC, ID, CD, P-HL, GG, CR, AB, VC. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: FC, ID, CD, P-HL, GG, CR, AB, VC.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Patient consent for publication Not required.