Article Text

Abstract
Coronavirus disease 2019 (COVID-19) results from infection by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). It was first reported in Wuhan, China in patients suffering from severe pneumonia and acute respiratory distress syndrome and has now grown into the first pandemic in over 100 years. Patients infected with SARS-CoV-2 develop arterial thrombosis including stroke, myocardial infarction and peripheral arterial thrombosis, all of which result in poor outcomes despite maximal medical, endovascular, and microsurgical treatment compared with non-COVID-19-infected patients. In this review we provide a brief overview of SARS-CoV-2, the infectious agent responsible for the COVID-19 pandemic, and describe the mechanisms responsible for COVID-19-associated coagulopathy. Finally, we discuss the impact of COVID-19 on ischemic stroke, focusing on large vessel occlusion.
- inflammation
- inflammatory response
- platelets
- stroke
- COVID-19
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Since January 22, 2020, the worldwide number of confirmed cases of coronavirus disease 2019 (COVID-19) is over 63 million with a resultant mortality of over 1.4 million. In the USA alone there have been more than 14 million cases and over 268 000 deaths (www.coronavirus.jhu.edu). Post-mortem histology of all organs studied in patients infected with SARS-CoV-2 demonstrated macrovascular and microvascular thrombosis in the arterioles, capillary bed, and venules consisting of platelets, fibrin, red blood cells, and leukocytes, supporting the fact that, rather than merely infecting the airway, SARS-CoV-2 induces a disease in the vasculature.
The primary reported cause of death is respiratory failure due to development of acute respiratory distress syndrome (ARDS). However, numerous studies have reported an increased incidence of both arterial and venous thrombosis contributing to disease severity. This outcome has included a rising incidence of stroke in younger patients or patients with no prior risk factors for stroke.1–5 Multiple risk factors associated with SARS-CoV-2 and the development of COVID-19 could contribute to the increased severity and earlier onset of acute ischemic stroke including generalized hypercoagulability, dysregulated immune response leading to cytokine-release syndrome, damage to endothelial cells leading to increased inflammation and thrombosis, dysregulation of the renin-angiotensin-aldosterone system, direct cytotoxic effect on the nervous system related to angiotensin converting enzyme-2 (ACE-2) receptor uptake of SARS-CoV-2 virus, hypoxemia related to cardiorespiratory failure, and metabolic derangements. The purpose of this review is to provide an overview of SARS-CoV-2 and the mechanisms related to the development of thrombosis that lead to the morbidity and mortality associated with COVID-19, including acute ischemic stroke.
Coronavirus and SARS-CoV-2
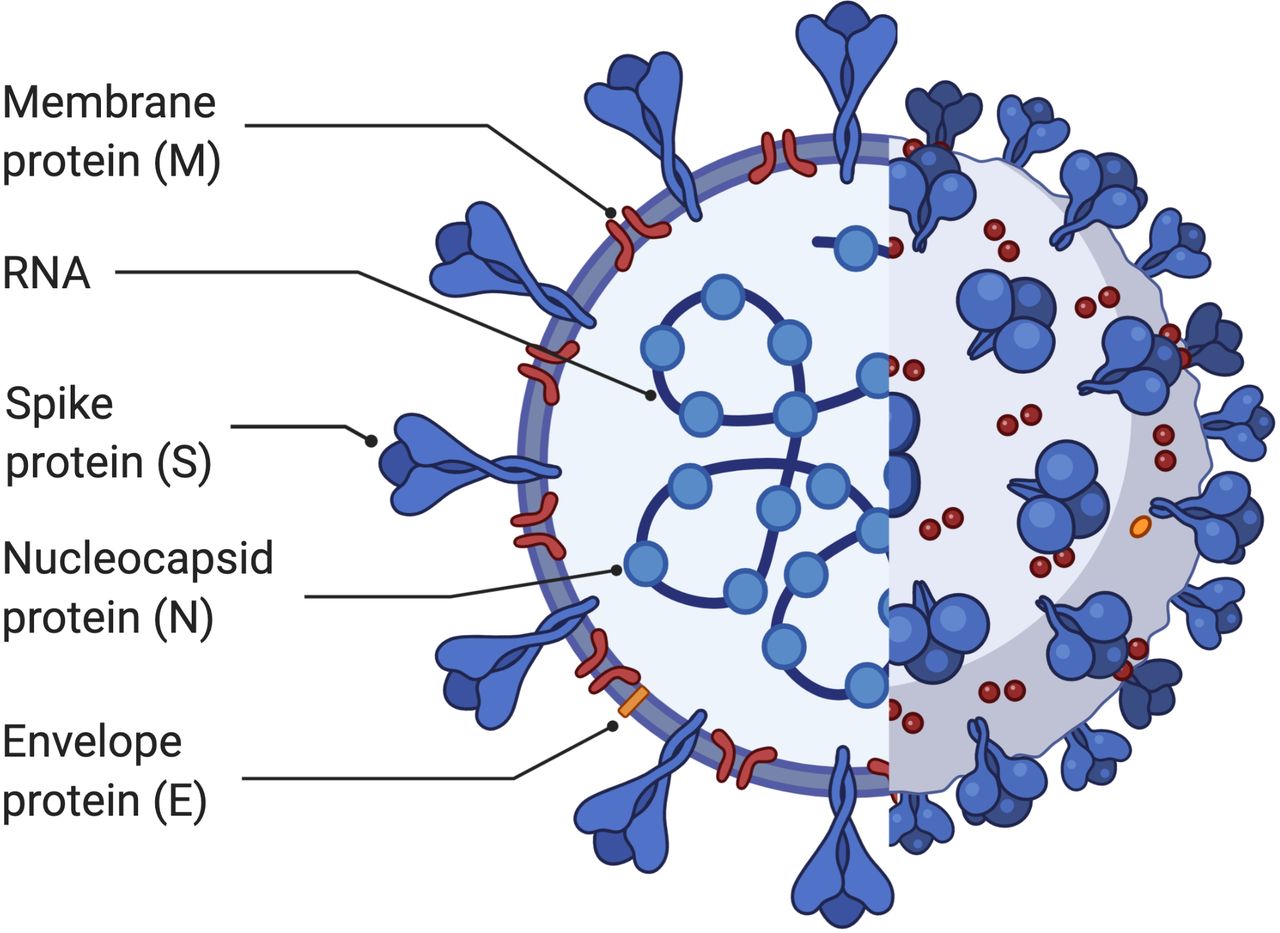
At least six coronaviruses exist that are known to infect humans including three beta coronaviruses: SARS, MERS, and now the new coronavirus SARS-CoV-2.6 Coronaviruses are enveloped positive-sense single-stranded RNA viruses. They have four key structural proteins including spike surface glycoprotein (S), membrane protein (M), envelope protein (E), and nucleocapsid protein (N) (figure 1). The S protein is used to initiate attachment to the host cell receptor and enables cell infection by the virus. In the case of SARS-CoV-2, the virus is thought to infect cells through the ACE-2 receptor and is also the main inducer of neutralizing antibodies.7

Structural elements of SARS-CoV-2. A member of the coronavirus family, this single-stranded RNA virus relies on the spike protein (S) to dock onto cells in order to infect its host.
Transmission of the virus is thought to occur through respiratory droplets via coughing and sneezing, as well as through aerosol transmission during prolonged exposure to aerosolized virus in closed spaces.8 There is an approximately 5.2 day incubation period9 during which time infected persons can continue to shed large amounts of virus. Infection with viral pathogens is known to induce tissue factor (TF) expression in lung epithelial cells, endothelial cells, and monocytes.10
COVID-19 and thrombosis
COVID-19 is the disease caused by infection with SARS-CoV-2. It has been associated with increased rates of both arterial and venous thromboses in the pulmonary vasculature and also systemically. Reported rates of arterial thrombosis range from 2.8% to 3.8%.10
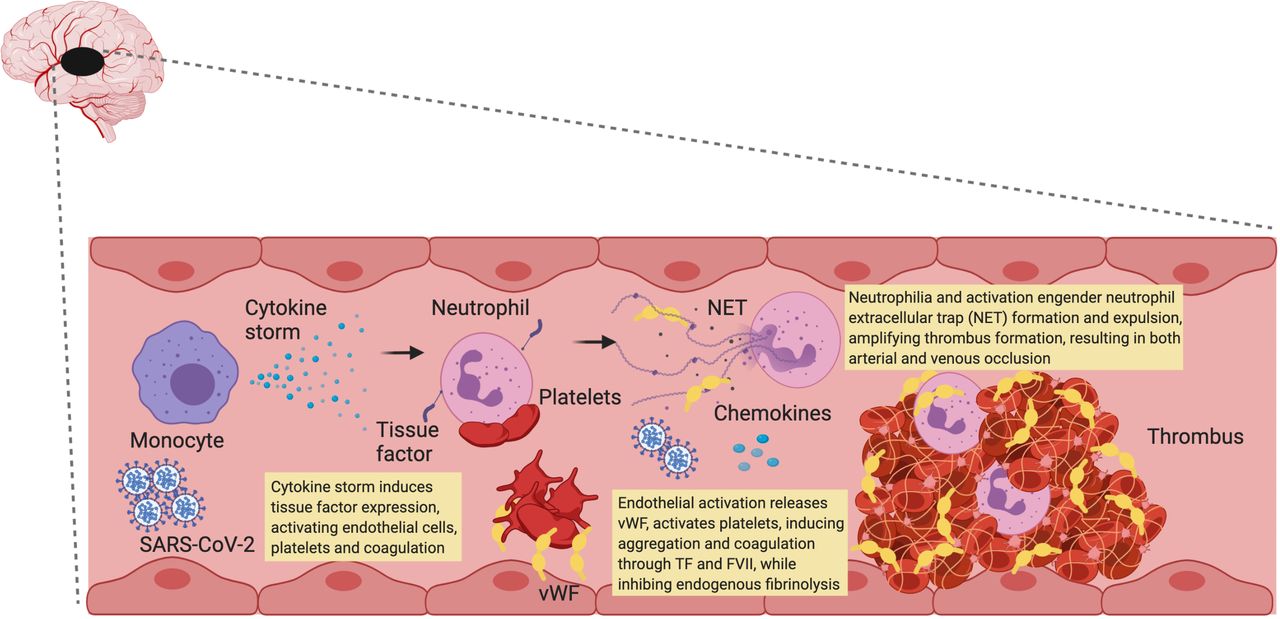
While numerous mechanisms of thrombosis have been proposed, general agreement is emerging that it begins with activation of the innate immune system in response to introduction of a viral pathogen. The term 'immunothrombosis' best describes the interaction between the innate immune system and thrombosis.11 It focuses on interplay between activation of intravascular TF, innate immune cells, platelets, endothelial cells, and releases neutrophil extracellular traps (NETs) which can activate the contact pathway of coagulation. This concept is a cornerstone for the main hypothesis underlying COVID-19-associated coagulopathy (CAC) (figure 2).11 12

{kind=link}
{kind=link}
Summary of COVID-19-associated coagulopathy (CAC). Viral infection activates monocytes, releasing a proinflammatory cytokine storm. This results in neutrophil recruitment and tissue factor (TF) activation. TF then binds to coagulation factor VII (FVII) activating coagulation. SARS-CoV-2 infection also induces an endotheliopathy, releasing von Willebrand factor (vWF) and activating platelets, which together further amplify coagulation. Persistent neutrophil recruitment promotes neutrophil extracellular trap (NET) formation which further facilitates thrombosis. NET formation and platelet aggregation both inhibit endogenous mechanisms of fibrinolysis including tissue factor pathway inhibitor (TFPI). These processes represent the best data describing CAC.
Cytokine storm
The likely initiating sequence of pathological thrombosis in patients with COVID-19 is a hyper-inflammatory response with resultant 'cytokine storm'.13 Patients with COVID-19 have elevated levels of both interleukin-6 (IL-6) and C-reactive protein.10 Moreover, IL-6 perpetuates the hypercoagulable state associated with COVID-19 through (1) induction of TF expression in mononuclear cells; (2) triggering acute endothelial cell activation, also resulting in expression of TF; (3) activation of acute phase response resulting in enhanced production of fibrinogen by hepatocytes; and (4) platelet hyperactivation and aggregation (figure 2).10 14
Tissue factor (TF) and the extrinsic coagulation pathway
Immune system activation and increased inflammatory cytokines at the site of infection lead to expression of TF on endothelial cells, as well as on infiltrating macrophages and neutrophils,13 resulting in increased concentrations of TF within the lungs. In TF-induced coagulation (extrinsic coagulation pathway), TF combines with factor VIIa to form the TF–factor VIIa complex enzyme which initiates blood coagulation by activating factor IX and X to factor IXa and Xa.15 Subsequent assembly of factor Xa into prothrombinase leads to conversion of prothrombin to thrombin, with thrombin activating fibrinogen to fibrin and finally the production of a fibrin-based clot as well as additional activation of platelets.16
Platelets and complement
Platelets play an integral role in the development of acute thrombus in COVID-19, both in the microvasculature and large vessels. During arterial thrombosis, platelet activation induces platelet expression of adhesion receptors, including P-selectin, as well as the release of chemokines that promote recruitment of innate immune cells.11 Platelets are also activated through mechanisms other than direct infection including inflammatory molecules, NETs, endothelial substrates including von Willebrand factor (vWF), and the endotheliopathy that has been demonstrated in COVID-19.
Endothelium
A central component to the prothrombotic state associated with COVID-19 lies within endothelial cell infection and disruption. This occurs through direct cytotoxic effects to endothelial cells as well as through endothelialitis, which have both been demonstrated in patients with COVID-19.17 Endothelial disruption leads to expression of activated TF on endothelial cells, excessive thrombin production, inhibition of fibrinolytic mechanisms, and activation of complement pathways.11 13 17–19 Patients with COVID-19 have elevations in vWF antigen in the plasma, with concentrations increasing in relation to disease severity.20
Factor VIII and vWF
Both vWF activity and factor VIII (FVIII) levels are generally increased secondary to endothelial cell activation, but the levels observed in CAC are 2–4-fold higher in COVID-19 patients than in healthy individuals.12 21 22 The potential role of vWF in contributing to the prothrombotic state associated with COVID-19 is also supported by the finding that patients who developed ARDS in the setting of SARS-CoV-2 had significantly elevated circulating levels of vWF antigen as well as vWF activity and FVIII.23
Neutrophil extracellular traps (NETs)
Neutrophils and monocytes are key components to the innate immune response but also contribute to the development of pathologic thrombosis in the setting of infection. One mechanism by which neutrophils localize and kill pathogens is through the development of NETs.24 NETs induce a significant procoagulant response and play a critical role in initiating and propagating arterial and venous thrombus formation (figure 2).11 25
Stroke and COVID-19
Initial reports of COVID-19 cases from China reported a high incidence of neurological manifestations, with rates of patients experiencing neurological symptoms reaching up to 36% and acute cerebrovascular disease occurring in up to 5.7% of patients with severe disease compared with 0.8% of patients with non-severe disease (p=0.03).4 Reported rates of cerebrovascular events ranged from 0.19% to 5.4% in one population study, with the rate of cerebrovascular events and acute ischemic stroke decreasing as the number of patients treated for COVID-19 increased.26 Other reports from Wuhan, China described a higher risk of poor outcomes associated with a history of stroke among infected patients, with increased rates of in-hospital mortality.27 In the USA, Yaghi et al provided the first study examining the rate of stroke among COVID-19-infected patients in New York and found that 0.9% of all patients hospitalized with COVID-19 experienced ischemic stroke, with 63.6% of these patients dying during their hospitalization.1 Importantly, the authors also found that cryptogenic stroke occurred twice as frequently in COVID-19-positive patients in comparison to COVID-19-negative patients (65.6% vs 30.4%, respectively).1 This increase in proportion of cryptogenic stroke as a mechanism of acute ischemic stroke was also noted by the largest population study performed to date, where cryptogenic stroke was also found to be the only independent predictor of mortality.26 It was proposed that COVID-19-associated cryptogenic stroke represented a unique stroke mechanism associated with a higher probability of early mortality.26 Other initial studies from New York, Italy, and Barcelona have described patients with COVID-19 experiencing both stroke and large vessel occlusion (LVO) at a younger age than is usually seen.3 28–30 Furthermore, three studies have found COVID-19 infection to be an independent risk factor for both acute ischemic stroke and LVO.31–33
The COVID-19 paradox
In contrast to what was anticipated with the rapid spread of a pandemic virus associated with prothrombotic complications, many cities experiencing the greatest incidence of COVID-19 cases actually found a significant decrease in the number of new stroke alerts, diagnoses, and admissions.30 34–37 Across China there was a decrease in the absolute number of thrombolysis and thrombectomy treatments, yet the overall rate of these therapies actually increased, suggesting that the absolute decline was related to the overall decline in stroke admissions.36 In addition, an increase in proportion of LVOs despite an overall decline in stroke diagnoses has been described.34 Aguiar de Sousa et al propose five reasons why stroke rates are thought to have declined in paradox to expected complications related to COVID-19.37 These include: fear of infection leading patients with milder symptoms to stay home, increased social isolation preventing the identification of stroke symptoms in elderly patients by family members, overwhelmed emergency medical services resulting in reduced activation of stroke codes, COVID-19 illness itself precluding the correct identification of stroke symptoms, and decline in stroke incidence due to environmental or behavioral changes.37
Mechanisms of stroke in COVID-19
Many mechanisms for ischemic stroke in the setting of COVID-19 infection have been proposed, including the relationship of severe COVID-19 disease occurring more frequently in older patients who are more likely to have multiple comorbidities increasing their risk of stroke. However, this is undermined by the findings outside of China suggesting that COVID-19-positive patients presenting with LVO had lower rates of pre-existing cardiac comorbidities and were actually younger than their COVID-19-negative counterparts.2 29
Rather than a single pathway to explain COVID-19-associated stroke, there is an interplay of the proposed mechanisms which would account for the heterogeneity that is being reported in the literature across centers. The key proposed mechanisms include the development of cytokine storm and activation of the innate immune system, embolic events propagated by pre-existing or new-onset arrhythmias, hypoxia-induced ischemia secondary to severe pulmonary disease, thrombotic microangiopathy, endotheliopathy/endothelialitis, and multifactorial activation of coagulation. The hypothesis that COVID-19 contributes to stroke risk differently depending on severity of illness, with patients with more severe illness experiencing a higher risk of stroke, is supported by the findings that stroke occurred in 5.7% of patients with critical illness in comparison to 0.8% of patients with milder COVID-19 disease.4
One unifying factor that seems to exist among the currently published literature is elevated D-dimer levels among COVID-19-infected patients experiencing acute ischemic stroke, suggesting activation of the coagulation and innate immune system.1 2 5 29 38 Among COVID-19-positive patients in New York presenting with emergent LVO, more than 90% had elevated D-dimer levels and 42% presented with symptoms of acute ischemic stroke rather than typical respiratory symptoms.29 In addition, patients presented with stroke days before demonstrating symptoms of COVID-19, suggesting that there may be an increased risk of thrombosis even in the early phase of the disease.5 39 A recent review found a consistent increase in D-dimer levels among patients with severe compared with non-severe COVID-19 disease.39 It is likely that, while D-dimer levels appear to be more significantly elevated among patients with severe disease and stroke appears to occur more frequently in severely ill COVID-19-infected patients,4 they may also be elevated with less severe COVID-19 infection.
Another consideration is the role of a cytokine storm resulting in elevated levels of both IL-6 and C-reactive protein, which have been associated with an increased risk of both stroke and myocardial infarction when elevated in healthy individuals.40 The expression and viral uptake of ACE-2 receptor may represent a twofold mechanism by which COVID-19 increases the risk of stroke. First, direct infection of brain endothelium, which expresses ACE-2 receptor, could pose a risk of viral-induced vasculitis.41 Second, ACE-2 receptor inhibition or depletion through viral infection and endocytosis on cell entry could result in reduction of ACE-2 function, thereby decreasing the formation of angiotensin (1–7) and impairing cerebral vascular autoregulation.2 42 Finally, the hypoxia ensuing from severe COVID-19 pulmonary infection could also contribute to an increased risk of stroke through reduced oxygen delivery.
COVID-19 and stroke: patient subgroups
Patients who present with new onset stroke in the setting of COVID-19 likely represent several discrete groups of individuals. First, there is likely a subset of patients who present with stroke in the setting of otherwise asymptomatic or mild COVID-19. In this group, COVID-19 per se may not be contributory to the stroke—for example, patients with pre-existing risk factors for stroke such as atrial fibrillation, intracranial atherosclerotic disease, or extracranial carotid artery disease who do not experience severe COVID-19. An alternative theory, that may also contribute to this group, proposes that viral involvement of the vascular endothelium may contribute to an increased risk of thrombus formation in otherwise healthy patients resulting in a higher risk of stroke among patients with otherwise mild or asymptomatic COVID-19.43 Additionally, there are likely patients with COVID-19 who develop accompanying symptoms that may increase the risk of hypercoagulability (ie, dehydration). A third group with severe disease in which COVID-19-related pathology directly increases the risk of stroke by creating a hypercoagulable state (thereby leading to thrombus formation) and/or disrupting the local endothelium, predisposing to both thrombus formation and degradation of vessel integrity, with potential for accompanying hemorrhagic complications. The majority of this third group is likely to be represented by patients with severe disease who develop pneumonia or ARDS. In this setting, there is likely activation of platelets and clotting as well as impaired arterial dilatation and hypoxia, thereby creating a prothrombotic milieu which increases the propensity for stroke.39 As reports continue to gather around LVO stroke in patients diagnosed with COVID-19, trends are beginning to appear that may affect outcome. Age, sex, race, and comorbidities as biological variables in patients with LVO stroke have been reported in multiple studies. Table 1 provides a summary of case series that have reported demographic information, comorbidities, and outcomes in COVID-19-infected patients who develop LVO stroke.1 3 29 44–50
Case series of COVID-19-infected patients presenting with LVO
Treatment of acute ischemic stroke in COVID-19
Thromboprophylaxis
Treatment paradigms to prevent ischemic stroke have largely been maintained with those of pre-COVID times, yet there is a paucity of data to support an ideal medical treatment regimen for patients presenting with acute ischemic stroke or to prevent acute ischemic stroke among hospitalized patients with COVID-19. This is underscored by one study that found admitted patients with COVID-19 were experiencing acute ischemic stroke in spite of therapeutic anticoagulation.5 Table 2 provides an overview of current antiplatelets and anticoagulants used, their mechanism of action, and proposed mechanism to mitigate CAC. It remains unclear whether anticoagulants or antiplatelet agents provide superior primary or secondary stroke prevention in patients with COVID-19. In particular, given the concern for activation of the TF-dependent pathway of coagulation, further trials could evaluate the efficacy of anticoagulation in preventing stroke in the setting of COVID-19. One recent case report of patients with mild COVID-19 experiencing macrothrombosis and stroke used apixaban 5 mg twice daily in one patient and enoxaparin 1 mg/kg every 12 hours in another patient, both with non-occlusive thrombus involving the internal carotid artery, and found near complete and complete resolution of the thrombus at 10 and 7 days following presentation, respectively.43 This is not to say that anticoagulation is appropriate for all stroke patients, particularly given that anticoagulation was identified as an independent risk factor for intracranial hemorrhage in patients with COVID-19.51 Instead, it highlights the need to direct future studies at evaluating the role of anticoagulants in treating acute ischemic strokes in COVID-19-positive patients who are not eligible for currently recommended therapies (eg, recombinant tissue plasminogen activator (rtPA) or thrombectomy). Gavioli et al have published a proposed clinical treatment pathway for hospitalized COVID-19 patients which guides treatment with prophylactic versus therapeutic heparin and enoxaparin as well as rtPA in hospitalized patients with COVID-19.52 In particular, for hospitalized patients with severe disease or elevated D-dimer, low molecular weight heparin appears to be associated with a better prognosis than other anticoagulants.53 54 Yet, the role of platelet hyperactivity through platelet activation/propagation of platelet aggregation via the inflammatory and immune response could support the idea that use of antiplatelet agents may represent a more beneficial treatment strategy. Other theories suggest that treatment of the underlying hyperinflammatory state with the use of immune modulating therapies may act synergistically with antithrombotic or antiviral therapies by treating the underlying cause of thrombosis in patients with severe disease. One final consideration is the use of 'targeted' COVID-19 therapy aimed at ACE-2 and the renin-angiotensin-system in patients with ARDS.42
Antithrombotic agents and potential mechanisms of mitigating CAC
Intravenous thrombolysis
Current international guidelines recommend intravenous thrombolysis for selected patients who can be treated within 3 hours and highly selected patients who can be treated within 3–4.5 hours of symptom onset.55 This recommendation comes with the caveat that patients with COVID-19 have been found to have a high prevalence of elevated concentration of inflammatory and hypercoagulability markers, which have been associated with increased risk of death or disability and post-thrombolytic intracranial hemorrhage among patients with acute ischemic stroke but without COVID-19 infection.55 The authors recommend evaluation of both liver function and coagulopathy to aid in assessment of risk/benefit profile prior to rtPA administration.55
Anesthesia for mechanical thrombectomy
With regard to mechanical thrombectomy, it is recommended to maintain current clinical guidelines for inclusion criteria and employ appropriate precautions including use of personal protective equipment for all persons within the angiography suite.55 A consensus statement from the Society for Neuroscience in Anesthesiology and Critical Care has proposed criteria to better identify patients as candidates for general anesthesia versus monitored anesthesia care.56 While many centers adapted a policy of intubating every patient prior to mechanical thrombectomy, preliminary data have suggested that the use of general anesthesia and intubation resulted in increased door to reperfusion time (138 vs 100 min, P<0.001) and was associated with a higher probability of in-hospital mortality (RR 1.871, P=0.029) as well as a lower probability of functional independence at discharge (RR 0.53, P=0.015).57 This is in contrast to prior studies which have found no difference in long-term outcomes between patients undergoing mechanical thrombectomy with general anesthesia in comparison to monitored anesthesia care.58 59 Interestingly, COVID-19 status was not associated with statistically significant in-hospital mortality or functional independence, although approximately half of patients were not tested and discharge modified Rankin Scale score was not available for 57 (23.6%) patients.57 For patients who require general anesthesia, it is recommended that patients are intubated in a negative pressure room, which may involve intubation in the emergency department prior to transport to the angiography suite.55 The findings of Al Kasab et al suggest that we may need to be more judicious in our use of general anesthesia, or work closely with our emergency department colleagues to develop protocols which enable rapid intubation and do not significantly delay time to reperfusion.
Conclusion
Understanding the interplay between COVID-19 and the cerebrovasculature is critical in guiding the management of this complex patient population that has rapidly emerged and bears daily relevance to the practicing neurointerventionalist. Future studies should aim to determine which patients benefit most from prophylactic and therapeutic anticoagulation and better delineate the role of platelet activation in COVID-19 infection. Longitudinal follow-up of patients receiving general anesthesia versus monitored anesthesia care may provide insights into the effects of anesthesia on patients undergoing mechanical thrombectomy with future practice implications.
References
Footnotes
Contributors AZ contributed to drafting and revising the manuscript. APJ contributed to the conception, drafting, and revising the manuscript. BAS contributed to the conception, drafting, and revising the manuscript. SMN contributed to conception, research, drafting, and revising the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.