Article Text

Abstract
Background Recently, liquid embolic agents have emerged for the endovascular treatment of cerebral aneurysms. Here we describe the in vivo performance of a novel liquid embolization agent (GPX Embolic Device).
Methods Elastase-induced aneurysms were embolized with a GPX prototype under balloon assistance. Digital subtraction angiography was performed pre-deployment and immediately after, and at 5, 10, and 30 min post-deployment in 10 rabbits and at 1 month in 8 rabbits. The early post-deployment intra-aneurysmal flow was graded as unchanged, moderately diminished, or completely absent. At 1 month the status of aneurysm occlusion was evaluated. Adhesion to catheter material and migration of GPX was assessed.
Results The mean aneurysm neck diameter, width, and height were 3.6±1.0 mm, 3.0±0.8 mm, and 7.4±1.4 mm, respectively. The mean dome-to-neck ratio was 0.9±0.2. Complete stagnation of intra-aneurysmal flow was observed in 9 of 10 aneurysms (90%) within 30 min of device deployment. One aneurysm showed moderately diminished intra-aneurysmal flow at 30 min. At 1 month, 8 aneurysms were completely occluded. There was no evidence of GPX adhesion to the catheter material. Histologically, a leukocyte and foreign body reaction to GPX was detectable 28 days after embolization.
Conclusions This is the first preclinical study reporting the performance of a protype version of the GPX Embolic Device in a wide-neck aneurysm model. GPX showed promising results by achieving and maintaining high rates of complete angiographic occlusion, but may induce an inflammatory reaction.
- aneurysm
- angiography
- embolic
- liquid embolic material
- balloon
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Endovascular techniques for the treatment of aneurysms are increasingly used in a variety of both ruptured and unruptured aneurysms. Through larger studies (International Subarachnoid Aneurysm Trial and Barrow Ruptured Aneurysm Trial) with long-term observations of up to 18 years, the survival advantage after endovascular treatment of a ruptured aneurysm, despite the persistence of an increased risk of recurrent bleeding, could be confirmed.1–5 Updated versions of Guglielmi detachable coils have been developed in recent years. However, limitations have been identified, including incomplete packing and coil compaction, that can lead to recurrent aneurysms followed by possible re-rupture with poor prognosis.6 7 The coil mesh often shows low stability over time in large aneurysms, particularly for those with a high dome-to-neck ratio.8–10 For acute treatment of a ruptured intracranial aneurysm, stent-assisted coiling and flow diverter implantation are effective in treating wide-necked aneurysms, but these methods require antiplatelet medication which has proven to correlate with increased risk of procedure-related complications including in-stent thrombosis and re-rupture.11 12 Novel flow disruption devices such as WEB,13 Contour,14 or Luna15 have gained more and more use in the neurointerventional field for treatment of ruptured and unruptured aneurysms. Research into the ideal endovascular device to produce reliable, stable occlusions for aneurysms is ongoing. To permanently isolate the weakened vessel wall from blood flow, and therefore stabilize the aneurysm in the long-term, the filling material should incorporate the aneurysm and induce an endothelial layer as well as neointima proliferation along the aneurysm neck.16 17 Preclinical in vitro18 and in vivo19 studies showed that optimal coverage of the aneurysm neck is a critical component in reducing intra-aneurysmal flow. Through advances in technology and materials, new generations of embolic agents have been developed that address the limitations of clinically used agents. For example, the novel GPX Embolic Device (Fluidx Medical Technology, Salt Lake City, UT) is composed of a concentrated polyelectrolyte solution that is produced using a blend of oppositely charged polymers. The sodium and chloride counterions of these polymers prevent their interaction before material delivery. This composition allows the GPX to be delivered in a fluid state and to solidify in response to the lower concentration of monovalent ions in the blood and surrounding tissues. Tantalum metal powder is added for radiopacity and is trapped in the polymer matrix. The purpose of this study was to assess the efficacy of GPX by evaluating the occlusion rate and the tissue response in a rabbit elastase aneurysm model.
Materials and methods
The GPx embolic device
The GPX Embolic Device has two viscosities in development: GPX-HV is designed for more proximal occlusions of larger vessels and can be used in catheters with internal diameters >0.024 inches; GPX-LV is a lower viscosity version that is designed for deep distal penetration and embolization of very small vessels. The latter can be used with catheters with internal diameters ≥0.016 inches. For this study, Fluidx Medical Technology provided an early prototype version of GPX-LV.
Aneurysm creation and embolization
All experiments were approved by the local institutional animal care and use committee (approval no. 18/2020). One saccular aneurysm with a mean dome-to-neck ratio of 0.9±0.2 mm was created in each of 10 New Zealand white rabbits (weight 3.8–4.6 kg) at the origin of the right common carotid artery. Aneurysm creation procedures were performed using the method reported by Altes et al.20 Embolization with GPX was performed at least 3 weeks after aneurysm induction.21 Under general anesthesia, the right femoral artery was surgically exposed and a 5F sheath was inserted. During the entire procedure, a total of 300 units of heparin were administered intravenously. Using a 4F diagnostic catheter (Glidecath; Terumo Europe, Leuven, Belgium), angiography of the aneurysm-harboring vessel was performed to assess the aneurysm morphology. A 0.017 inch microcatheter (Echelon 10; Medtronic, Minneapolis, MN) was advanced in the sac of the created aneurysm with a jailing technique using a 0.014 inch microwire. A non-compliant balloon (Aviator 4×20 mm; Cordis, CA) was then placed across the neck of the aneurysm (figure 1) in the brachiocephalic trunk and inflated with a mixture of 50/50 contrast media and 0.9% saline under fluoroscopy. A control angiogram obtained through the Echelon 10 microcatheter confirmed the occlusion of the aneurysm neck through the balloon. The GPX Embolic Device was prepared as recommended: two preconnected 1 mL syringes containing GPX were removed from the packaging, then GPX was mixed by pushing the opposing plungers and moving the material from one syringe to the other 25 times. After preparation, the GPX was slowly injected into the aneurysm under roadmap guidance, until satisfactory embolization was achieved. GPX was injected at a rate of 0.1–0.2 mL/min, and the injection time ranged between 2 and 5 min. The balloon was constantly inflated during the injection period in all cases. We aimed for complete occlusion of the aneurysm as visible on the road map. If migration of GPX was detected, the injection was terminated immediately and was not continued. After deflation of the balloon, the microcatheter and balloon were removed 3 min after termination of the embolic injection. The 4F diagnostic catheter was again advanced into the aortic arch and control angiograms were obtained after embolization to evaluate the occlusion rate and migration/protrusion of GPX into the parent artery. Catheters and wires were removed, and the femoral artery was ligated. At 28 days after GPX embolization, the animals were re-anesthetized and a 5F introducer sheath was inserted after surgical exposure of the left femoral artery. Digital subtraction angiography (DSA) of the aortic arch was performed to evaluate aneurysm occlusion. All animals were euthanized immediately afterwards by an overdose of sodium pentobarbital. Aneurysm and parent artery tissue with the implanted devices were surgically removed and fixed in a 4% solution of buffered formalin.

Angiograms demonstrating the embolization procedure. Angiogram of an aneurysm (A) before embolization with liquid embolic agent. A microcatheter is placed in the aneurysm and a balloon is positioned over the neck. A contrast agent is injected through the microcatheter before balloon inflation to assure adequate positioning of the catheter (B). Unsubtracted angiogram (C) shows low opacity of the aneurysmal sac (dashed arrows) due to the embolic agent, immediately after embolization. Angiogram at 28 days follow-up (D) shows complete occlusion of the aneurysm.
Data analysis
Angiographic evaluation
Baseline aneurysm characteristics that were analyzed included the parent vessel diameter as well as the aneurysm neck, height, width, and dome-to-neck-ratio.
DSA was performed before embolization and immediately after, and then 5, 10, and 30 min after embolization in 10 rabbits and at 1 month in eight rabbits. The early post-embolization intra-aneurysmal flow was graded as unchanged, moderately diminished, or completely absent. At 1 month, the status of aneurysm occlusion was graded using a 3-point scale (complete, near-complete, or incomplete occlusion). Adhesion to catheter material and migration/protrusion of GPX into the parent artery were assessed.
Histopathologic processing and analysis
A part of the aneurysm and parent artery tissue without the implanted device were embedded in paraffin. For histological analysis, 1–3 µm slides were stained with hematoxylin and eosin (H&E), elastic Verhoeff-van Gieson stain, and Prussian blue. All sections were prepared, viewed, and analyzed by an experienced neuropathologist (WSS). Samples were scored by determining whether a thrombus was visible, the GPX embolus was detectable, and a physiological reaction to GPX was observed.
Results
Angiography
Aneurysms were successfully induced in all animals. The mean aneurysm neck diameter, width, and height were 3.6±1.0 mm, 3.0±0.8 mm, and 7.4±1.4 mm, respectively. The mean dome-to-neck ratio was 0.9±0.2. All aneurysms were successfully embolized. In nine of 10 aneurysms (90%), complete stagnation of intra-aneurysmal flow was observed immediately and within 30 min of device deployment. In one case (10%) the aneurysm showed moderately diminished flow due to distal migration of the GPX that was still connected to the intra-aneurysmal embolic sample in all post-embolization control angiograms (up to 30 min). Apart from that, we did not observe distal thrombus migration angiographically. We did observe some resistance during the injection of GPX within the Echelon 10 microcatheter, but sufficient injection was maintained in every case. There was no resistance during removal of the microcatheter at the end of the GPX injection. No adhesion of GPX to the catheter or the balloon was found. Two animals, including the one where migration of GPX was observed, died due to narcosis after all early control angiograms were obtained. We observed varying visibility with this first generation GPX prototype when injected through a 0.017 inch microcatheter within the aneurysm sac (compare figure 1B with figure 2B and figure 3C).

Representative study results for testing the GPX embolic agent in a rabbit aneurysm model. Angiogram of an aneurysm (A) before embolization with liquid embolic agent. Unsubtracted angiogram (B) shows adequate opacity of the aneurysmal sac (dashed arrow) due to the embolic agent immediately after embolization. Subtracted angiogram (C) shows complete occlusion of the aneurysm at follow-up (28 days).
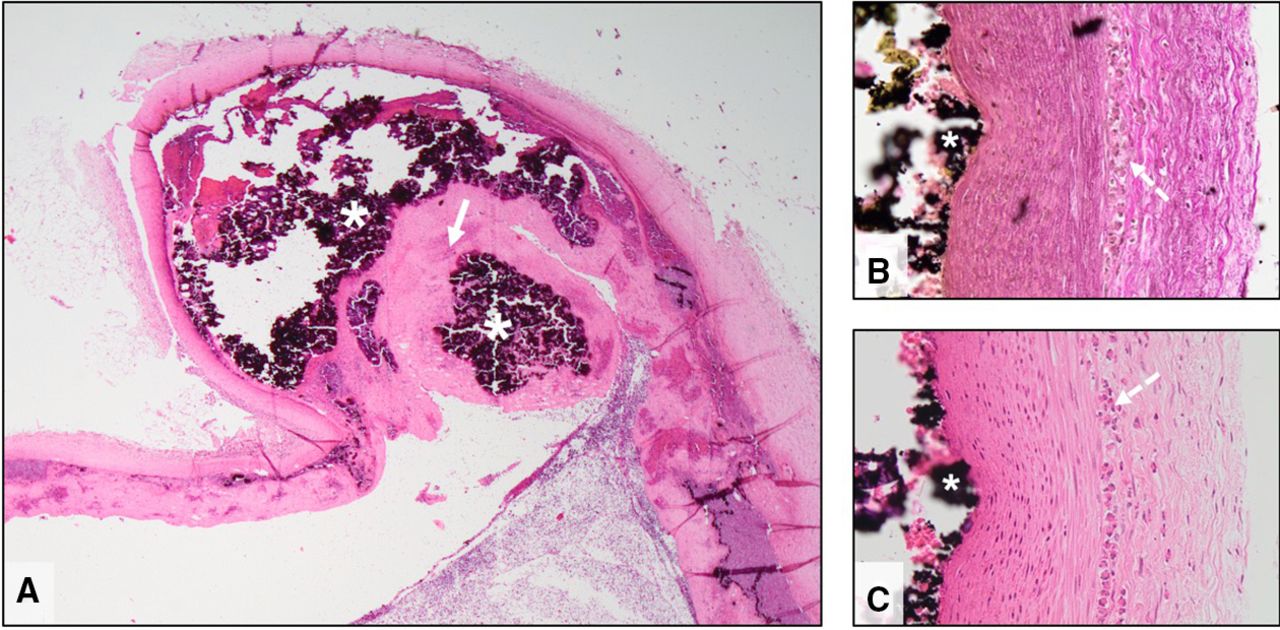
Microscopic images of an aneurysm treated with GPX liquid embolic agent. GPX (asterisk) is located in the aneurysm sac (A). Note the large endothelialized thrombus formation covering the aneurysmal neck (solid arrow). Images of the aneurysmal wall (B,C) showing GPX at the surface of the tunica intima (asterisk). Leukocyte infiltration (dashed arrows) in the tunica adventitia at the border to the tunica muscularis was present at 28 days. Note the preparation artefacts inside the vessel lumen (white areas) caused by dissolving of the embolic agents during histopathological preparation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Microscopic images show the junction (white dashed arrows) of the GPX liquid embolic agent with the arterial wall (A) and aneurysm wall (B). Organized fibrinous thrombus (arrowheads) was seen within the embolic agent cast (black areas). In (B) the edge of the thrombus (arrowheads) is connected to the aneurysm wall (white hashtag) and covered by neoendothelium (arrows) adjacent to the lumen of the parent vessel (black hashtag). Note the formations of leukocytes (asterisk) close to the embolic agent.
At 1 month, in the remaining eight rabbits, all aneurysms (100%) were completely occluded (figure 2). There were no cases of near-complete or incomplete occlusion. There was no thrombosis or GPX visible in the parent vessels at 1 month. We did not observe any health problems in the remaining eight rabbits.
Histology
Histopathological findings are illustrated in figures 3 and 4. The embolic agent was identified as amorphous, disintegrated material of black appearance. After 28 days the embolized aneurysms were filled with a mixture of GPX and fibrin accompanied by thrombus attached to the vascular lining (figures 3A,B and 4). Neoendothelialization of the thrombus was found in all samples. Signs of inflammation were present, represented by leukocyte infiltration of the vessel wall (figure 3B,C) next to the embolic agent. No necrosis was evident. In one of the samples a group of giant cells was found in the media of the vessel wall which indicated a foreign body reaction. The giant cells did not contain material of GPX. Recanalization of the embolized aneurysms was not observed in the analyzed samples.
Discussion
The past few decades have seen a gradual shift from open surgery to endovascular therapies for the treatment of both ruptured and unruptured aneurysms in the USA.22 Although coils are the archetypical device for endovascular aneurysm treatment and provide a safe and effective therapy for many aneurysms, wide-necked and large or giant aneurysms are still a major challenge. In addition, Fujiwara and Kallmes23 found that coil embolization led to occasional coil compaction in one of 17 cases (6%) and Dai et al 24 found this to occur in three of 18 cases (17%), both using the same animal model.
As neurointervention continues to evolve, a large variety of new and improved aneurysm treatment devices have been developed, such as extra-aneurysmal flow diversion (eg, Pipeline, FRED, and DERIVO) or intra-aneurysmal flow diversion (eg, WEB and Luna), to address different clinical scenarios and aneurysm configurations. Interest in liquid embolic agents has increased because these agents do not depend on the individual patient’s ability to coagulate and can penetrate into areas where catheters and coils are not accessible for peripheral procedures.25 For example, they can provide embolization distal to the catheter tip and therefore treat hemorrhaging that cannot be reached with a catheter. A major advantage is that they can fully occlude aneurysms regardless of their configuration, with potentially high occlusion rates and low risk of recanalization. While fluid embolic agents like Onyx are mainly used for the treatment of arteriovenous malformations in the cerebrovascular system, they also appear to be a promising alternative treatment method for aneurysms of the distal posterior circulation,26–28 large or giant aneurysms,29 or mycotic aneurysms.30 However, several problems have been encountered, such as adhesion to catheters and vascular walls, complicated handling, and toxicity to living tissue.31 32 Liquid embolics are irreversible once injected whereas detachable coils and other devices can be repositioned. Tortuous anatomy may also preclude the delivery of a balloon across the aneurysm neck, or potentially of achieving a tight seal so that no liquid embolic can escape the aneurysm lumen. In addition, balloon occlusion for prolonged periods should be avoided because it is not tolerated in all patients for several minutes without transient or potentially permanent deficits, specifically not in the distal circle of Willis due to lack of collateral flow. Furthermore, liquid embolics are not ideal for aneurysms with perforating arteries at or close to the aneurysm neck.
Liquid embolic agents differ in their induction of beam hardening artifacts, which may be of clinical relevance in CT or MRI follow-up examinations. While Squid induces fewer beam hardening artifacts than Onyx on CT and flat panel CT acquisitions,33 it would be interesting to compare these results with the artifacts induced by GPX in future studies.
Regarding aneurysmal occlusion, our results with GPX in a rabbit elastase model are comparable with the preclinical16 and clinical27 30 studies using Onyx. However, Struffert et al 16 observed a higher rate of distal migration of Onyx (three of nine cases) in the same aneurysm model using compliant balloons. In one of these cases, total occlusion of the parent vessel was seen. In surgically constructed rabbit aneurysms, Suh et al 34 achieved complete embolization in five of eight aneurysms treated with glue (N-butyl 2-cyanoacrylate) only. However, in two of these cases they experienced occlusion of the parent vessel while withdrawing the microcatheter from the aneurysm. A higher aneurysmal occlusion rate was only achieved with a combination of glue and coils. Berenstein35 created bifurcation and sidewall (lateral) aneurysms in five dogs and achieved high aneurysmal occlusion rates (100% of intended aneurysms) by using a new liquid embolic agent (PHIL 35) in combination with a retrievable stent (FRED). They did not see any distal embolization or migration of the embolic agent after performing transient stenting. However, this study was done using an adjuvant device in a small number of animals so results may not be comparable. Similarly, the use of GPX with protective stents and/or coils could be used to improve outcomes.
GPX has several major advantages compared with commonly used liquid embolic agents like Onyx, glue, PHIL, Squid, or the novel liquid embolic agent Menox, which offers similar technical and clinical results in the endovascular treatment of arteriovenous malformations in comparison with the other currently available liquid embolic agents.36 First, GPX does not rely on precipitation with dimethyl sulfoxide (Onyx, PHIL, Squid, Menox) or in situ polymerization (glue). Due to its water-based composition, no specialized catheters or catheter pre-flush are needed, in contrast to Onyx, PHIL, Squid, and Menox which require dimethyl sulfoxide, and glue which requires D5W. Additionally, the minimized preparation steps (mixing back and forth between two syringes) are a significant advantage compared with Onyx, Squid, and Menox as these agents must be vortexed for 20 min before use. Meanwhile, glue requires a complicated multistep preparation, often involving a separate sterilized area to avoid premature polymerization. However, we experienced varying resistance and visibility with this first generation GPX prototype when injected through a 0.017 inch microcatheter. These observations were communicated to the company resulting in changes to the formulation of GPX, including adjusted viscosity.37 38 Angiographically, we did not see any fragmentation of GPX. Concerning the rabbit with distal migration of GPX that was still connected to the intra-aneurysmal embolic sample, we cannot exclude the possibility that microembolization or distal embolization of the migrated portion contributed to the death of the animal at the end of the narcosis. Additionally, flushing the catheter with hypertonic saline into a confined aneurysm space before product deployment may have slowed the solidification of the product. This step has since been removed from directions for using the product.
In the experimental series presented here, a leukocyte reaction to GPX was detectable 28 days after embolization. The cause and resolution remain unclear at this early phase of testing. However, inflammatory reactions and even necrosis have been observed within the first weeks after arteriovenous malformation embolization in clinical practice.39 40
Jones et al 37 38 observed progressive tissue remodeling in their preclinical study using GPX in a domestic swine model, which was largely resolved by 180 days (unpublished data). They did not note localized or systemic adverse effects in the animals. Therefore, these data suggest that further studies should be conducted to determine whether physiological reactions to GPX dissipate over longer time periods in rabbit and other models, and these studies should incorporate updated and advanced versions of the GPX embolic agent. Further effects of GPX next to the aneurysm wall will need to be examined over a longer period of time, given the possibility of inflammatory reactions that may thin the vessel wall and potentially result in aneurysm rupture. In addition, the observed foreign body reaction and its incidence would need further investigation, as this could potentially result in vasogenic edema and if in the brain, may be symptomatic.
Limitations
Distal embolization remains one of the main risks of liquid embolic agents. The use of compliant balloons in our study could have led to better prevention of any distal migration. For cost reasons, we used non-compliant balloons. Further limitations of this study are the limited number of animals and the two deceased rabbits during narcosis. Distal embolic material was assessed angiographically only. To better identify distal microembolization, end-organ examination for microscopic particles might have been useful. Longer observation periods (90 or 180 days) would be necessary to see any histologic evidence of further thrombus organization and neoendothelialization across the aneurysm neck.
Conclusions
Embolization of aneurysms with the GPX Embolic Device is technically feasible with neck protection of the flow with a balloon. GPX occluded aneurysms in a stable and durable condition for the 1 month observation period. However, we observed an inflammatory reaction in the treated vessel and aneurysm wall that was likely induced by the liquid embolic agent. Future long-term studies are warranted with an updated version of the device.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information.
Ethics statements
Patient consent for publication
Ethics approval
Approval from the institutional animal care committee was obtained from the Ethikkommission der Ärztekammer des Saarlandes, No 18/2020.
Acknowledgments
We would like to thank the Head of the Institute of Experimental Surgery Prof Dr Micheal D Menger and his team, for supporting this study. We would like to thank Fluidx Medical Technology (Salt Lake City, UT, USA) for providing the endovascular materials.
References
Footnotes
Contributors Study design: RM-B, FF, and WR. Data acquisition: FF, RM-B, TT, UY, AS, and MK. Literature research: FF and RM-B. Data analysis and interpretation: FF, RM-B, TT, UY, and WJS-S. Manuscript preparation: FF, RM-B and TT. Revision of manuscript for important intellectual content: UY, WR, and JJ. Approval of final version of the manuscript: all authors.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JJ is an engineer at the company Fluidx Medical Technology (Salt Lake City, UT, USA) and served as a proctor during this study.
Provenance and peer review Not commissioned; externally peer reviewed.