Article Text

Abstract
Background Venous sinus stenting (VSS) is a safe, effective, and increasingly popular treatment option for selected patients with idiopathic intracranial hypertension (IIH). Serious complications associated with VSS are rarely reported.
Methods Serious complications after VSS were identified retrospectively from multicenter databases. The cases are presented and management strategies are discussed.
Results Six major acute and chronic complications after VSS were selected from a total of 811 VSS procedures and 1466 venograms for IIH. These included an acute subdural hematoma from venous extravasation, cases of both intraprocedural and delayed stent thrombosis, an ultimately fatal cerebellar hemorrhage resulting in acute obstructive hydrocephalus, venous microcatheter perforation during venography and manometry, and a patient who developed subarachnoid hemorrhage and subdural hematoma after cerebellar cortical vein perforation. The six cases are reviewed and learning points regarding complication avoidance and management are presented.
Conclusion We report on six rare, major complications after VSS for IIH. Familiarity with these potential complications and appropriate timely management may allow for good clinical outcomes.
- stent
- complication
- vein
Statistics from Altmetric.com
Introduction
Idiopathic intracranial hypertension (IIH), previously referred to as pseudotumor cerebri, is a disorder characterized by headaches, pulsatile tinnitus, papilledema, vision loss, and elevated intracranial pressure (ICP) on lumbar puncture without an intracranial mass on imaging.1 Venous sinus stenting (VSS) has emerged as a safe and effective treatment option for patients with refractory IIH with associated venous sinus stenosis.2 3 Meta-analyses have suggested roughly 90% improvement in papilledema, 80% improvement in visual symptoms, and 80% improvement in headache,4–9 with major complication rates ranging from 1–7%.5–10 The literature offers limited guidelines or recommendations for patient selection or treatment for IIH.11 Major complications including subdural hematoma (SDH), subarachnoid hemorrhage (SAH), intracerebral hemorrhage (ICH), intraventricular hemorrhage (IVH), in-stent thrombosis, retroperitoneal hemorrhage, and femoral pseudoaneurysm have been rarely reported12–21 (table 1). To date, there have been no reports specifically focusing on the technical management of these complications.
Collection of studies reporting significant complications of dural venous sinus stenting in patients with IIH
While the literature suggests VSS to have high efficacy and low complication rates, there is potential for severe complications. There is essentially no guidance in the literature on stent construct sizes or lengths, location of stent placement based on anatomic variability, or technical aspects about avoiding complications while performing the procedure. The aim of this manuscript is to provide expert opinion on severe complications from the databases of several operators with robust stenting experience and provide management strategies for the early identification and treatment of these complications, in the absence of societal recommendations or guidance. The intent is to provide education on this important and emerging therapy for providers performing VSS to treat IIH.
Methods
Six cases of clinically-significant complications of VSS were identified through retrospective review of 811 VSS procedures performed by seven neurointerventional practitioners at six centers. Information collected, including patient age, sex, IIH diagnostic methodology and values, current and past symptoms, and past medical treatment of IIH, was gathered from the electronic medical records. Information regarding procedural technique, endovascular devices used, and any specific intraprocedural abnormalities encountered was gathered from the procedural notes and associated angiographic imaging/reports. All data were collected in a manner that allowed for complete patient de-identification. All data collection and analysis methods were approved by the Institutional Review Board at the institution where the data were collected.
Cases
Complication 1: acute SDH
A patient in their 30s presented with acute visual deterioration over 6 weeks with papilledema and intolerance to acetazolamide. Venography demonstrated severe transverse sinus (TS) stenosis with a gradient of 12 mmHg and concomitant superior sagittal sinus (SSS) stenosis with a gradient of 4 mmHg. The patient was placed on dual antiplatelet therapy of aspirin 325 mg and clopidogrel 75 mg daily for 7 days pre-procedure and underwent VSS under general anesthesia. Intravenous heparin (5000 units) was administered. Manometry was repeated pre-stenting using a Rebar-27 microcatheter (Medtronic, Dublin, Ireland) without complication. A Neuron 070 guide catheter (Penumbra, Alameda, CA) was navigated into the TS over a Berenstein 5F insert catheter (Merit Medical, Salt Lake City, UT) and 0.038 inch Glidewire (Terumo Medical, Shibuya City, Tokyo, Japan) without difficulty. One Precise stent (Cordis, Hialeah, FL) was implanted from the proximal SSS to the torcula over a microwire and then two from the torcula to the transverse sigmoid sinus junction without issue (figure 1). Manometry was repeated demonstrating reduction in venous pressures and resolution of the pressure gradients. Final internal carotid artery (ICA) injection was performed demonstrating no residual TS stenosis and no stent thrombosis. A tiny amount of venous extravasation emanating from the region of the anterior petrous apex and extending under the right temporal lobe was present in the venous phase of the post-stent angiogram, but was not immediately recognized during the procedure by the operator. Heparinization was therefore not reversed, and the patient emerged from anesthesia normally. The patient emerged with significant headache and nausea, which persisted. The patient was noted to be obtunded in the recovery room 1 hour later with a fixed and dilated right pupil and hemiparesis. Emergent CT demonstrated a holoconvexity right hyperacute SDH, protamine was given, and the patient was taken for emergent craniotomy and hematoma evacuation. No ongoing bleeding was encountered intraoperatively. The patient was restarted on aspirin and clopidogrel 2 days after the craniotomy. The patient has made a full recovery and is neurologically normal with excellent visual improvement.

Case 1: (A) Pre-stenting and (B) post-stenting venous phase angiogram demonstrating venous extravasation along the floor of the middle fossa (blue arrow). (C) Non-contrasted head CT obtained immediately after the patient decompensated in the PACU. (D) Non-contrasted head CT obtained postoperative day 1 after craniotomy for evacuation of the subdural hematoma. PACU, post-anesthesia care unit.
Learning points
In this case, venous extravasation occurred from a remote site that was not catheterized; the reason for this extravasation is not clear, but may have been from inadvertent wire puncture while obtaining sinus access. While not borne out in the literature, the authors recommend performing ipsilateral ICA angiography before and after VSS for visualizing the venous system in its entirety and ensuring no evidence of stent or adjacent venous thrombosis and for visualizing overall perfusion pre- and post-stenting. In this case, ICA injection was performed; however, greater attention to the venous phase structures may have allowed for early identification of venous extravasation. Early identification would have been beneficial as protamine could have been administered, better blood pressure control could have been utilized, and early CT with close monitoring to identify the SDH may have potentially allowed for surgical treatment to be initiated before a herniation event occurring. Many patients emerge from anesthesia with headache and nausea; however, in cases where a deficit is noted or the nausea or headache are out of proportion to the procedure after VSS, emergent CT should be ordered to rule out intracranial hemorrhage. In this case emergent craniotomy on aspirin and clopidogrel was necessary and was tolerated without bleeding sequelae.
Complication 2: Intra-procedural stent thrombosis
A recently post-partum patient in her 20s presented with worsening subacute visual acuity and papilledema refractory to medical therapy. Venography demonstrated significant right TS stenosis with a gradient of 16 mmHg. It is not the standard of any author to conduct preoperative clopidogrel response assays, and consistent with that none was conducted in this case. The patient was placed on dual antiplatelet therapy of aspirin 325 mg and clopidogrel 75 mg daily for 7 days pre-procedure and underwent VSS under general anesthesia. Intravenous heparin (5000 units) was given after placement of femoral arterial and venous sheaths. Two 8 mm × 40 mm Precise stents were deployed from the torcula to the transverse sigmoid sinus junction without issue (figure 2). Navigation of the microcatheter through the stents for post-stenting manometry was attempted, but the microwire could not navigate the stent construct. ICA angiography was then repeated, demonstrating acute stent thrombosis. An additional 4000 units of intravenous heparin was administered. Activated clotting time (ACT) was checked 5 min later and was only 189 s, and so another 5000 units of intravenous heparin (total of 14 000 units) was given with an increase in the ACT to 229 s. The Neuron 070 guide catheter was introduced into the non-dominant left TS and contralateral access was used to allow microcatheterization of the SSS for infusion of a weight-based loading dose of eptifibatide over 8 min. The right-sided TS stents were then accessed across the torcula with a wire and opened with sub-maximal angioplasty utilizing a 3 mm × 15 mm Gateway balloon (Stryker, Kalamazoo, MI), a Viatrac 5 mm × 30 mm balloon (Abbott Laboratories, Chicago, IL), and a Viatrac 7 mm × 30 mm balloon. Serial ICA injections were performed demonstrating persistent improvement in flow through the stented TS. The patient was continued on an intravenous heparin drip overnight and discharged on clopidogrel and apixaban, with no neurological sequelae and satisfactory post-procedural improvement in vision. No aspirin or clopidogrel response assays were conducted. The patient continued clopidogrel and apixaban for 3 months, and was then transitioned to aspirin and clopidogrel and has had no complications from this and no further signs of stent thrombosis.
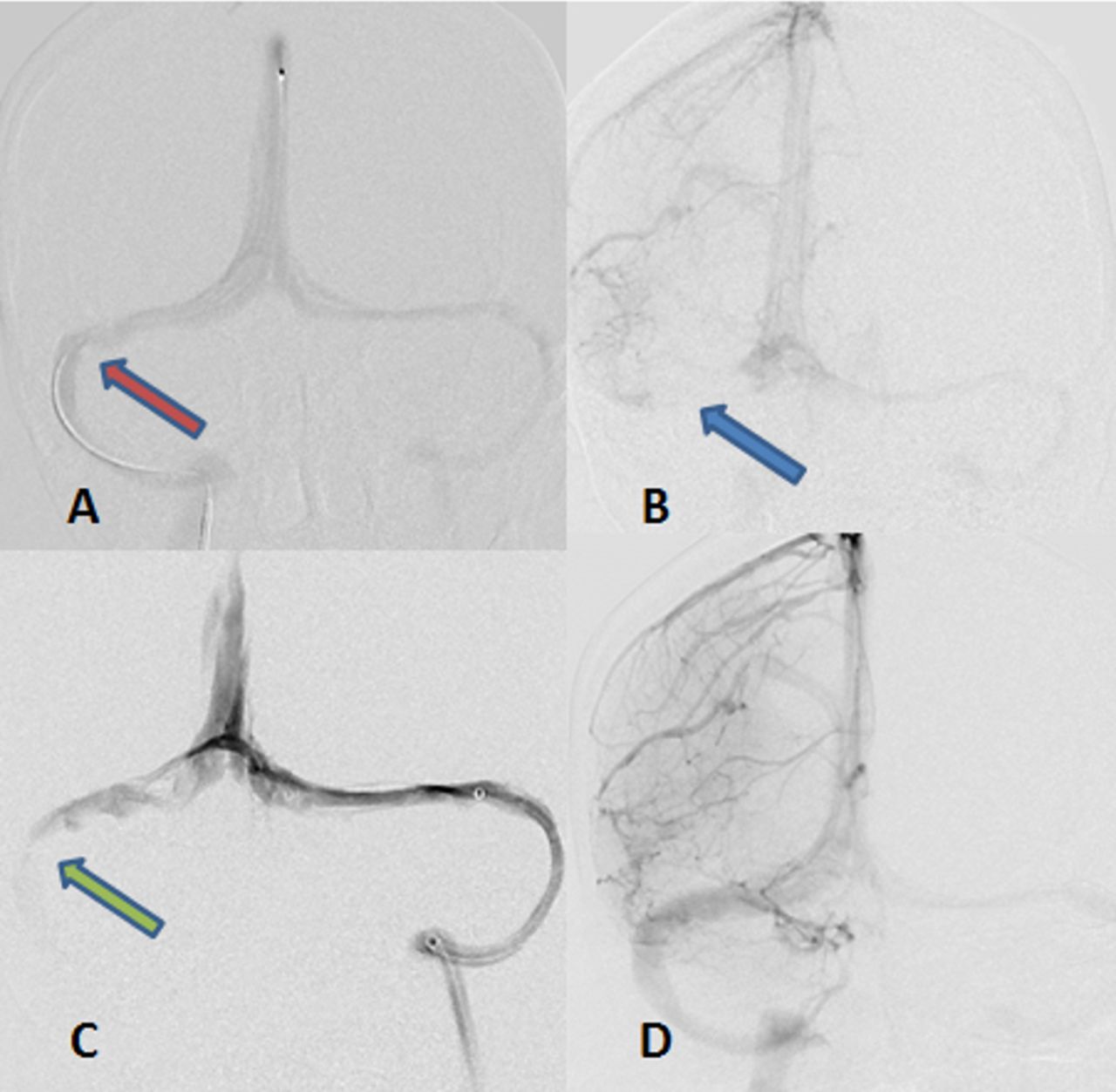
Case 2: AP venogram demonstrating (A) stenosis (red arrow) of the dominant right TS. (B) Thrombosis of the right TS stent (blue arrow). (C) AP venogram demonstrating thrombosis of the right TS stent (green arrow) and (D) following successful recanalization. AP, anteroposterior; TS, transverse sinus.
Learning Points
Acute venous sinus stent thrombosis poses unique considerations given the fact that venous flow is typically towards the heart, and thus contrast flows from the catheter tip down the catheter length. In this case, microcatheterization of the stents could not be performed to allow for adequate thrombolytic infusion, and guide catheter access through the occluded stents was not attempted due to concern for potential stent telescoping or migration. Contralateral venous sinus access, if the anatomy allows, represents a useful corridor for obtaining distal access to the thrombus to allow for thrombolytic infusion and other thrombectomy techniques, such as angioplasty. In this case, contralateral TS access allowed for recanalization of the occluded stents in a safe manner. The patient was a poor responder to heparin and, since this case, the authors now perform ACT during each procedure after heparinization to identify potential heparin non-responders before stent implantation. Strict compliance with ACT surveillance may have allowed for early recognition of poor heparin responsiveness and prevented this complication.
Complication 3: delayed in-stent thrombosis
A patient in their 30s presented with blurred vision and papilledema refractory to medical therapy. Venography demonstrated a 15 mmHg gradient across severe right-sided TS stenosis. The patient was placed on dual antiplatelet therapy of aspirin 325 mg and clopidogrel 75 mg daily for 7 days pre-procedure (clopidogrel response testing not performed) and underwent right VSS under general anesthesia with placement of a Zilver 6 mm × 40 mm stent (Cook Medical, Bloomington, IN) across the stenotic right TS in the standard fashion. There were no identified intraoperative complications and the patient was awoken from general anesthesia and discharged. Three weeks after the procedure the patient presented to the emergency department with 1 week of progressive headaches without neurologic deficit. CT venography demonstrated occlusion of the right TS stent (figure 3A–C). The patient was taken to the angiography suite where they underwent revascularization using a tri-axial system with an Ace 68 (Penumbra, Alameda, CA) for aspiration and then a UniFuse catheter (Angiodynamics, Latham, NY) to deliver tissue plasminogen activator (tPA) infusion. The thrombus was rigid, and the UniFuse catheter was maneuvered with significant difficulty into the clot and peri-torcular SSS. Weight-based tPA was then infused through this catheter over 3 days, in addition to systemic intravenous heparin infusion. The patient underwent catheter directed venography postoperative days 1 and 2 for monitoring of the stent, which remained patent. After the UniFuse catheter was removed on postoperative day 3, selective venous manometry demonstrated a persistent gradient of 6 mmHg. The patient was discharged on dual antiplatelet therapy of aspirin 325 mg and clopidogrel 75 mg daily. Clopidogrel response testing was not performed. Grade 4 papilledema did not resolve, so the patient underwent ventriculoperitoneal shunt (VPS) placement 1 month after revascularization after holding clopidogrel for 1 week. The papilledema improved after VPS placement and the patient was managed on the previous dual antiplatelet therapy, with eventual transition to aspirin monotherapy. The most recent CT venogram obtained on aspirin monotherapy demonstrated a patent stent. Hypercoagulability workup obtained during the thrombosis admission revealed a significant level of immunoglobulin G (IgG) antibodies to β-2 glycoprotein I receptor, signifying possible antiphospholipid syndrome.22
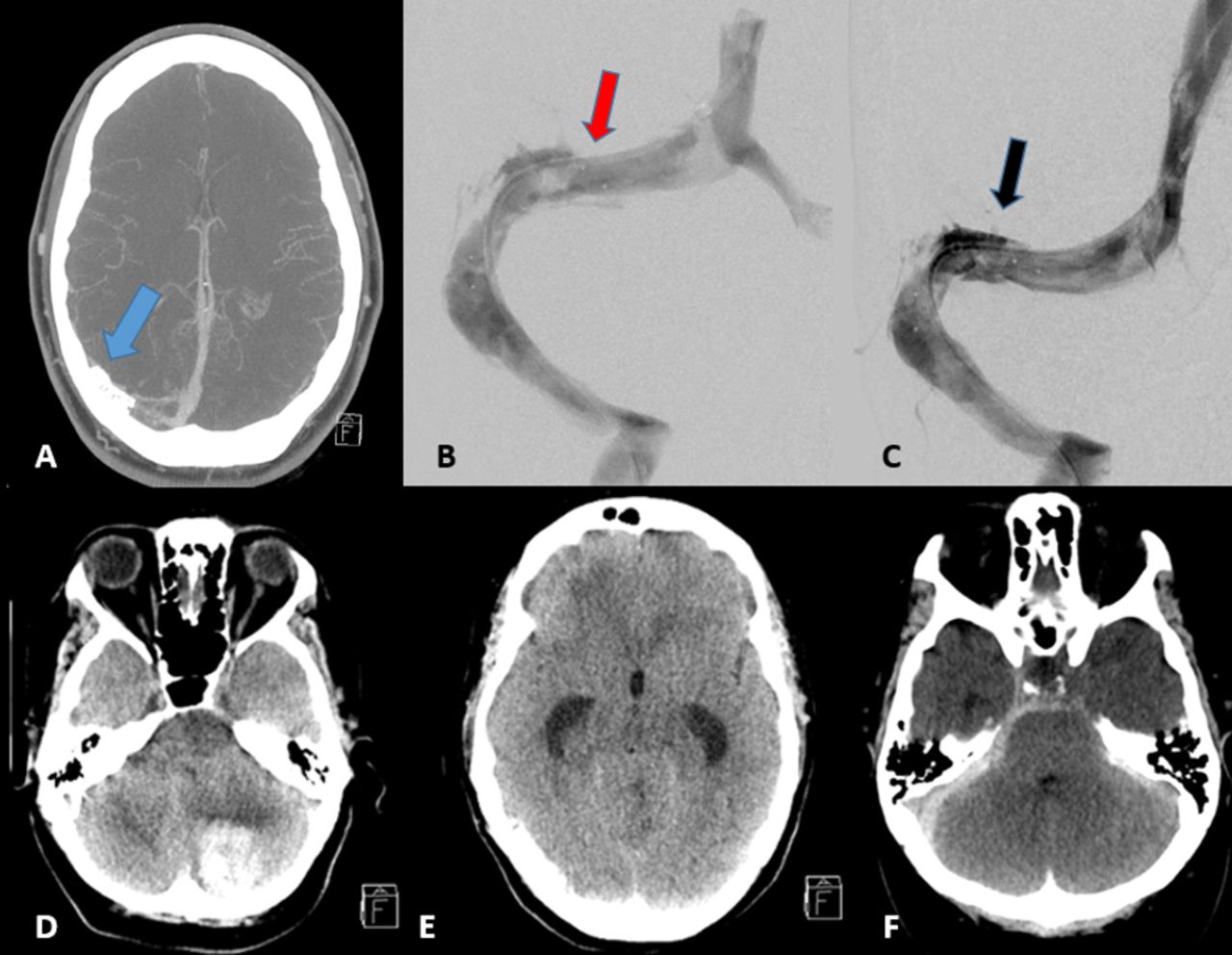
(A) Case 3: Axial CTA of the head demonstrating no enhancement or hemorrhage adjacent to the right TS stent (blue arrow). (B) Oblique catheter venogram on post-revascularization day 1 after 24 hours on tPA drip demonstrates some thrombus within the right TS stent (red arrow), with (C) resolution on post-revascularization day 2 (black arrow). (D) Case 4: Left sided cerebellar ICH with (E) obstructive hydrocephalus. (F) Case 6: Non-contrast axial head CT demonstrating SAH in the left choroidal fissure with IVH. CTA, CT angiography; ICH, intracerebral hemorrhage; IVH, intraventricular hemorrhage; SAH, subarachnoid hemorrhage; tPA, tissue plasminogen activator; TS, transverse sinus.
Learning points
Management of delayed stent thrombosis should focus on early revascularization to restore venous outflow and prevent cortical vein thrombosis or hemorrhagic complications from occlusion of the dominant TS and potentially prevent the need for cerebrospinal fluid (CSF) shunting. In this case, local tPA infusion was performed over a 3 day time period resulting in recanalization without complication. It is the opinion and experience of the authors that systemic anticoagulants are unlikely to lead to timely recanalization given the clot burden present within an occluded stent, and thus direct transvenous revascularization is recommended. While ultimately shunting was necessary for persistent papilledema, serious sequelae such as venous infarcts or intracranial hemorrhage were avoided by aggressive transvenous revascularization.
It is important to note that a subset of patients with IIH will have an underlying hypercoagulable state.23 There is little consensus on the role of preoperative hypercoagulability workup in patients with IIH who have never presented with clinical thrombosis, and likely workup in that scenario would not be beneficial. Patients who develop thrombus formation in an acute or delayed manner should undergo hypercoagulability evaluation.
Complication 4: contralateral cerebellar hemorrhage with IVH
A patient in their 50s presented with blurred vision, papilledema, and elevated opening pressure on lumbar puncture. Venography demonstrated severe stenosis of the right TS with significant pressure gradient. The patient was placed on dual antiplatelet therapy of aspirin 325 mg and clopidogrel 75 mg daily for 7 days pre-procedure and underwent VSS under general anesthesia. A Neuron 070 guide catheter was navigated over a Berenstein 5F insert into the right TS, where a Zilver stent was deployed across the stenosis without issue. Runs from the ICA were obtained demonstrating no complications, and the patient was awoken from anesthesia without incident. Ten hours after the procedure the patient developed headaches, nausea, emesis, and obtundation. CT of the head demonstrated left cerebellar hemorrhage with fourth ventricular compression and acute triventricular hydrocephalus (figure 3D,E). The antiplatelet agents were reversed and an external ventricular drain was placed emergently at the bedside. The patient’s neurological exam remained poor and the subject ultimately expired.
Learning points
In this case there were no intraprocedural abnormalities to explain or predict the development of the cerebellar ICH, which developed in a site remote from access with wires or catheters. No venous extravasation was appreciated on review of imaging, and the etiology of the hemorrhage is presumed to be venous congestion as a result of changes in venous flow patterns occult to intraprocedural venography. Alternatively poorly controlled hypertension, exacerbated by the normal post-procedural headache, while on antiplatelet agents could also have led to a hypertensive cerebellar hemorrhage. Finally, cerebellar hemorrhages have been reported following dramatic reductions in ICP, usually following aggressive CSF removal intraoperatively, which could also have contributed if ICP was abruptly and dramatically reduced.24 25
Adequate blood pressure control following VSS is highly recommended. To monitor for hemorrhagic complications, the physician now routinely obtains a non-contrast CT of the head 2 hours post-procedure. This practice is not uniform among all authors; however, all authors have a low threshold for CT imaging if there is concern for neurological deficit or unexplained severe symptoms after VSS.
Complication 5: subdural perforation with microcatheter during venography
An obese teenage patient presented with severe papilledema and elevation of opening pressure on lumbar puncture initially treated with VPS. Removal of the VPS after infection led to worsening papilledema, and the patient presented for venography, venous manometry, and cerebral angiography. The patient was placed on dual antiplatelet therapy of aspirin 325 mg and clopidogrel 75 mg daily for 7 days before the initial evaluation to facilitate possible stent placement. Venography and manometry were performed with minimal sedation and without initial systemic heparinization. A 5F Penumbra Select insert (Penumbra, Alameda, CA) was navigated through a 6F Benchmark guide catheter (Penumbra, Alameda, CA) into the internal jugular vein. A Headway 027 microcatheter (Microvention, Aliso Viejo, CA) was guided into the right sigmoid sinus over a Synchro 2 Standard 014 microwire (Stryker, Kalamazoo, MI) with J-curve on the wire. The microwire was then passed without difficulty across the torcula into what appeared to be the left sigmoid sinus. There was some resistance to passage of the microcatheter over the wire and so the wire was removed and contrast injected, demonstrating the catheter tip in the subdural space (figure 4). The patient was immediately assessed and found to have no headache or neurologic changes. Angiography did not demonstrate extravasation from a cortical vein or from the sinus itself. A flat-detector CT (DynaCT, Siemens, Munich, Germany) was then obtained on the table, demonstrating a small volume of contrast in the subdural space. The microcatheter was withdrawn back into the sinus under blank roadmap while puffing contrast. Repeat venography again did not demonstrate any extravasation. Manometry was performed, and no significant gradient was identified. CT of the head 5 hours post-procedure demonstrated resolution of the subdural collection, and the patient was discharged home 2 days post-procedure neurologically intact.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Case 5: (A) Lateral venogram demonstrating the tip of the microcatheter in the subdural space of the posterior fossa. (B) AP venous phase angiogram demonstrating no cortical venous extravasation. (C) DynaCT sagittal view demonstrating contrast in the posterior fossa subdural space (red arrows). (D) AP and (E) lateral venography after microcatheter withdrawal demonstrating no extravasation from the sinus. (F) Head CT 5 hours post-procedure demonstrating no subdural hematoma. AP, anteroposterior.
Learning points
In this case, the first sign alerting the physician to a potential complication was the resistance to advancing the microcatheter over the wire. Resistance to microcatheter access is frequently encountered during retrograde sinus access, likely secondary to anatomical variability such as cortical vein anastomoses, webs, dural leaflets, or other anatomical anomalies that have been documented in the venous sinuses.26 Often times using a microwire ‘J’ configuration assists with safe access through the transverse sinus. Undue resistance while manipulating the microwire and microcatheter in the sinuses should prompt withdrawing the microcatheter and wire and attempting access again. This is particularly important at the sigmoid sinus–jugular bulb interface where webs may exist.
If suspicion for venous perforation is high, investigation with gentle microcatheter venous injection to assess for sinus perforation is indicated. Before removing the catheter, which may be tamponading venous extravasation, protamine should be given (if heparinized) and ICA angiography should be performed to look for venous extravasation. There are a few techniques to consider in the event of microcatheter entry into the subdural space. The catheter can be withdrawn over the wire, leaving the wire through the rent in the wall of the sinus. This provides the neurointerventionalist with the means to again access the defect and potentially coil across the defect. Alternatively the microcatheter can be withdrawn, as in this case, under blank roadmap guidance while puffing low contrast volumes, allowing the operator to confirm when the microcatheter is back in the sinus. Balloon tamponade could also be performed. Coil sacrifice of the injured segment of the sinus would not be recommended except in the direst of circumstances. In this case, the patient was under conscious sedation allowing for intraprocedural neurologic examinations, which helped to reassure the operator. Finally, this case illustrates the utility of DynaCT in documenting the location of contrast and for ruling out intracranial hemorrhage, which could alert operators to a neurosurgical emergency or reassure the interventionalist that the procedure can potentially be continued safely.
Complication 6: SAH and SDH after cerebellar cortical venous perforation
A patient in their 50s presented with papilledema refractory to weight loss and acetazolamide. Venography demonstrated severe stenoses of the bilateral transverse sinuses with a gradient of 32 mmHg on the right and 14 mmHg on the left. The patient was placed on dual antiplatelet therapy of aspirin 325 mg and clopidogrel 75 mg daily for 5 days pre-procedure. Without heparinization, a Neuron Max (Penumbra, Alameda, CA) was placed in the right TS and attempts were made to advance a stent into the right TS but were unsuccessful due to challenging anatomy. So, we proceeded to stent the left side. Stenting of the left side was uneventful. Following the stenting, a Rebar 18 microcatheter was advanced through the stent and into the right TS to attempt to obtain bilateral venous manometry. There was difficulty crossing the right-sided stenosis, even in a retrograde fashion. A venogram was performed which showed extravasation of contrast (figure 3F), which was not immediately recognized. The patient complained of severe (8/10) headache and neck pain postoperatively but did not have any drowsiness or focal neurological deficit (ie, Glasgow Coma Scale 15). A CT was obtained which showed a mixed subdural and perimesencephalic SAH which was asymmetric to the right. Review of prior runs revealed perforation of a right-sided cerebellar bridging cortical vein. The patient was monitored for 2 days in the neuro-ICU with repeat CTs being performed at 1, 12 and 24 hours. During this time antiplatelet therapy was halted, but was resumed on discharge at postoperative day 2. No surgical intervention was performed and the patient has done well in follow-up.
Learning points
The acute SAH and SDH in this patient during the procedure was due to rupture of a cerebellar cortical vein at the junction between the subdural and subarachnoid space. The mechanism of hemorrhage here was either from a microcatheter or wire perforation. A less likely potential mechanism of cortical vessel rupture would be a forceful microcatheter injection. There were significant challenges in advancing catheters and wires across the right-sided stenosis. Practitioners should have a low threshold to abandon efforts to catheterize or stent a sinus if there is significant resistance to the advancement of catheters and wires. Gentle injections and ensuring that catheters are not wedged in either the wall of a sinus or in a tiny cortical vein should also be employed to avoid ruptures from catheter injections.
Discussion
This series of six selected cases was designed to highlight unique, potentially severe complications of VSS and present expert author opinion on management strategies and salvage techniques, in the absence of societal evidence-based recommendations. Acute SDH, acute stent thrombosis, delayed stent thrombosis, perioperative cerebellar hematoma, venous perforation, and cerebellar cortical vein perforation resulting in SDH and perimesencephalic SAH are all rarely reported and/or previously unreported complications that occurred following VSS by one of our authors. Among 811 VSS procedures and 1466 venograms for IIH performed across six institutions by seven practitioners, major complications occurred in 1.7% of VSS procedures and 0.14% of venograms. A neurointerventionalist performing these procedures should be aware of these potential complications and this article aims to serve as a resource for physicians who may rarely encounter similar clinical scenarios.
A number of series and meta-analyses have been published that report on major or minor complications after VSS. A meta-analysis by Starke et al 5 reported an overall major complication rate of 1.6% and overall minor complication rate of 3.8%, while Puffer et al 10 found an overall major complication rate of 2.1% and overall minor complication rate of 4.2% using similar review methodology. Definitions of major and minor complications were not consistent across publications. Ten series have reported on major complications such as SDH, SAH, ICH, retroperitoneal hematoma, femoral artery pseudoaneurysm, and stent thrombosis (table 1). SDH was reported by Ahmed et al 13 in one of 52 patients and by Kumpe et al 15 in one of 18 patients. In-stent thrombosis has been reported between 2.3% and 15.4% depending on the series,12 18 20 although most recent series have reported dramatically lower thrombosis rates. Boddu et al reported impaired drainage of the ipsilateral vein of Labbe after dural VSS in 13% of cases.27 There has been a single case reported in the literature of dural arteriovenous fistula formation after VSS.28 The overall incidence of serious complications based on the published literature varies from 1.9–6.7% (table 1). The senior authors calculate their incidence of serious complications to be close to 2%. To our knowledge, there have been no previously reported mortalities following VSS, making the case in this series the first reported fatality after VSS.
As the popularity of VSS increases and more neurointerventionalists add this treatment to their repertoire, the incidence of complications will likely increase, particularly by those inexperienced with intracranial venous catheterization. For novel procedures and procedures utilizing otherwise rare techniques, it is important to consider the learning curve phenomenon. Learning curve phenomena have been demonstrated in carotid artery stenting in particular, with a decrease in catheterization phase strokes as experience increases.29 We believe VSS is subject to a similar learning curve due to the relatively infrequent need for venous access and navigation, which is only necessary in venous thrombectomies, or even more rarely during arteriovenous malformation or fistula treatment. Maneuvering wires, catheters and stents across the jugular foramen into the venous sinuses requires substantially more force than is needed in the arterial system and may require rigid wires and robust guide constructs. The sinuses are enveloped by the dural leaflet which tolerates significant load and lessens the risk of perforation, but cortical veins entering the sinuses are not protected by this leaflet and are vulnerable to perforation with forceful manipulations as demonstrated in complication 3. This can be avoided by placing a J-curve on the microwire and/or keeping the wire pointed inferiorly away from the entrance of cortical veins such as Labbe when traversing the transverse sinus. These maneuvers are made easier with a strong triaxial support system, examples of which are highlighted in these cases.
In the operators’ experience, balloon angioplasty is uncommonly needed following stent placement. Furthermore, while the literature is silent on the matter, it is the authors’ opinion that pre-dilation of the venous stenosis is unnecessary and potentially harmful. In cases where the stenosis is a result of prior thrombosis or the sinus stenosis is rigid, post-dilatation may be necessary. These lesions are often evident by the irregular, intrinsic nature of a filling defect, and typically result in stent deformation and narrowing by the stenotic site. In our collective experiences there is almost never an indication for angioplasty before stenting as this poses potential risk of venous injury or rupture and is almost never required for distal guide catheter or stent navigation.
As the venous system is accessed in a retrograde manner, bleeding complications or thrombus formation are often occult to the operator if appropriate measures are not taken to assess for these complications. We recommend obtaining ipsilateral ICA arteriography through the venous phase before stenting as a baseline and then again following stenting to rule out venous extravasation, cortical vein obstruction or thrombus formation. This imaging is particularly useful for practitioners who are less experienced with VSS and may be less apt to recognize these complications during venography alone. Arteriography can also be repeated if there is an intraprocedural event that needs further evaluation. It is the opinion of the authors that re-accessing the ICA in these patients is relatively safe as the patients are generally young with favorable arch anatomy. Another tool available to assess for intraoperative complications is the flat detector CT. Recent studies have shown this modality to be reliable at detecting SAH, IVH and even loss of gray-white differentiation.30 In our presented sinus perforation case (complication 6), DynaCT revealed there was no SDH after perforation of the sinus with the microcatheter, which reassured the operator and the procedure was continued normally. Following uncomplicated VSS, most patients emerge from anesthesia with headache and nausea from stent radial force acting on the sinus wall. Assessing for hemorrhage in the immediate post-procedural stage can therefore be confounded by normal postoperative symptoms. As such, one of the senior authors has made it his practice to obtain a routine short-interval non-contrast CT to rule out ICH, although this is not practiced uniformly among the other authors. Certainly, imaging should be considered in any patient with worsening headache or with worsening neurologic deficit or level of consciousness in the postoperative time period.
The association between IIH and thrombophilia has been known for some years.23 In one retrospective series a decreased level of antithrombin 3 (AT3) and proteins C and S were noted in 4–5% of IIH patients, which is elevated compared with controls.31 The same study noted that 31% of their IIH patients demonstrated some variety of thrombophilia, and those patients had worse visual outcomes. Antiphospholipid antibody syndrome (APLA) is a specific thrombophilia known to be associated with up to 43% of patients with IIH.23 The study conducted by Pollak and colleagues found that 31% of their IIH patients also had APLA, but that it had no effect on the natural history.31 There is no current recommendation to evaluate for thrombophilia in IIH patients before stenting with no history of arterial or venous thrombosis, but special attention with thrombophilia work-up should probably be performed in patients with a relevant history before VSS. Finally, while thromboembolic events have been reported in patients being treated with aspirin only,32 there is only weak evidence supporting dual antiplatelet agent therapy in the setting of VSS.11 The most commonly reported antiplatelet regimen is aspirin 325 mg and clopidogrel 75 mg daily for 3–5 days pre-procedure, and for 3–6 months post-procedure.4 At the very least, the high association of IIH and hypercoagulable states should alert operators to the need for patients to rigorously follow their antiplatelet premedication regimens.
This case series has limitations. This is a series of unique complications as recollected by the senior authors and selected for relevance and teaching points. However, to the authors’ knowledge this is the first series to focus on the technical management of these low-incidence, high-impact complications, and thus provides a unique cache of knowledge for other neurointerventionalists performing VSS.
Conclusions
VSS is increasingly being utilized as a treatment for selected patients with IIH. Serious, life-threatening complications in patients undergoing VSS are rare but require urgent attention and action. We report strategies to prevent and mitigate complications during VSS and in the postoperative period.
Ethics statements
Patient consent for publication
Ethics approval
IRB # 00067648.
References
Footnotes
Contributors KMF and RKT designed the study. KMF, MRA, FH, MTB, SRS, RM, KL, and WB contributed clinical cases and/or critical revisions to the cases, learning points, and discussion. RKT, KMF, and AJ contributed to the acquisition, analysis, and interpretation of data as well as drafting, revision, and submission of the manuscript. KMF conceived of the work and provided critical revisions and final review before submission.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests KMF- Associate Editor, Journal of Neurointerventional Surgery.
Provenance and peer review Not commissioned; externally peer reviewed.