Article Text

Abstract
Background Intrasaccular flow disruption with WEB is a safe and efficacious technique that has significantly changed endovascular management of wide-neck bifurcation aneurysms (WNBAs). Use of stent in combination with WEB is occasionally required. We analyzed the frequency of use, indications, safety, and efficacy of the WEB–stent combination.
Methods All aneurysms treated with WEB and stent were extracted from a prospectively maintained database. Patient and aneurysm characteristics, complications, and anatomical results were independently analyzed by a physician independent of the procedures.
Results From June 2011 to January 2020, 152 patients with 157 aneurysms were treated with WEB. Of these, 17/152 patients (11.2%) with 19/157 aneurysms (12.1%) were treated with WEB device and stent. Indications were very wide neck with a branch emerging from the neck in 1/19 (5.2%) aneurysms and WEB protrusion in 18/19 (94.7%). At 1 month, no morbimortality was reported. At 6 months, anatomical results were complete aneurysm occlusion in 15/17 aneurysms (88.2%), neck remnant in 1/17 (5.9%), and aneurysm remnant in 1/17 (5.9%). At 12 months, there was complete aneurysm occlusion in 13/14 aneurysms (92.9%) and neck remnant in 1/14 (7.1%).
Conclusions Combining WEB and stent is a therapeutic strategy to manage WNBA. In our series, this combination was used in 11.2% of patients treated with WEB, resulting in no morbidity or mortality with a high efficacy at 6 and 12 months (complete aneurysm occlusion in 88.2% and 92.9%, respectively).
- aneurysm
- flow diverter
- stent
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Since publication of the ISAT (International Subarachnoid Aneurysm Trial) results, the endovascular approach has increasingly replaced surgery when managing intracranial aneurysms (IAs).1 In cases where treatment was initially based on coil use (with or without balloon-assistance), treatment complexity of some IAs led to the development of alternative techniques such as flow diversion and flow disruption.2–6 Flow disruption with WEB (MicroVention, Aliso Viejo, CA, USA) is an innovative treatment for wide-neck bifurcation aneurysms (WNBAs) that has been evaluated in several multicenter prospective studies, including two European trials (WEB Clinical Assessment of Intrasaccular Aneurysm Therapy (WEBCAST) and WEBCAST-2), one trial in the United States (WEB Intrasaccular Therapy (WEB-IT)), and one French trial (French Observatory), showing high safety and efficacy in the short and long term.7–14 Additional WEB trials are currently recruiting or under analysis: CLinical Assessment of WEB Device in Ruptured aneurYSms (CLARYS), CLinical EValuation of WEB 0.017 Device in Intracranial AneuRysms (CLEVER), and WEB-IT China (WEB-IT China).
The initial clinical experience with WEB showed that WEB sizing was critical to obtain a good apposition of the lateral surface of the WEB against the aneurysm wall and a complete sealing of the aneurysm neck. Recommendations regarding WEB sizing have evolved over time including proposing oversizing (approximately 1 mm) the device in transverse diameter.15 Although this approach is now routine practice, excessive oversizing may lead to WEB protrusion, which is potentially associated with thromboembolic events (TEs). To overcome the protrusion problem, three options have been considered: downsizing the WEB device, use of balloon assistance during or after WEB deployment, or placement of a stent in the parent artery in the event of protrusion with important reduction of parent artery lumen.16 However, downsizing the device may not be a viable option given its potential association with a higher risk of aneurysm recurrence. Given that balloon inflation during WEB deployment only very slightly changes the WEB position in the aneurysm sac, our limited experience with balloon assistance was inconclusive. Additionally, using balloon assistance after WEB placement led to poorer outcomes with no or very limited change in WEB position. After these relatively disappointing attempts with balloon assistance, our department devised a new strategy for WEB aneurysm treatment. The strategy involves oversizing the WEB device in transverse diameter and, in the event of WEB protrusion, placing a stent (adjunctive stenting) in the parent artery.
We report and retrospectively analyze our preliminary experience with this strategy in patients treated with WEB and stent in our prospective database of patients treated with WEB.
Materials and methods
According to the retrospective study design and the fact that WEB treatment and intracranial stenting were already part of current clinical practice, no institutional review board or ethics committee review was necessary; instead, patients were required to give oral consent for data use.
Patients
Since 2001, our department has maintained a prospective database of all patients with endovascularly treated aneurysms. We extracted data from all patients from the database who had aneurysms treated with WEB and stent between June 2011 (first WEB patient) and January 2020.
Web device
The WEB is a self-expanding, retrievable, electrothermally detachable, nitinol braided device, placed within the aneurysm sac. There have been several WEB device iterations over time. From November 2013, WEB DL (dual layer) was replaced by WEB with a single braid (WEB SL (single layer) and WEB SLS (single layer spherical), each possessing a barrel and a spherical shape, respectively).
Stents
The following stents were used: Low-Profile Visualized Intraluminal Support Junior (LVIS Jr) Stent (MicroVention, Aliso Viejo, CA, USA), Stent ACCLINO (Acandis, Pforzheim, Germany), and Stent Enterprise (Cerenovus, Miami, FL, USA).
Therapeutic strategy
In our center, treatment decisions for ruptured, unruptured, and recanalized aneurysms are made by a local multidisciplinary team that includes neurosurgeons and neuroradiologists. When endovascular treatment is selected as the primary treatment strategy, the Interventional Neuroradiology team selects the endovascular technique. WEB is usually used for treatment of WNBA, but the introduction of WEB 17 permits broader indications, such as pericallosal and sidewall wide neck aneurysms. Ruptured, unruptured, and recanalized aneurysms are treated with WEB if their anatomy is compatible with this treatment.
The decision to use stent in addition to WEB placement occurs in two circumstances:
Preoperative analysis shows that aneurysm anatomy, namely neck width, is not compatible with placement of the WEB device alone. This occurs when a branch emerges from the aneurysm neck, in which case a microcatheter is placed in the branch to be stented before WEB deployment; the stent is delivered after WEB deployment.
A WEB protrusion in the parent artery (or one branch of the bifurcation) is seen after several WEB deployments. In this case, the stenotic branch must be catheterized with a microcatheter and a stent placed in front of the neck and WEB. This strategy was developed after analyzing protrusion situations where WEB size reduction (or WEB undersizing) will inevitably conduct to mid-term or long-term aneurysm recanalization.
Embolization procedure
Procedures were performed under general anesthesia on a biplane angiographic system (Axiom Artis, Siemens Biplane and Allura Clarity, Philips Healthcare). Since 2013, all patients treated with WEB (with or without stent) received premedication with double antiplatelet treatment (DAPT). Two protocols were used successively: aspirin and clopidogrel (Sanofi-Aventis, Gentilly, France) for 5 days until April 2015, followed by aspirin and ticagrelor (AstraZeneca, Courbevoie, France) for 2 days. The change of DAPT protocol was prompted by the high rate of clopidogrel resistance. In the event of stent placement, this treatment continued for 3 months; thereafter, clopidogrel or ticagrelor were stopped and aspirin continued for at least 12 months post-procedure date. Antiplatelet activity testing was not performed.
Post-procedure MRI including diffusion-weighted imaging (DWI) was performed 24 hours post-procedure. Digital subtraction angiography (DSA) was performed at 6 and 12 months.
Follow-up imaging protocol
Anatomical follow-up of aneurysms treated by EVT is usually conducted on a lifetime basis.
Immediate postoperative aneurysm occlusion was evaluated on DSA performed at the end of the procedure. At 6 and 12 month follow-ups, both DSA and MRA were performed. Yearly or less frequent (depending on the initial anatomical occlusion and its evolution along the time) follow-up was performed using MRI/MRA. Ten years post-procedure, follow-up imaging was always performed using MRI/MRA every 5 years.
Data collection
The following data were collected:
Patient: age, gender;
Aneurysm: location, size (pretreatment);
WEB procedure: date, type and size of device used, any complications;
Stent type;
Procedure images, 24-hour MRI and DSA at 6 and 12 months.
Data analysis
All clinical data and collected images were independently evaluated by an interventional neuroradiologist with 5 years’ experience who was not involved in any procedure.
Aneurysm occlusion was evaluated at 6 and 12 months on a three-grade scale: complete occlusion, neck remnant, and aneurysm remnant. WEB shape was also evaluated at 6 and 12 months using a three-grade scale: no WEB shape modification, mild WEB shape modification (<50% of decrease in height), or strong WEB shape modification (≥50% in height). Artery status in which the stent was placed was evaluated using a four-grade scale: no stenosis, stenosis 50% or less, stenosis greater than 50%, and occlusion.
Statistical analysis
Continuous variables were described as mean±SD and range. Categorical variables were described as counts and percentage. Analyses were performed using Microsoft Office Excel 2010 (Redmond, WA, USA).
Results
Patients
From June 2011 to January 2020, 152 patients with 157 aneurysms were treated with WEB. Among them, 17/152 (11.2%) patients with 19/157 (12.1%) aneurysms were treated with WEB device and stent (table 1). Thirteen of 17 patients (76.5%) were female and mean age was 53±8 years (range 40–63 years). Sixteen patients were treated with WEB and stent for one aneurysm, while one patient (17) was treated for three aneurysms during three procedures.
Characteristics of patients and aneurysms
Aneurysms
Of 19 aneurysms (table 1), 15 (78.9%) were unruptured while four (21.0%) were recanalized aneurysms (N0 1, 3, 5, and 10). The four recanalized aneurysms were previously ruptured, treated at the acute phase of bleeding by coils in three patients (No 1, 3, and 10) and WEB in one patient (No 5). Patients were retreated with WEB and stent for aneurysm recanalization 4, 20, 22, and 3 years after initial treatment, respectively.
Aneurysm location was middle cerebral artery (MCA) in 11/19 (57.9%), basilar artery (BA) in 5/19 (26.3%), internal artery carotid terminus (ICAt) in 1/19 (5.2%), and anterior communicating artery (Acom) in 2/19 (10.5%). Aneurysms had a maximum width between 3.0 and 9.6 mm (mean 6.1±1.9 mm) and a height between 2.6 and 12.1 mm (mean 5.2±2.7 mm). The neck was narrow (<4 mm) in 9/19 (47.4%) and wide in 10/19 aneurysms (52.6%).
Procedures
Pretreatment DAPT was aspirin and clopidogrel in 5/17 (29.4%) patients and aspirin and ticagrelor in 12/17 (70.6%) patients (table 2). All aneurysms were successfully treated with WEB and stent (100%). WEB SL was used in 18/19 aneurysms and WEB DL (deployed through a Via 27) in 1/19 (No 1). Among aneurysms treated with WEB SL, 7 aneurysms were treated with WEB 17 system (No 11, 12, 13, 14, 15, 16, and 17 (third aneurysm)), 3 with WEB 21 system (No 3, 4 and 6), 7 with WEB 27 system (No 2, 5, 7, 8, 9, and 17 (first and second aneurysms)), and 1 (5.9 %) with WEB 33 system (No 10).
Dual antiplatelet therapy, devices, complications, and anatomical results
LVIS JR was used in 16/19 (84.2%), Enterprise in 2/19 (10.5%), and Acclino in 1/19 (5.2%) (figure 1).

{kind=link}
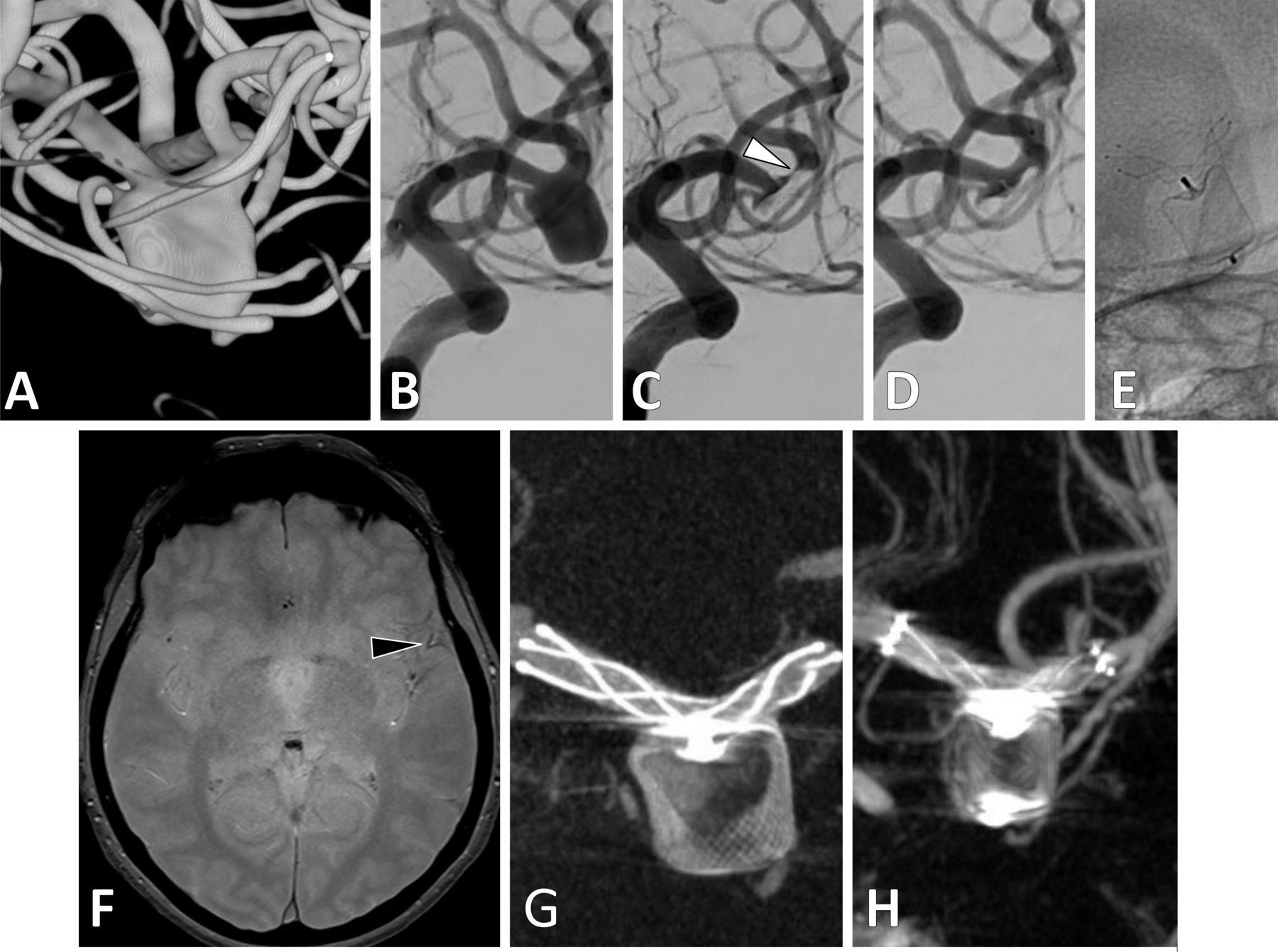
Patient17: unruptured left middle cerebral artery (MCA) aneurysm. (A) Three-dimensional digital subtraction angiography (3D-DSA) shows the aneurysm. (B) and (C) DSA, working view, before and after web device deployment. After web deployment web protrusion is visible (white arrowhead). (D) and (E) subtracted and unsubtracted working view. DSA subtracted and unsubtracted working view at the end of procedure show the web and the stent deployed. (F) Subarachnoid hemorrhage depicted by 24-hour MRI (T2*) (black arrowhead). (G) and (H) MIP 3D-DSA at the end of procedure and at 6 months, respectively, show the web and stent with complete aneurysm occlusion.
Stent placement was planned pre-procedure in 1/19 (5.2%) aneurysms due to a very wide neck with a branch emerging from it. In 18/19 (94.7%) aneurysms, stent placement was determined during procedure due to WEB protrusion.
Complications
There were seven minor complications in 5/17 patients (29.4%) and 7/19 aneurysms/procedures (36.8%). Three patients (No 5, 7, and 16) had transient ischemic attack (TIA) that occurred on day 1, 10, and 2 post-procedure, respectively. In all cases, control MRI performed after TIA showed multiple spots on DWI images without territorial infarct. Two patients (No 8 and 17) had four hemorrhagic complications including one (No 17) who had three procedures for three different aneurysms with one hemorrhagic complication at each of them. Among them, two were subarachnoid hemorrhage (SAH) depicted on 24-hour MRI occurring after MCA aneurysm treatment. The patient also had a cerebellar hematoma depicted on 24-hour MRI post-BA aneurysm treatment. These three events were not associated with any clinical deterioration. Finally, patient No 8 (treated for MCA aneurysm) had two hematomas in the Sylvian fissure, distal to the aneurysm, likely due to distal artery perforation during stent placement, indicated by postoperative headache and confirmed by 24-hour MRI.
Finally, all patients were mRS 0 1 month post-complication, resulting in a morbimortality rate of 0.0%.
Anatomical results at 6 months
DSA at 6 months was obtained in 15/17 (88.2%) patients and 17/19 (89.5%) aneurysms. Patient No 7 was evaluated only with MRI due to a vascular access problem. Patient No 12 did not attend his appointment at 6 months due to concurrent unrelated disease. Complete aneurysm occlusion was achieved in 15/17 aneurysms (88.2%), neck remnant in 1/17 (5.9%), and aneurysm remnant in 1/17 (5.9%). Patient No 3 with aneurysm remnant was retreated immediately after the 6-month control DSA (see below). No intra-stent stenosis or occlusion was shown.
WEB shape was unchanged in 13/17 (76.5%) aneurysms. There was mild modification in 2/17 (11.8%) aneurysms and strong modification in 2/17 (11.8%).
Anatomical results at 12 months
DSA at 12 months was obtained in 14/17 (82.3%) patients and 14/19 aneurysms (73.7%). Patient No 7 did not have a DSA control at 12 months (see above). Patient No 3, who was retreated 6 months post-WEB and stent procedure, was not included in this analysis. Patient No 17 (three aneurysms) refused follow-up DSA at 12 months. Complete aneurysm occlusion was achieved in 13/14 aneurysms (92.9%) and neck remnant in 1/14 aneurysms (7.1%).
No intra-stent stenosis or occlusion was depicted at 12 months.
WEB shape was unchanged in 10/14 (71.4%) aneurysms. There was mild modification in 3/14 (21.4%) aneurysms and strong modification in 1/14 (7.1%).
Retreatment
One patient (No 3) of 17 (5.9%) was retreated the year following the initial WEB and stent procedure. Additional coils were placed through the stent.
Discussion
This single-center retrospective study shows that additional stenting was used in a relatively low percentage of cases (11.2%). Stent placement was always performed after WEB deployment and was successful in all cases (100.0%). Complications (most asymptomatic) were observed in 29.4% of cases, but morbimortality at 1 month was 0.0%. Aneurysm treatment with WEB and stent was associated with excellent anatomical results: complete aneurysm occlusion in 92.9% and neck remnant in 7.1% at 12 months. Retreatment rate at 12 months was limited to 5.9%.
Since 2010, WEB treatment has primarily been used in Europe for WNBA management.17 Prospective, multicenter studies conducted in Europe and the USA have shown high safety and great efficacy at 12 months, 2 years, and 3 years.6 8 18 During the learning curve with this innovative device, it became apparent that appropriate WEB sizing is critical to obtain a stable and complete aneurysm occlusion. Achieving good apposition of the device against the aneurysm wall to properly block the neck required oversizing the WEB device relative to aneurysm mean transverse diameter of approximately 1 mm.15 However, oversizing may lead to WEB protrusion and potential stenosis of one branch of the bifurcation. This is particularly true for complex WNBA: aneurysms not centered on the bifurcation, irregular shape aneurysm, and aneurysms with a strong angulation with the parent artery. In these situations, proper deployment of the WEB in the aneurysm is sometimes challenging. To overcome this problem, Mihalea and colleagues have proposed combining WEB and remodeling techniques.16 The balloon is inflated before WEB deployment in order to slightly change WEB position in the aneurysm sac to avoid or reduce WEB protrusion.
As our experience with this technique was not very effective, we decided to evaluate another treatment strategy. This strategy, which we used in 18/19 aneurysms (94.7%), consisted of routinely oversizing the WEB and, if there was a WEB protrusion in one branch, placing a stent. In a limited number of aneurysms (1/19, 5.2%), placement was deemed mandatory at the beginning of the procedure. In this case, the microcatheter for stent deployment was placed before WEB placement, followed by WEB deployment and finally, stent deployment.
Adjunctive stenting was used with all WEB systems (17, 21, 27, and 33) and no specific problems were encountered with any system. Given the number of patients/aneurysms, it is unfeasible to analyze whether the progressive evolution of the WEB system (including evolution of delivering microcatheter size) has significantly influenced the need for adjunctive stenting. Both braided and laser-cut stents were used in combination with WEB, and no specific technical difficulty was encountered with any type.
In this series, we reported detailed data on complications, including those not associated with clinical deterioration and depicted only on postoperative MRI, an imaging protocol that has yet to be fully integrated into routine clinical practice. The detailed reporting of complications may partially explain why the reported rate of complications is relatively high (29.4%) and slightly higher than that reported with stent-assisted coiling (21.2%).19 Even if the complication rate was relatively high, most complications were asymptomatic and no morbidity or mortality was observed at 1 month. Compared with what was reported in European and US WEB studies (no mortality, morbidity 3.0% and 0.7%, respectively), the safety of the WEB and stent treatment is unlikely to be significantly different from WEB alone. Knowing that stent-assisted coiling is associated with a higher rate of morbimortality compared with coiling alone, this result is important.20
Very good efficacy results were observed in the present study with complete occlusion in 88.2% at 6 months and 92.9% at 12 months, and adequate occlusion in 94.1% at 6 months and 100.0% at 12 months. Furthermore, these efficacy results are superior to those reported in prospective, multicenter studies conducted in Europe and the USA. In the entire population of three European studies (WEBCAST, WEBCAST 2, and French Observatory), aneurysm occlusion at 12 months was complete occlusion in 52.9%, neck remnant in 26.1%, and aneurysm remnant in 20.9%.7–9 Similar results were reported in the US study: complete occlusion in 53.8%, neck remnant in 30.8%, and aneurysm remnant in 15.4%.11 However, a recent study analyzing factors affecting aneurysm occlusion after WEB treatment did not show a positive association between stenting and the rate of adequate occlusion.21
In contrast to what has been observed for anatomical results, rate of retreatment at 12 months is relatively similar across the European series (6.9%), US series (5.6%), and the current series (5.9%).
One previous series of 17 patients reported what the authors termed ‘Stent-assisted WEB’, and mentioned two circumstances in which stent placement was performed in addition to WEB treatment: (1) WNBA with a branch emerging from the neck, and (2) narrowing of a bifurcation branch.22 This is similar to what was observed in our series, in which the second indication for stent was by far the most frequent (94.7%). This series reported similar safety (no morbimortality), but slightly poorer efficacy at 12 months, with complete aneurysm occlusion in 69.0%, neck remnant in 12.5%, and aneurysm remnant in 18.5%.
Limitations
This study has some limitations. First this analysis was retrospectively conducted in a prospectively maintained database. At the beginning of our experience of combining WEB and stent, the impression was that it would be used in a very limited number of cases and that no prospective study was required to evaluate this treatment. Second, the patient cohort is relatively small because indications for combining WEB and stent are relatively limited. Nonetheless, it is important to report the usefulness, safety, and efficacy of this combination.
Conclusion
Combining WEB with stent is part of the treatment strategy to manage WNBA. In our series, this combination was used in 11.2% of patients treated with WEB, resulting in no morbidity or mortality and high efficacy at 6 and 12 months (complete aneurysm occlusion in 88.2% and 92.9%, respectively). This combination should be considered as a safe and effective option in the treatment of complex WNBA. Further studies (including comparative ones) are needed to further analyze the place of this EVT when managing intracranial aneurysms.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
References
Footnotes
Contributors All authors have: provided a substantial contribution to the conception and design of the studies and/or the acquisition and/or the analysis of the data and/or the interpretation of the data; drafted the work or revised it for significant intellectual content; approved the final version of the manuscript; and agreed to be accountable for all aspects of the work, including its accuracy and integrity.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests LP consults for Balt, MicroVention, Perflow, Phenox, and Vesalio.
Provenance and peer review Not commissioned; externally peer reviewed.