Article Text

Abstract
Background Poor patient outcomes after aneurysmal subarachnoid hemorrhage (SAH) occur due to a multifactorial process, mainly involving cerebral inflammation (CI), delayed cerebral vasospasm (DCVS), and delayed cerebral ischemia, followed by neurodegeneration. CI is mainly triggered by enhanced synthesis of serotonin (5-HT), prostaglandin F2alpha (PGF2a), and cytokines such as interleukins. Levosimendan (LV), a calcium-channel sensitizer, has already displayed anti-inflammatory effects in patients with severe heart failure. Therefore, we wanted to elucidate its potential anti-inflammatory role on the cerebral vasculature after SAH.
Methods Experimental SAH was induced by using an experimental double-hemorrhage model. Sprague Dawley rats were harvested on day 3 and day 5 after the ictus. The basilar artery was used for isometric investigations of the muscular media tone. Vessel segments were either preincubated with LV or without, with precontraction performed with 5-HT or PGF2a followed by application of acetylcholine (ACh) or LV.
Results After preincubation with LV 10−4 M and 5-HT precontraction, ACh triggered a strong vasorelaxation in sham segments (LV 10−4 M, Emax 65%; LV 10−5 M, Emax 48%; no LV, Emax 53%). Interestingly, SAH D3 (LV 10−4, Emax 76%) and D5 (LV 10−4, Emax 79%) segments showed greater vasorelaxation compared with sham. An LV series after PGF2a precontraction showed significantly enhanced relaxation in the sham (P=0.004) and SAH groups (P=0.0008) compared with solvent control vessels.
Conclusions LV application after SAH seems to beneficially influence DCVS by antagonizing 5-HT- and PGF2a-triggered vasoconstriction. Considering this spasmolytic effect, LV might have a role in the treatment of SAH, additionally in selected patients suffering takotsubo cardiomyopathy.
- inflammation
- pharmacology
- stroke
- aneurysm
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Aneurysmal subarachnoid hemorrhage (SAH) is a devastating hemorrhagic type of stroke, possibly leading to severe disability, functional dependency, or death in the affected patient group.1 2 Despite recent advances in tailored pharmacological approaches to address SAH-associated complications, patient outcomes still remain poor.3 Vasoconstrictive as well as proinflammatory cytokines are known to play an essential role in mediating and maintaining delayed cerebral vasospasm (DCVS).4 Endothelin-1 (ET-1) triggers DCVS by targeting the ET-A receptor (ETA-R), considering the established inactivation of the vasorelaxant ET-B1 receptors (ETB1-R) post-SAH.1 Driving factors for cerebral inflammation (CI), contributing to DCVS and neurodegeneration as well, include peripheral immune cells,5 inflammatory cytokines,6 serotonin (5-HT), and prostaglandin F2alpha (PGF2a).7
Levosimendan (LV), a calcium channel sensitizer, is already a mainstay in the treatment of congestive heart failure, as well as after SAH in patients suffering from DCVS and/or stress cardiomyopathy.8 It is known to significantly enhance maximal cerebral vasorelaxation after SAH, addressing mostly all subparts of the ETB1-R pathway (sarafotoxin S6c (S6c), sodium nitroprusside (SNP), bromo-cGMP (cGMP)).9 Cerebral vasocontractility under LV on PGF2a was also significantly reduced.10
Therefore, the aim of our study was to examine a potential vasorelaxant effect of LV by prior vasoconstriction with the proinflammatory mediators 5-HT and PGF2a under physiological as well as pathophysiological conditions mimicking SAH.
Methods
Animals and anesthesia protocol
The local ethics committee (Gen. Nr. F 138/12, 28 December 2009, Darmstadt, Germany) approved the experimental study which is in consensus with the German Federal Guidelines for animal experiments. Male rats, each 328–416 g in body weight (mean 346.32 ± 14.19 g), were included after fulfilling the legally needed acclimatization period. For all study issues, the ARRIVE guidelines were rigorously followed.11 Prior to each operation, maximal five rats were kept in a cage, combined with a 12-hour dark–light cycle. Food and water were available ad libitum.
Rats were randomized to either a sham or bleeding group; blinding was not feasible due to the neurological deficits in the SAH group objectified by the Bederson scale postoperatively.
Anesthesia was inducted with midazolam and ketamine (1 mg/kg body weight, intraperitoneal; 100 mg/kg body weight, intraperitoneal). Animals breathed spontaneously during the entire procedure without supplementary oxygen. For postoperative rescue analgesia animals received 5 mL crystalloid solution with 0.0125 mg fentanyl (Janssen-Cilag Pharma GmbH, Germany) intraperitoneally at least twice per day.
Surgical procedure and brain vessel dissection
For the detailed surgical protocol, we refer to previously published works.1 Briefly, SAH with autologous blood was induced after meticulously opening up the atlantooccipital membrane of each rat. After bleeding induction, the same surgical procedure was performed after 24 hours. Isotonic sodium chloride solution (0.9%) was injected twice in the sham group. The severity of bleeding induction, neurological deterioration, angiographic vasospasm, and magnetic resonance imaging perfusion deficits have already been published.12
On day 3 and day 5 postoperatively, rats were deeply anesthetized via CO2 narcosis. Subsequently, each rat was culled by exsanguination after cutting the carotid arteries. The brain was meticulously excised and immediately immersed in cold modified Krebs-Högestätt solution which was prepared on the day of the operation. Before euthanasia, a neurological evaluation was performed with the use of a grading system.1 SAH on the basal surface of the brain was macroscopically verified.
The basilar artery along with a subarachnoid plane were dissected from the brainstem under a binocular microscope (Carl Zeiss, Germany). Each artery was cut into four parts, measuring 2 mm in length. Rats and basilar artery segments were randomly assigned to different experimental groups. This enabled the use of segments from different animals in the final analysis of each group. Therefore, multiple vessels from each rat were taken.
Experimental workflow
All ring segments were mounted on stainless steel rods and introduced in an organ bath (IOA-5301; FMI GmbH, Germany). Isometric force changes were quantified in millinewtons (mN) and registered by using a transducer (GM Scaime, Annemasse Cedex, France).
Organ baths were filled with a modified Krebs-Högestätt solution and continuously carbonated with a humidified gas mixture (95% O2, 5% CO2). This resulted in a pH of approximately 7.35. For the analyses, 54 sham and 26 SAH vessel segments were included.
Segments without LV were defined as the control group. A reference contraction was induced by 124 mM potassium + Krebs solution (124 mM KCl) (Krebs-Högestätt solution with equimolar exchange of sodium chloride (NaCl) by KCl) and repeated at the end of each experiment. Segments reaching less than 2 mN of contraction were excluded before the experimental onset; likewise, segments developing less than 75% of the initial reference contraction at the end of the experiment were excluded as well. The functional integrity of the endothelium was tested by acetylcholine (ACh) (10−4 M) after precontraction with 5-HT (10−5 M). A vasorelaxation of more than 30% indicated a functionally intact endothelium. Segments not reaching this percentage were excluded from further analysis.
Muscular media tone was analyzed by the application of 124 mM KCl and prior preincubation with LV 10−4 M, 10−5 M, and 10−6 M in sham and SAH segments, and compared with a solvent control group. Vessel relaxation by ACh was analyzed after application of LV 10−4 M and LV 10−5 M in sham segments, as well as in day 3 and day 5 SAH segments with 10−4 M and compared with a solvent control group. Vessel relaxation was analyzed by the cumulative application of an LV series (10−8 M, 10−7 M, 10−6 M, 10−5 M, 10−4 M, 3×10−4 M) in sham and SAH segments as well, and compared with a corresponding solvent control group.
After a waiting period of 60 min, LV was added to the organ bath and vessels were preincubated for 20 min before testing vasocontractility using 124 mM KCl.
Also, LV was added to the organ bath for all sham segments at 10−4 M and 10−5 M, and to the SAH segments only in the LV 10−4 M group for day 3 and day 5 followed by incubation of 45 min. In each case, only one LV concentration-effect curve (CEC) was conducted by cumulative application to avoid tachyphylaxis. Post precontraction with 5-HT (10−9 M to 10−5 M), CECs for ACh (10−8 M to 10−4 M) were performed by cumulative application.
Likewise, vessel segments were precontracted by PGF2a 3×10−5 M in sham and SAH segments. An LV series (10−8 M, 10−7 M, 10−6 M, 10−5 M, 10−4 M, 3×10−4 M) was added to the organ bath for the sham and SAH group and compared with a solvent control sham group, as reported previously.13 The LV concentration range was determined according to current data in the literature, including our own experience.9 10
Compounds and solvents
Krebs-Högestätt solution was composed of the following components: NaCl (Sigma Aldrich, Germany), 119 mM; KCl (Sigma Aldrich, Germany), 3.0 mM; sodium dihydrogen phosphate, 1.2 mM (AppliChem, Germany); calcium chloride, 1.5 mM (AppliChem, Germany); magnesium chloride (Merck, Germany), 1.2 mM; sodium hydrogen phosphate (VWR International BVBA, Belgium), 15 mM; and glucose (Sigma Aldrich, Germany), 10 mM.
5-HT, PGF2a, and ACh were acquired from Sigma-Aldrich (Schnelldorf, Germany). LV was kindly provided by Jouko Levijoki, MSc (Pharm) of Orion Corporation, Orion Pharma (Espoo, Finland). All compounds were directly dissolved in distilled water or dimethyl sulfoxide (DMSO) on the day of each experiment. The selectivity of these compounds was described earlier.
Analysis of results and statistics
Vasocontraction was measured in millinewtons and given as percentage of the reference contraction. All values in the text and figures are given as mean±SD For each completed CEC, the Emax and pD2 or EC50 (ie, the concentration at which half of the maximal effect occurs) were calculated.
All statistical analyses, except for the 124 mM KCl, ACh, and PGF2a investigations, were performed using the non-parametric Wilcoxon–Mann–Whitney test. One-way analysis of variance followed by Scheffe’s test for post hoc comparisons of mean values was used for 124 mM KCl, ACh, and PGF2a investigations. A probability value (P) less than 0.05 was considered significant. Data were analyzed using IBM SPPS (Version 22; IBM Corp., Armonk, NY, USA). The sample size per group was determined using an a priori sample size calculation (BiAS.for.Windows Version 11; epsilon Verlag, Germany). To achieve α = 0.05 at β = 0.2 with a sigma of 0.2, the sample size calculation showed that n = 4–8 segments per group was appropriate to have a delta between 0.3 to 0.5. Figures were prepared using Microcal Origin 7.0 (OriginLab, Northampton, MA, USA).
Results
In total, 95 basilar artery ring segments were included (67 sham segments, 28 SAH segments), corresponding to 24 rats. Finally, 54 sham and 26 SAH segments were analyzed (sample size of at least five vessel segments per subgroup).
Effect of LV 10−4 M, 10−5 M, 10−6 M, or without on 124 mM potassium + Krebs solution-induced vasocontraction in sham and SAH segments
In sham segments, the maximal vasocontraction (Emax) elicited by 124 mM potassium + Krebs solution (124 mM KCl) was not altered in the LV 10−4 M (Emax 103%), LV 10−5 M (Emax 100%), LV 10−6 M (Emax 101%), or solvent control group (Emax 102%).
On day 3 after bleeding induction, prior preincubation with LV 10−4 M did not significantly (P=0.9) change the maximal contraction induced by 124 mM KCl (Emax 111%) (table 1).
Contractile assessment (124 mM KCl) after incubation with levosimendan under physiological and pathophysiological conditions
Effect of LV 10−4 M and 10−5 M after 5-HT-triggered vasoconstriction followed by ACh-mediated vasorelaxation in sham and SAH segments
All vessel segments were precontracted by cumulative application of 5-HT 10–5 M. In sham- and SAH segments, an ACh series (10−8 M to 10−4 M) followed, which was compared with a solvent control group in sham segments. The solvent control group showed a spontaneous diminution in muscular media tone over time.
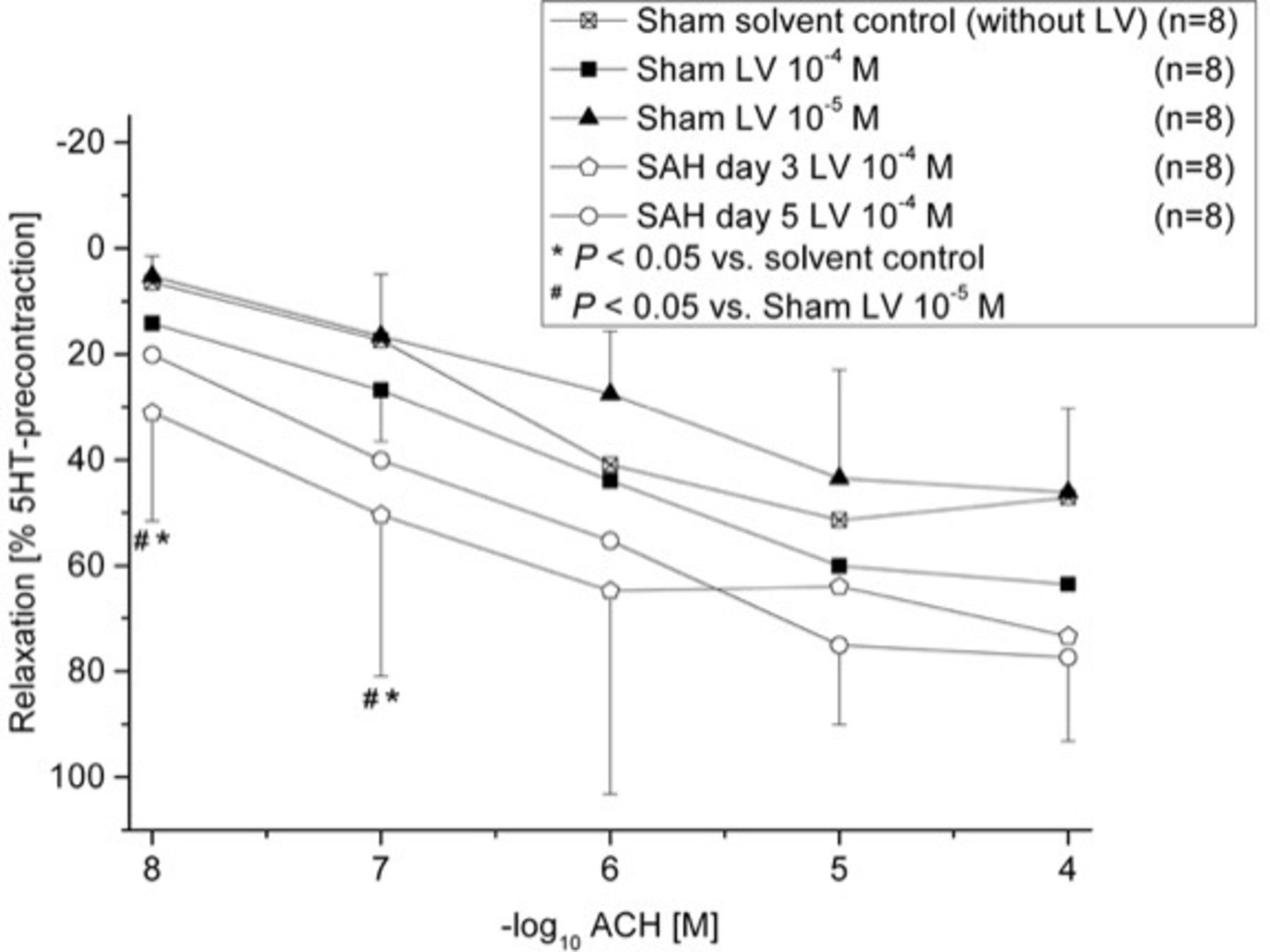
In all sham segments, ACh induced a strong vasorelaxation. For the LV 10–4 M group, vasorelaxation was stronger (Emax 65%) than in the LV 10−5 M group (Emax 48%) (figure 1).

Effect of acetylcholine (ACh) on serotonin (5-HT) precontraction by prior preincubation with levosimendan (LV) in vessel segments in the sham and subarachnoid hemorrhage (SAH) groups. ACh elicited a dose-dependent vasorelaxation. Shown are the concentration-effect curves (CECs) for each group with LV. LV reduced the Emax dose-dependently. ACh triggered a dose-dependent relaxation in the SAH day 3 and SAH day 5 groups. Shown are the CECs for each group with LV. Likewise, LV reduced the Emax dose-dependently, so that the relaxative effects of LV in the SAH groups were even stronger than in the sham groups. *P<0.05 vs solvent control; #P<0.05 vs Sham LV 10−5 M.
SAH day 3 segments (Emax 76%) as well as day 5 (Emax 79%) segments (figure 1, table 2) showed a stronger vasorelaxation compared with the sham groups (figure 1). The maximal vasorelaxation between SAH day 3 and day 5 was not significantly changed (P=0.9) (table 2). In the SAH day 3 segments, administration of ACh 10−8 M (Emax ACh 10−8 M 31%, P=0.002) and 10−7 M (Emax ACh 10−7 M 50%, P=0.02; table 3) showed a statistically enhanced vasorelaxation as compared with the sham group with LV 10−5 M (Emax ACh 10−8 M 5%; Emax ACh 10−7 M 17%). Furthermore, the SAH day 3 segments showed a statistically enhanced vasorelaxation (Emax ACh 10−8 M 31%, P=0.004; Emax ACh 10−7 M 50%, P=0.03; table 3) compared with the solvent control group at corresponding dosages (Emax ACh 10−8 M 6%; Emax ACh 10−7 M 17%).
Relaxative assessment (acetylcholine) after preincubation with levosimendan and precontraction by serotonin under physiological and pathophysiological conditions post subarachnoid hemorrhage
Detailed analysis of the acetylcholine series in subarachnoid hemorrhage segments
Effect of cumulative LV series on PGF2a 3 x 10−5 M precontracted vessel segments in sham and SAH segments
The solvent control group showed a spontaneous diminution in muscular media tone (Emax 10%).
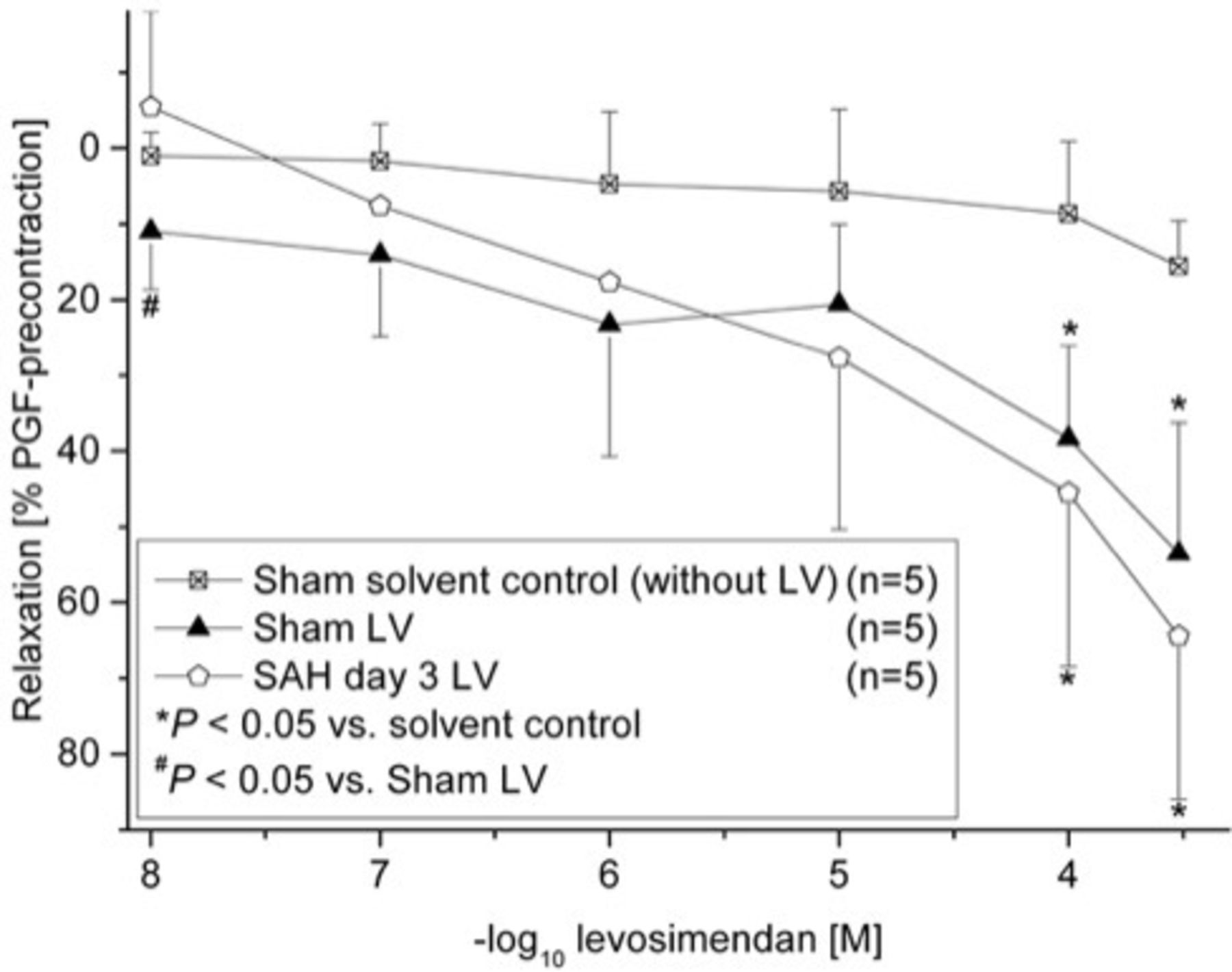
In sham segments, the LV series elicited a dose-dependent vasorelaxation in all segments. Vasorelaxation with LV 10−8 M was significant (P=0.03). For LV 10−4 M, 3×10−4 M vasorelaxation compared with the solvent control group was also significantly enhanced (LV 10−4 M 38%, P=0.03; LV 3×10−4 M 54%, P=0.04). The maximum vasorelaxation was significantly enhanced compared with the solvent control group (54%, P=0.004, pD2 (−log10EC50) = 5.38), whereas no significant changes in the pD2 were noted, suggesting that the induced contraction seemed to be altered in a non-competitive way (figure 2, table 4).

{kind=link}
{kind=link}
Effect of levosimendan (LV) series after precontraction with PGF2a in the sham and subarachnoid hemorrhage (SAH) groups. An LV series, in the sham and SAH day 3 groups, dose-dependently induced a significant maximal vasorelaxation as compared with the solvent control group. *P<0.05 vs solvent control; #P<0.05 vs Sham LV.
Relaxative assessment (levosimendan series) after precontraction by prostaglandin F2alpha under physiological and pathophysiological conditions post subarachnoid hemorrhage
In SAH segments, the LV series also triggered a dose-dependent vasorelaxation. For LV 10−4 M, 3×10−4 M vasorelaxation compared with the solvent control series was significantly enhanced (LV 10−4 M 46%, P=0.01; LV 3×10−4 M 64%, P=0.01). The Emax was significantly enhanced compared with the solvent control group as well (64%, P=0.0008, pD2 (-log10EC50) = 5.38), but pD2 was not significantly altered as compared with the sham segments (figure 2, table 4).
Discussion
Our study findings indicate that LV has the ability to ameliorate cerebral vasoconstriction after experimentally induced SAH. Of note, LV did not influence the contractile response to 124 mM KCl in the groups with or without the induction of SAH (table 1). This might be due to the fact that 0.124 M KCl is present in a more than 1 000 000-fold concentration, leading to a cell membrane depolarization with a strong and long-lasting contraction of the muscular media. So, a certain bias in analyzing the results can be excluded.
After SAH, multiple receptors located on smooth muscle or endothelial cells are of certain pathophysiological interest. For example, the vasocontractile muscular ETA-R are upregulated, whereas the endothelial vasorelaxant ETB1-R are functionally impaired.14 Furthermore, besides increased ET-1 synthesis, vasocontractile angiotensin-II type-1 receptors as well as vasocontractile 5-HT receptors, located on the muscular media, are upregulated as well.15 In addition to 5-HT receptor upregulation post SAH, 5-HT is upregulated as well.16 Similar findings have already been described by Lobato et al in a cat model of SAH.17 The present data demonstrate, in sham segments and after prior preincubation with LV, a strong and dose-dependent ACh-mediated vasorelaxation in 5-HT precontracted vessels (figure 1). For LV 10−5 M, an Emax of 48% was observed, whereas for LV 10−4 M, vasorelaxation to ACh was strongly enhanced to 65%. Interestingly, a stronger vasorelaxation in the same experimental setting was observed in the SAH group. For day 3 and day 5 segments, a vasorelaxation Emax of 76% and 79% was determined, respectively (figure 1).
As already mentioned, after SAH the functional integrity of ETB1-R is impaired.18 Normally, after binding of ET-1, the vasorelaxant pathway via ACh, cGMP, and NO is activated. Binding of the ligand in experimental settings is performed with the use of S6c, with NO release simulated by SNP.1 Our group has already published data that clearly support a significant activation of the vasorelaxant subparts of the ETB1-R pathway for S6c, cGMP, and SNP after SAH compared with a corresponding solvent control group. For S6c, a significant vasorelaxation after prior preincubation with LV 10−4 M was observed (Emax 56%) as compared with the solvent group (Emax 20%). For ACh, after prior preincubation with LV 10−4 M, enhanced relaxation to an Emax of 87% was observed as well. A cGMP series, with prior LV 10−4 M incubation, reached a significant enhanced vasorelaxation of 52%, compared with an Emax of 26% in the solvent control group. For SNP, under LV 10−4 M, a significant relaxation Emax of 86% was noted, compared with 51% spontaneous relaxation in the solvent control group.9 So, besides its anti-inflammatory components, LV seems to have beneficial influences regarding the restoration of the vasorelaxant ETB1-R.
After SAH, the upregulation of eicosanoids in cerebrospinal fluid (CSF), such as PGF2a, is already known to participate in the pathogenesis of DCVS.7 Similar findings have been confirmed by Seifert et al, suggesting that pre- and postoperative monitoring of CSF levels of 6-keto-PGF1α and especially TXB2 may serve as possible indicators for the detection of patients at risk of developing DCVS.19 With additional data from our study group, we underline that preincubation with LV 10−4 M compared with a solvent control group (Emax 56%) significantly prevented PGF2a-mediated vasoconstriction in sham segments (Emax 28%) (figure 2). After SAH day 3 and day 5, LV 10−4 M preincubation significantly prevented vasoconstriction as well (22% to 26%), similar to the sham group with LV 10−4 M (figure 2).10 With the present data, we clearly underline these findings by showing that LV administration dose-dependently reduced PGF2a-mediated vasoconstriction to an Emax of 64% in the SAH group, and to an Emax of 54% in the sham group. These findings confirm an anti-inflammatory effect of LV,20 besides its already known effects in the cerebral and cardiac vasculature. Until now, the issue of inflammation in aneurysm walls has also been a subject of intensive research. In this context, after SAH the role of an upregulated inflammatory cerebral microenvironment in aneurysm formation and rupture is undisputed.21–23 Here, LV might be an interesting pharmacological agent in analyzing effects on concentrations/amounts of prostaglandin E2 synthase-1, cyclooxygenase-2, and/or neutrophils in histological samples of the basilar artery or aneurysms walls with different wall characteristics in other animal models in future experiments.23
Certainly, next to CI with DCVS, delayed ischemia and neurodegeneration, a multifactorial process is responsible for poor patient outcomes after SAH, including cortical spreading depressions, hydrocephalus, early brain injury, and impaired cerebral autoregulation.1
Role of LV in the clinical context
LV is an already well-established drug in clinical practice for the treatment of congestive heart failure.20 Multiple anti-inflammatory effects in patients with severe heart failure are known also.24
One severe complication after SAH is the development of takotsubo cardiomyopathy, which in its clinical course and onset is similar to other types of congestive heart failures.9 25 Additionally, in cases of symptomatic DCVS, the use of catecholamines as inotropic substances for providing hypertension is not feasible. LV, a calcium-channel sensitizer, upregulates cardiac sensitivity of the muscular contractile proteins, triggered by its binding to cardiac troponin C. This provides positive inotropic effects without affecting diastolic relaxation. A possible explanation therefore might be that the transmembraneous calcium flow does not exceed pharmacological relevant concentrations. In addition, LV opens ATP-sensitive potassium channels in vascular smooth muscle cells, thus providing vasorelaxation as well.26 Thus, LV could positively and beneficially influence myocardial contractility in selected cases, and even alleviate DCVS mediated by inflammatory vasoconstrictors like 5-HT and PGF2a.27
Study limitations
The pathophysiological mechanisms after SAH may be divided into an acute phase after the initial bleeding event, including increased intracranial pressure, reduced cerebral blood flow (CBF), and delayed sequelae of the subarachnoid blood clot. Analyzing the acute phase pressure-dependent injection models seem to mimic the pathological consequences superior to those which are volume dependent. However, the development of delayed mechanisms, like reduced CBF due to DCVS or other pathological mechanisms, seems mainly to be dependent on the amount and duration of the subarachnoid blood. Accordingly, the double cisterna magna blood injection model, in which a sufficient subarachnoidal blood distribution and contact time is achieved, might be predisposed for investigating the delayed consequences of SAH. LV, a lipophilic substance, has a molecular weight of 280 daltons.28 In our experiments, the highest concentration of LV given was 10−4 M (0.0001 M). Additively, LV 10−4 M was already used in other trials analyzing the contractility of pulmonary arterial vessels in rats and humans, demonstrating that ET-1-mediated precontraction is strongly diminished by LV via opening ATP-sensitive potassium channels.29 Correspondingly we applied a dose of 28 mg (= 28 000 mcg). Normally, in terms of treating congestive heart failure, clinicians start a LV infusion with 0.1 mcg/kg/min for 24 hours, and some even start with 0.2 mcg/kg/min for 60 min in order to reach the desired therapeutic effect more rapidly.30 For a standardized person weighting 75 kg, 7.5 mcg/min has to be applied for a continuous infusion of 0.1 mcg/kg/min and150 mcg/min for a continuous infusion of 0.2 mcg/kg/min. Multiplied by 24 hours, this means a maximal dosage of 10 800 mcg given for an infusion rate of 0.1 mcg/kg/min and 21 600 mcg for an infusion rate of 0.2 mcg/kg/min. For an obese patient (ie, 100 kg), 28 800 mcg for an infusion rate of 0.2 mcg/kg/min are required. So, dosages at least are more or less comparable. Nevertheless, in terms of safety, in possible clinical translation clinicians should probably start with the recommended continuous infusion rate, under cardiac monitoring in an intensive care unit, titrated to the desired effect.
Nevertheless, the main limitation of this study is the focus on in vitro tension studies only with the inability to provide more data on other aspects regarding the multifactorial process being responsible for poor patients’ outcome after SAH, for example, cerebral microvasospasm, impaired cerebral autoregulation, cortical spreading depressions, and/or other inflammatory parameters as concentrations of prostaglandin E2 synthase-1 and cyclooxygenase-2 in blood, cerebrospinal fluid, or the vessel wall of the basilar artery, as well as indirect signs like the invasion of neutrophils. Furthermore, swelling of the vascular cells might have been triggered by exchanging sodium chloride for potassium chloride; here, sucrose added as adjunct could create a more isotonic solution.
Conclusions
LV is able to significantly antagonize 5-HT- and PGF2a-mediated inflammation and inflammatory cerebral vasospasm. Interestingly, relaxation was more pronounced in the SAH groups. Besides these effects, LV might be a treatment option in patients suffering from takotsubo cardiomyopathy after SAH, where the use of catecholamines is contraindicated. Therefore, LV might be a valuable option in selected cases of patients after SAH.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplemental information.
Ethics statements
Patient consent for publication
Ethics approval
The project was performed according to the Animal Research: Reporting of In Vivo Experiments (ARRIVE) guidelines and was performed in accordance with the permission of the local ethics committee (Gen. Nr. F 138/12, 28 December 2009. Regierungspräsidium Darmstadt, Germany) and in compliance with the German Federal Guidelines for animal experiments.
References
Footnotes
SW and LA contributed equally.
Contributors Study conception and design: SW, JK. Experimental procedures: SW, JK. Drafting the article: SW, LA, JK. Statistical analysis and data interpretation: SW, LA, JK. Critically revising the article: SW, LA, JM, SK, GAS, SM, JK. SW and LA contributed equally and share first authorship.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.