Article Text

Abstract
Background First pass reperfusion (FPR), that is, excellent reperfusion (expanded treatment in cerebral ischemia (eTICI) 2C-3) in one pass, after endovascular treatment (EVT) of an occluded artery in the anterior circulation, is associated with favorable clinical outcome, even when compared with multiple pass excellent reperfusion (MPR). In patients with posterior circulation ischemic stroke (PCS), the same association is expected, but currently unknown. We aimed to assess characteristics associated with FPR and the influence of FPR versus MPR on outcomes in patients with PCS.
Methods We used data from the MR CLEAN Registry, a prospective observational study. The effect of FPR on 24-hour National Institutes of Health Stroke Scale (NIHSS) score, as percentage reduction, and on modified Rankin Scale (mRS) scores at 3 months, was tested with linear and ordinal logistic regression models.
Results Of 224 patients with PCS, 45 patients had FPR, 47 had MPR, and 90 had no excellent reperfusion (eTICI <2C). We did not find an association between any of the patient, imaging, or treatment characteristics and FPR. FPR was associated with better NIHSS (−45% (95% CI: −65% to −12%)) and better mRS scores (adjusted common odds ratio (acOR): 2.16 (95% CI: 1.23 to 3.79)) compared with no FPR. Outcomes after FPR were also more favorable compared with MPR, but the effect was smaller and not statistically significant (NIHSS: −14% (95% CI: −51% to 49%), mRS acOR: 1.50 (95% CI: 0.75 to 3.00)).
Conclusions FPR in patients with PCS is associated with favorable clinical outcome in comparison with no FPR. In comparison with MPR, the effect of FPR was no longer statistically significant. Nevertheless, our data support the notion that FPR should be the treatment target to pursue in every patient treated with EVT.
- stroke
- thrombectomy
- brain
- intervention
Data availability statement
In compliance with the General Data Protection Regulation, source data are not available for other researchers. Information about analytic methods, study materials and scripts of the statistical analyses are available from the corresponding author on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution 4.0 Unported (CC BY 4.0) license, which permits others to copy, redistribute, remix, transform and build upon this work for any purpose, provided the original work is properly cited, a link to the licence is given, and indication of whether changes were made. See: https://creativecommons.org/licenses/by/4.0/.
Statistics from Altmetric.com
Introduction
Excellent reperfusion (expanded treatment in cerebral ischemia (eTICI) 2C-3) in one pass, first pass reperfusion (FPR), after endovascular treatment (EVT) of an occluded artery in the anterior circulation, is associated with favorable clinical outcome.1 2 In comparison with patients with anterior circulation ischemic stroke, patients with posterior circulation ischemic stroke (PCS) have not been studied extensively. Variables associated with outcome and reperfusion in patients with PCS are heterogeneous.3 It has been suggested that patients with PCS may have a different underlying pathophysiology than patients with anterior circulation ischemic stroke, which secondarily influences reperfusion and outcomes.3 Previous studies showed that in patients with a basilar artery occlusion, successful reperfusion is a strong predictor of favorable 90-day outcome.4–8 However, other studies showed more heterogeneity of clinical outcome despite high reperfusion rates.9–11
No studies have been published about the association between FPR and outcomes in patients with PCS. In patients with anterior circulation ischemic stroke, FPR is associated with favorable outcome, independently of patient, imaging, and treatment characteristics, even when compared with multiple pass excellent reperfusion (MPR).1 12 In patients with PCS, one might expect the same association, but this is currently unknown. Knowledge about the association of FPR with favorable clinical outcome in patients with PCS is needed to use FPR as a benchmark of good quality PCS care. We aimed to assess characteristics associated with FPR and assess the influence of FPR compared with MPR on clinical outcome in patients with PCS.
Methods
We used data from the Multicenter Randomized Clinical Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry. This was a prospective observational study in all 18 centers performing EVT in the Netherlands. All patients undergoing EVT for acute ischemic stroke in the anterior and posterior circulation were registered, except for those who were treated in the BASICS trial.13 Detailed study design and methods have been described previously.14 15
Patients
From the MR CLEAN Registry, we included patients aged 18 years or older, who had a symptomatic occlusion of the vertebral, basilar, or posterior cerebral artery confirmed by baseline computed tomography angiography. These data concerned patients who were treated with EVT between March 16, 2014 and December 31, 2018.
Definition of FPR, clinical, imaging, and treatment characteristics
An imaging core laboratory analyzed all patient imaging. The members of the core laboratory were blinded to all clinical data. Reperfusion grade was measured according to the eTICI scale on final digital subtraction angiography (DSA) by the core laboratory. The number of attempts used to achieve reperfusion was based on the information given by the local treating interventionalist.
FPR was defined as a single pass of the device, without rescue treatment with intra-arterial thrombolytics, resulting in complete or near-complete reperfusion of the large vessel occlusion and its downstream territory: eTICI 2C-3. MPR was defined as eTICI 2C-3 after more than one pass or after one pass followed by rescue treatment with intra-arterial thrombolytics. No excellent reperfusion (NER) was defined as eTICI <2C independently of the number of passes.
Patient characteristics included: age, sex, history of atrial fibrillation, history of hypertension, history of diabetes mellitus, history of myocardial infarction, history of peripheral artery disease, history of stroke, history of hyperlipidemia, smoking, use of antiplatelet agents, use of vitamin K antagonists, use of direct oral anticoagulants, National Institutes of Health Stroke Scale (NIHSS) score at baseline, and pre-stroke modified Rankin Scale (mRS) score.
Imaging characteristics (scored by the core laboratory) included: level of obstruction, hyperdense artery sign, posterior circulation collateral score,16 posterior circulation Alberta Stroke Program Early CT Score (pc-ASPECTS),17 and vertebral artery dissection.
Treatment characteristics included: estimated time of large vessel occlusion (eLVO) to presentation at intervention hospital, presentation at intervention hospital to groin time, intravenous alteplase treatment, general anesthesia, and used device.
In patients with transient or mild neurological symptoms with secondary worsening consistent with the large vessel occlusion, the moment of secondary worsening was considered as the eLVO.15
Outcomes
The percentage change in 24-hour NIHSS (±12 hours) was used as the primary outcome. This has been shown to be more closely related to EVT and reperfusion than the mRS score at 3 months, and has a good predictive value for long-term stroke outcome.18 We used the mRS scores at 3 months as a secondary outcome. Study staff were instructed to assess mRS scores at 90 days (±14 days).
Missing data
All baseline data were reported as crude. If successful reperfusion was not achieved during EVT, we used the time of last contrast bolus injection as the final reperfusion time. For the use in regression models we imputed missing data using multiple imputation with R (package, MICE) based on relevant covariates and outcomes. Any mRS score of 0 to 5 at follow-up assessed within 30 days of symptom onset was considered invalid and treated as missing.
Statistical analysis
We compared baseline characteristics of patients with FPR with patients without FPR using descriptive statistics. To investigate the association between patient, imaging, and treatment characteristics and FPR we used an univariable logistic regression model and selected all variables with a P value ≤0.2. These selected variables were used in a multivariable logistic regression model with a backward stepwise selection procedure with three steps. In each additional step, variables with a P value >0.2 were dropped, except for age and sex which were forced into the model. In step one, we tested all patient characteristics. In step two, we added all imaging characteristics to the remaining variables from step one. In step three, we added treatment characteristics to the remaining variables from step two. The final model consisted of all variables with a P value ≤0.2 and age and sex.
We analyzed the association between FPR and outcomes, adjusted for characteristics associated with FPR. First, we compared outcomes between FPR and no FPR. Second, we compared FPR with MPR. We used a linear regression model to analyze the NIHSS score at 24 hours and presented percentage change with 95% confidence intervals (CIs). Patients who had died before the time point of NIHSS assessment was reached, received the maximum NIHSS score of 42. The NIHSS was then log10 transformed, to better meet the assumption of normally distributed residuals in linear regression.18 We added one point to the NIHSS, so the original NIHSS of 0 was equivalent to log10 NIHSS +1. We used an ordinal logistic regression model to analyze the outcome mRS at 3 months and presented common odds ratios (ORs) with 95% CIs. We used the inverse of the mRS score for each patient. Lastly, we carried out a sensitivity analyses with a linear mixed model with random intercepts for hospitals and the primary outcome, NIHSS at 24 hours, to account for patient clustering within each hospital. All statistical analyses were performed with R statistical software (version 3.6.1).
Results
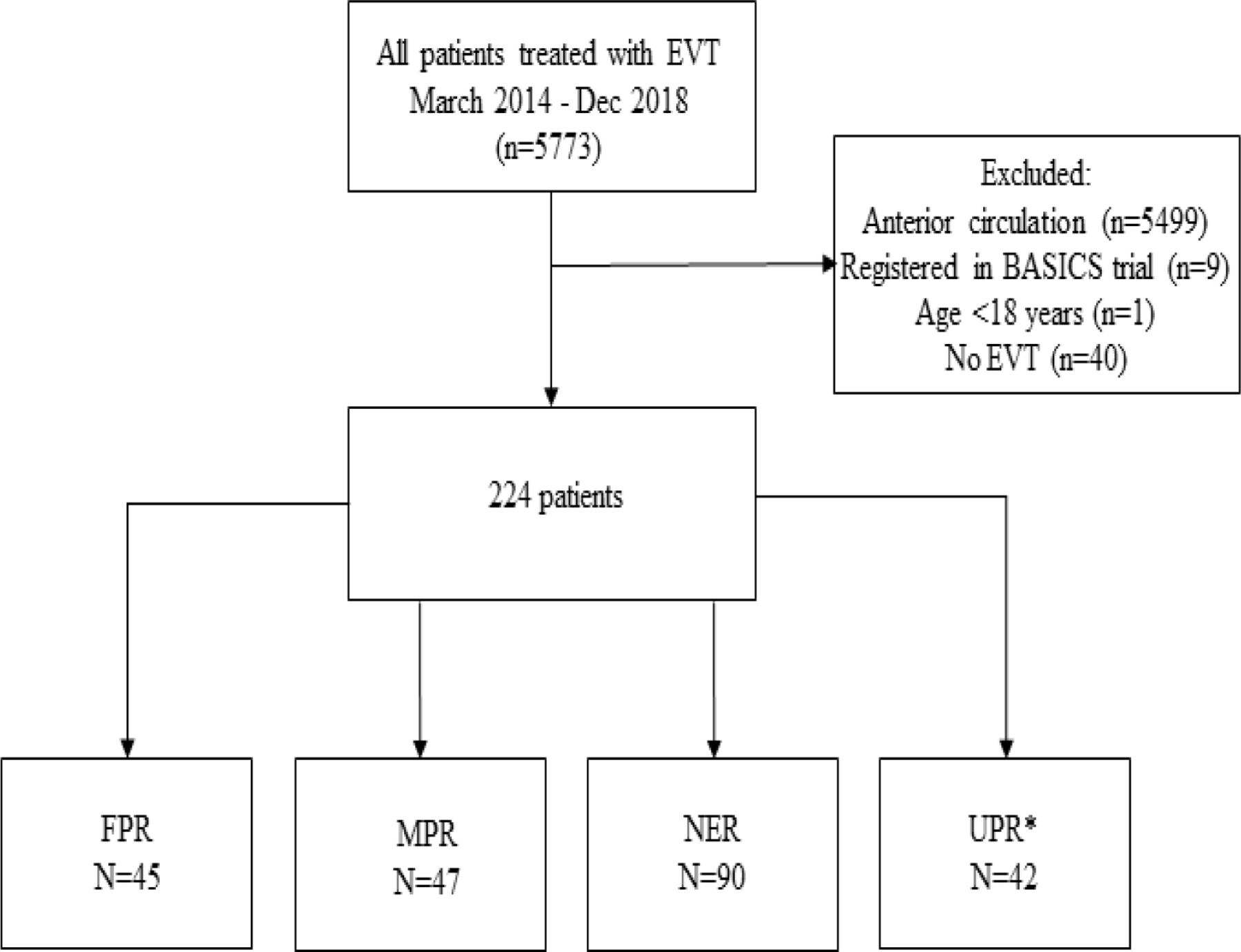
Of all the patients in the MR CLEAN Registry, 264 adult patients had PCS. We excluded 40 patients who did not receive mechanical thrombectomy, because arterial access to the intracranial vasculature was not achieved or first DSA before EVT showed (spontaneous) reperfusion. Therefore, 224 patients were included (figure 1). FPR was achieved in 45/224 (20%) patients, MPR in 47/224 (21%), and NER in 90/224 (40%) patients. In 42 patients (19%) there was a missing number of attempts or missing eTICI score. These patients were allocated to the unclassified reperfusion (UPR) group. Baseline characteristics of the FPR, MPR, NER, and UPR group are shown in table 1.
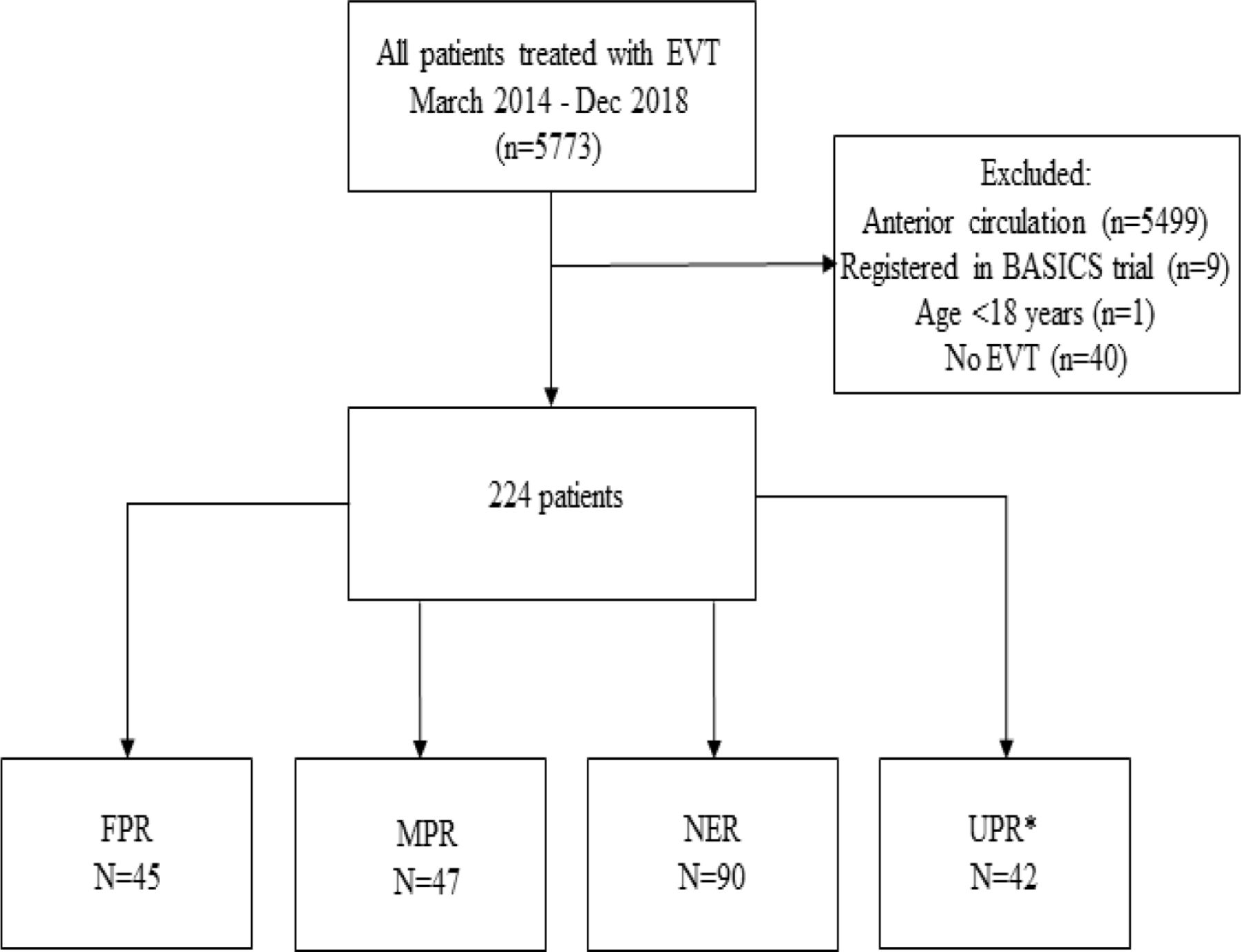
Flowchart of MR CLEAN Registry patients selected for analysis. *Thirty-four patients with a missing number of attempts, six patients with a missing eTICI score, and two patients with a missing number of attempts and missing eTICI score. eTICI, expanded treatment in cerebral ischemia; EVT, endovascular treatment; FPR, first pass reperfusion; MPR, multiple pass reperfusion;MR CLEAN, Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke in the Netherlands; NER, no excellent reperfusion; UPR, unclassified pass reperfusion.
Baseline characteristics of patients with first pass reperfusion, multiple pass reperfusion, no excellent reperfusion, and unclassified reperfusion
Characteristics associated with FPR
We analyzed the association of patient, imaging, and treatment characteristics with FPR compared with no FPR (MPR+NER). In the backward stepwise selection procedure only a history of hyperlipidemia was selected, next to age and sex which were forced into the model. None of these variables were associated with FPR (history of hyperlipidemia adjusted odds ratio (aOR) 1.17 (95% CI: 0.99 to 1.39)). We also analyzed the association of patient, imaging, and treatment characteristics with FPR contrasted with MPR. We selected age, sex, history of hyperlipidemia, and baseline pc-ASPECTS from the backward stepwise selection procedure. However, none of these variables were associated with FPR (history of hyperlipidemia aOR 1.27 (95% CI: 0.98 to 1.63), pc-ASPECTS aOR 1.04 (95% CI: 0.95 to 1.13)).
Association between FPR and NIHSS at 24 hours
In the univariable regression analysis, FPR compared with no FPR led to a statistically significant decrease in 24-hour NIHSS score of −45% (95% CI: −64 to −14) (table 2). Compared with MPR the reduction in 24-hour NIHSS score was −22% (95% CI: −54 to 32). In the multivariable analyses, we adjusted for characteristics selected from the backward stepwise selection procedure. FPR still led to a reduction in 24-hour NIHSS score compared with no FPR (−45% (95% CI: −65 to −12)) and compared with MPR (−14% (95% CI: −51 to 49)). We found no differences in the results when we adjusted for patient clustering within each hospital (online supplemental data table S1) (ICC=0.05).
Supplemental material
Univariable and multivariable linear/ordinal logistic regression for the association between first pass reperfusion (FPR) and 24-hour National Institutes of Health Stroke Scale score and FPR and modified Rankin Scale score at 3 months
Procedure time for FPR was shorter than for no FPR (table 1). When procedure time was added to the adjustments there was still a benefit of FPR compared with no FPR (−39% (95% CI: −63 to −2)) and compared with MPR (−6% (95% CI: −53 to 89)).
Association between FPR and MRS score at 3 months
In the univariable regression analyses, FPR led to more favorable mRS scores at 3 months compared with no FPR (cOR 1.96 (95% CI: 1.14 to 3.39)) and compared with MPR (cOR 1.33 (95% CI: 0.69 to 2.53)) (table 2). The shift on the mRS scale is shown in figure 2. In the multivariable analysis, FPR led to more favorable mRS scores at 3 months compared with no FPR (acOR 2.16 (95% CI: 1.23 to 3.79)) and compared with MPR (acOR 1.50 (95% CI: 0.75 to 3.00)). When procedure time was added to the adjustments the effect of FPR over MPR was reduced (acOR 1.19 (95% CI: 0.56 to 2.55)).

{kind=link}
{kind=link}
Modified Rankin Scale (mRS) scores at 3 months, first pass reperfusion (FPR) versus no FPR and FPR versus multiple pass reperfusion (non-imputed data). eTICI, expanded thrombolysis in cerebral infarction; FPR, first pass reperfusion; MPR, multiple pass reperfusion; no FPR, MPR (eTICI ≥2C in multiple passes) + no excellent reperfusion (NER) (eTICI <2C, independent of number of passes).
Discussion
In our study, FPR was associated with favorable clinical and functional outcomes. There were no patient, imaging, or treatment characteristics associated with FPR. In a study of patients with PCS treated with aspiration first, a history of diabetes, onset-to-groin time, and cardioembolic etiology were found as predictors of FPR (in this study defined as eTICI ≥2B in one attempt).19 We did not find such associations in our analysis, but no separate analysis for aspiration first and stent retriever thrombectomy were done. In two systematic reviews, aspiration as first attempt appeared to be superior to stent retriever in achieving modified treatment in cerebral infarction (mTICI) 2b-3 in patients with PCS,3 20 which is not in line with our results. However, in the ASTER trial where patients with an anterior circulation ischemic stroke were randomly assigned to EVT with a stent retriever or aspiration, similar rates of FPR were achieved in both groups.21 In patients with an anterior circulation ischemic stroke there is a strong association between location of the occluded artery and FPR.1 22 We did not find an association between FPR and the location of the occluded artery in the posterior circulation. However, most of the patients in our cohort had a basilar artery occlusion (177/224, 79%), whereas 31 patients (14%) had a posterior cerebral artery occlusion and only 12 patients (5%) had a vertebral artery occlusion. In the FPR group there was only one patient with a vertebral artery occlusion. We do not have an explanation for this low number, probably this is due to chance. Our study population is heterogeneous as regards the location of the occluded artery. The likelihood of a good outcome may differ between these localizations, but relative effects of intervention less so. We therefore do not think that location influenced our results.
The association between FPR and 24-hour NIHSS is comparable to our results in patients with anterior circulation ischemic stroke (compared with no FPR; −45% vs −37% compared with MPR −14% vs −23%).12 In contrast to patients with anterior circulation ischemic stroke, in patients with PCS there is no significant benefit of FPR over MPR in our results. In a previous study with a pooled analysis of patients with either anterior or posterior circulation stroke, no differences in outcome (dichotomized mRS) between the FPR and MPR group were noted.19 In a study with a small number of patients (FPR n=19 and MPR n=13) with a basilar artery occlusion there was also no difference in outcomes between the FPR and MPR group.23 There are, however, no studies describing the effect of FPR versus MPR on outcome in a larger sample of patients with only PCS. The differences in effect of FPR over MPR on outcome between patients with anterior circulation stroke and patients with PCS suggests a different pathophysiology, vascular anatomy, and outcomes in patients with PCS compared with patients with anterior circulation ischemic stroke.3 Although the effect of FPR over MPR is not significant as regards the 24-hour NIHSS and mRS score at 3 months, the observed percentage change in NIHSS and odds of a favorable mRS score is high. Therefore, we may conclude that FPR should be the treatment target to pursue in every patient treated with EVT.
The effect of FPR over MPR and NER can be partly explained by a shorter procedure time. We showed that the effect of FPR on outcomes was not completely reduced when we adjusted for procedure time. A higher maneuver count is associated with a poor outcome despite successful recanalization.24 Explanations for these poor outcomes could be an increase in complications, vessel wall damage, thrombus migration, and microembolization.1 25 26
Limitations
Parallel to the data collection of the MR CLEAN Registry, the BASICS trial was performed. Of all the hospitals in the MR CLEAN Registry, 10 participated in the BASICS trial and eight did not participate in the BASICS trial. There could be some selection bias in our cohort because we only collected data of patients treated with EVT outside the BASICS trial. In separate analyses of our data there were no differences in patient characteristics and outcomes between patients treated in a BASICS trial center and patients treated in an non-BASICS trial center.15 Moreover, our cohort is similar as regards baseline characteristics and outcomes to other registries on EVT for patients with PCS.5 15 27 28
All our imaging was assessed by an independent core laboratory. We used very strict definitions for these assessments, and when the quality of imaging was low or there were only a few images available the imaging variables were scored as missing. Registries in general are prone to missing values. However, all data were verified by our study coordinators, and we made every effort to retrieve the missing data.13 To use the missing data in a responsible way and to avoid bias, the missing values were imputed by means of multiple imputation.
During the inclusion period of the MR CLEAN Registry there was no clear evidence for a benefit of EVT over best medical management on outcome in patients with a basilar artery occlusion.29 Therefore, the treatment of patients with PCS differed between hospitals. This could result in bias and a clustering effect. The sensitivity analyses with a linear mixed model, to account for this clustering, did not show any differences in outcome compared with the results of the linear regression model.
Another limitation is the assessment of the eTICI score, which is less reliable in the posterior circulation. The assessment is more difficult due to the interference with abundant collateral flows, incomplete visualization of the perforating arteries to the brain stem, and the necessity to consider the antegrade flow from the anterior circulation.30 Our core laboratory was well instructed to assess the eTICI score. However, a reliable eTICI score is fundamental for the definition of FPR. Further research is needed on how to assess the eTICI score in the posterior circulation.
Conclusions
FPR in patients with PCS is associated with favorable clinical outcome in comparison with no FPR. In comparison with MPR, the effect of FPR was no longer statistically significant. Nevertheless, our data support the notion that FPR should be the treatment target to pursue in every patient treated with EVT.
Data availability statement
In compliance with the General Data Protection Regulation, source data are not available for other researchers. Information about analytic methods, study materials and scripts of the statistical analyses are available from the corresponding author on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
The central medical ethics committee of the Erasmus MC, University Medical Center Rotterdam, the Netherlands, evaluated the study protocol and granted permission to carry out the study as a registry (MEC-2014-235). With this approval the study was approved by the research board of each participating center. At University Medical Center Utrecht, approval to participate in the study has been obtained from their own research board and ethics committee. The need for individual patient consent has been waived.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Strokologist
Collaborators MR CLEAN Registry investigators: Executive committee: Diederik W.J. Dippel (Department of Neurology, Erasmus MC, University Medical Center); Aad van der Lugt (Department of Radiology, Erasmus MC, University Medical Center); Charles B.L.M. Majoie (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Yvo B.W.E.M. Roos (Department of Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Robert J. van Oostenbrugge (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Wim H. van Zwam (Department of Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Jelis Boiten (Department of Neurology, Haaglanden MC, the Hague); Jan Albert Vos (Department of Radiology, Sint Antonius Hospital, Nieuwegein). Study coordinators: Ivo G.H. Jansen (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Maxim J.H.L. Mulder (Department of Neurology; Radiology, Erasmus MC, University Medical Center) ;Robert- Jan B. Goldhoorn (Department of Neurology, Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Kars C.J. Compagne (Department of Radiology, Erasmus MC, University Medical Center); Manon Kappelhof (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Josje Brouwer (Department of Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Sanne J. den Hartog (Department of Neurology, Erasmus MC, University Medical Center; Radiology, Erasmus MC, University Medical Center); Wouter H. Hinsenveld (Department of Neurology, Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)). Local principal investigators: Diederik W.J. Dippel (Department of Neurology, Erasmus MC, University Medical Center); Bob Roozenbeek (Department of Neurology, Erasmus MC, University Medical Center); Aad van der Lugt (Department of Radiology, Erasmus MC, University Medical Center); Charles B.L.M. Majoie (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Yvo B.W.E.M. Roos (Department of Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Bart J. Emmer (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Jonathan M. Coutinho (Department of Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Wouter J. Schonewille (Department of Neurology, Sint Antonius Hospital, Nieuwegein); Jan Albert Vos (Department of Neurology, Sint Antonius Hospital, Nieuwegein); Marieke J.H. Wermer (Department of Neurology, Leiden University Medical Center); Marianne A.A. van Walderveen (Department of Radiology, Leiden University Medical Center); Adriaan C.G.M. van Es (Department of Radiology, Leiden University Medical Center); Julie Staals (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Robert J. van Oostenbrugge (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Wim H. van Zwam (Department of Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Jeannette Hofmeijer (Department of Neurology, Rijnstate Hospital, Arnhem); Jasper M. Martens (Department of Radiology, Rijnstate Hospital, Arnhem); Geert J. Lycklama à Nijeholt (Department of Radiology, Haaglanden MC, the Hague); Jelis Boiten (Department of Neurology, Haaglanden MC, the Hague); Sebastiaan F. de Bruijn (Department of Neurology, HAGA Hospital, the Hague); Lukas C. van Dijk (Department of Radiology, HAGA Hospital, the Hague); H. Bart van der Worp (Department of Neurology, University Medical Center Utrecht); Rob H. Lo (Department of Radiology, University Medical Center Utrecht); Ewoud J. van Dijk (Department of Neurology, Radboud University Medical Center, Nijmegen); Hieronymus D. Boogaarts (Department of Neurosurgery, Radboud University Medical Center, Nijmegen); J. de Vries (Department of Neurology, Isala Klinieken, Zwolle); Paul L.M. de Kort (Department of Neurology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Julia van Tuijl (Department of Neurology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Jo P. Peluso (Department of Radiology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Puck Fransen (Department of Neurology, Isala Klinieken, Zwolle); Jan S.P. van den Berg (Department of Neurology, Isala Klinieken, Zwolle); Boudewijn A.A.M. van Hasselt (Department of Radiology, Isala Klinieken, Zwolle); Leo A.M. Aerden (Department of Neurology, Reinier de Graaf Gasthuis, Delft); René J. Dallinga (Department of Radiology, Reinier de Graaf Gasthuis, Delft); Maarten Uyttenboogaart (Department of Neurology, University Medical Center Groningen); Omid Eschgi (Department of Radiology, University Medical Center Groningen); Reinoud P.H. Bokkers (Department of Radiology, University Medical Center Groningen); Tobien H.C.M.L. Schreuder (Department of Neurology, Atrium Medical Center, Heerlen); Roel J.J. Heijboer (Department of Radiology, Atrium Medical Center, Heerlen); Koos Keizer (Department of Neurology, Catharina Hospital, Eindhoven); Lonneke S.F. Yo (Department of Radiology, Catharina Hospital, Eindhoven); Heleen M. den Hertog (Department of Neurology, Isala Klinieken, Zwolle); Emiel J.C. Sturm (Department of Neurology, Medisch Spectrum Twente, Enschede;); Paul J.A.M. Brouwers (Department of Neurology, Medisch Spectrum Twente, Enschede). Imaging assessment committee: Charles B.L.M. Majoie (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam) (chair); Wim H. van Zwam (Department of Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Aad van der Lugt (Department of Radiology, Erasmus MC, University Medical Center); Geert J. Lycklama à Nijeholt (Department of Radiology, Haaglanden MC, the Hague); Marianne A.A. van Walderveen (Department of Radiology, Leiden University Medical Center); Marieke E.S. Sprengers (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Sjoerd F.M. Jenniskens (Department of Radiology, Radboud University Medical Center, Nijmegen); René van den Berg (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Albert J. Yoo (Department of Radiology, Texas Stroke Institute, Texas, United States of America); Ludo F.M. Beenen (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Alida A. Postma (Department of Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Stefan D. Roosendaal (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Bas F.W. van der Kallen (Department of Radiology, Haaglanden MC, the Hague); Ido R. van den Wijngaard (Department of Radiology, Haaglanden MC, the Hague); Adriaan C.G.M. van Es (Department of Radiology, Leiden University Medical Center); Bart J. Emmer (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Jasper M. Martens (Department of Radiology, Rijnstate Hospital, Arnhem); Lonneke S.F. Yo (Department of Radiology, Catharina Hospital, Eindhoven); Jan Albert Vos (Department of Radiology, Sint Antonius Hospital, Nieuwegein); Joost Bot (Department of Radiology, Amsterdam UMC, Vrije Universiteit van Amsterdam, Amsterdam); Pieter Jan van Doormaal (Department of Radiology, Erasmus MC, University Medical Center); Anton Meijer (Department of Radiology, Radboud University Medical Center, Nijmegen); Elyas Ghariq (Department of Radiology, Haaglanden MC, the Hague); Reinoud P.H. Bokkers (Department of Radiology, University Medical Center Groningen); Marc P. van Proosdij (Department of Radiology, Noordwest Ziekenhuisgroep, Alkmaar); G. Menno Krietemeijer (Department of Radiology, Catharina Hospital, Eindhoven); Jo P. Peluso (Department of Radiology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Hieronymus D. Boogaarts (Department of Neurosurgery, Radboud University Medical Center, Nijmegen); Rob Lo (Department of Radiology, University Medical Center Utrecht); Dick Gerrits (Department of Radiology, Medisch Spectrum Twente, Enschede); Wouter Dinkelaar (Department of Radiology, Albert Schweitzer Hospital, Dordrecht); Auke P.A. Appelman (Department of Radiology, University Medical Center Groningen); Bas Hammer (Department of Radiology, HAGA Hospital, the Hague); Sjoert Pegge (Department of Radiology, Radboud University Medical Center, Nijmegen); Anouk van der Hoorn (Department of Radiology, University Medical Center Groningen); Saman Vinke (Department of Neurosurgery, Radboud University Medical Center, Nijmegen); Sandra Cornelissen (Radiology, Erasmus MC, University Medical Center); Christiaan van der Leij (Department of Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Rutger Brans (Department of Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)). Writing committee: Diederik W.J. Dippel (Department of Neurology, Erasmus MC, University Medical Center) (chair); Aad van der Lugt (Radiology, Erasmus MC, University Medical Center); Charles B.L.M. Majoie (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Yvo B.W.E.M. Roos (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Robert J. van Oostenbrugge (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Wim H. van Zwam (Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Geert J. Lycklama à Nijeholt (Department of Radiology, Haaglanden MC, the Hague); Jelis Boiten (Neurology, Haaglanden MC, the Hague); Jan Albert Vos (Radiology, Sint Antonius Hospital, Nieuwegein); Wouter J. Schonewille (Department of Neurology, Sint Antonius Hospital, Nieuwegein); Jeannette Hofmeijer (Department of Neurology, Rijnstate Hospital, Arnhem); Jasper M. Martens (Radiology, Rijnstate Hospital, Arnhem); H. Bart van der Worp (Department of Neurology, University Medical Center Utrecht); Rob H. Lo (Radiology, University Medical Center Utrecht). Adverse event committee: Robert J. van Oostenbrugge (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)) (chair); Jeannette Hofmeijer (Department of Neurology, Rijnstate Hospital, Arnhem); H. Zwenneke Flach (Department of Radiology, Isala Klinieken, Zwolle). Trial methodologist: Hester F. Lingsma (Department of Public Health, Erasmus MC, University Medical Center); Research nurses / local trial coordinators: Naziha el Ghannouti (Department of Neurology, Erasmus MC, University Medical Center); Martin Sterrenberg (Department of Neurology, Erasmus MC, University Medical Center); Wilma Pellikaan (Department of Neurology, Sint Antonius Hospital, Nieuwegein); Rita Sprengers (Department of Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Marjan Elfrink (Department of Neurology, Rijnstate Hospital, Arnhem); Michelle Simons (Department of Neurology, Rijnstate Hospital, Arnhem); Marjolein Vossers (Department of Radiology, Rijnstate Hospital, Arnhem); Joke de Meris (Department of Neurology, Haaglanden MC, the Hague); Tamara Vermeulen (Department of Neurology, Haaglanden MC, the Hague); Annet Geerlings (Department of Neurology, Radboud University Medical Center, Nijmegen); Gina van Vemde (Department of Neurology, Isala Klinieken, Zwolle); Tiny Simons (Department of Neurology, Atrium Medical Center, Heerlen); Gert Messchendorp (Department of Neurology, University Medical Center Groningen); Nynke Nicolaij (Department of Neurology, University Medical Center Groningen); Hester Bongenaar (Department of Neurology, Catharina Hospital, Eindhoven); Karin Bodde (Department of Neurology, Reinier de Graaf Gasthuis, Delft); Sandra Kleijn (Department of Neurology, Medisch Spectrum Twente, Enschede); Jasmijn Lodico (Department of Neurology, Medisch Spectrum Twente, Enschede); Hanneke Droste (Department of Neurology, Medisch Spectrum Twente, Enschede); Maureen Wollaert (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Sabrina Verheesen (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); D. Jeurrissen ((Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM))); Erna Bos (Department of Neurology, Leiden University Medical Center); Yvonne Drabbe (Department of Neurology, HAGA Hospital, the Hague); Michelle Sandiman (Department of Neurology, HAGA Hospital, the Hague); Nicoline Aaldering (Department of Neurology, Rijnstate Hospital, Arnhem); Berber Zweedijk (Department of Neurology, University Medical Center Utrecht); Jocova Vervoort (Department of Neurology, Elisabeth-TweeSteden ziekenhuis, Tilburg); Eva Ponjee (Department of Neurology, Isala Klinieken, Zwolle); Sharon Romviel (Department of Neurology, Radboud University Medical Center, Nijmegen); Karin Kanselaar (Department of Neurology, Radboud University Medical Center, Nijmegen); Denn Barning (Department of Radiology, Leiden University Medical Center). Clinical/imaging data aquisition: Esmee Venema (Department of Public Health, Erasmus MC, University Medical Center); Vicky Chalos (Department of Neurology, Public Health, Erasmus MC, University Medical Center); Ralph R. Geuskens (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Tim van Straaten (Department of Neurology, Radboud University Medical Center, Nijmegen); Saliha Ergezen (Department of Neurology, Erasmus MC, University Medical Center); Roger R.M. Harmsma (Department of Neurology, Erasmus MC, University Medical Center); Daan Muijres (Department of Neurology, Erasmus MC, University Medical Center); Anouk de Jong (Department of Neurology, Erasmus MC, University Medical Center); Olvert A. Berkhemer (Department of Neurology, Erasmus MC, University Medical Center; Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam; Radiology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Anna M.M. Boers (Department of Radiology and Nuclear Medicine, Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); J. Huguet (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); P.F.C. Groot (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Marieke A. Mens (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Katinka R. van Kranendonk (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Kilian M. Treurniet (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Manon L. Tolhuisen (Department of Radiology and Nuclear Medicine, Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Heitor Alves (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Annick J. Weterings (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Eleonora L.F. Kirkels (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Eva J.H.F. Voogd (Department of Neurology, Rijnstate Hospital, Arnhem); Lieve M. Schupp (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam); Sabine L. Collette (Department of Neurology, Radiology, University Medical Center Groningen); Adrien E.D. Groot (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Natalie E. LeCouffe (Neurology, Amsterdam UMC, University of Amsterdam, Amsterdam); Praneeta R. Konduri (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Haryadi Prasetya (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Nerea Arrarte-Terreros (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Lucas A. Ramos (Biomedical Engineering & Physics, Amsterdam UMC, University of Amsterdam, Amsterdam); Nikki Boodt (Department of Neurology, Radiology, Public Health, Erasmus MC, University Medical Center); Anne F.A.V Pirson (Department of Neurology, Maastricht University Medical Center and Cardiovascular Research Institute Maastricht (CARIM)); Agnetha A.E. Bruggeman (Department of Radiology and Nuclear Medicine, Amsterdam UMC, University of Amsterdam, Amsterdam).
Contributors SJdH monitored data collection for the whole trial, wrote the statistical analysis plan, cleaned and analyzed the data, and drafted and revised the paper. NB and AAEB collected data and revised the draft paper. BR, ACGMvE, BJE, CBLMM, WHvZ, IRvdW, PJvD, and HFL revised the draft paper. DWJD wrote the statistical analysis plan and drafted and revised the paper.
Funding The MR CLEAN Registry (Multicenter Randomized Clinical Trial of Endovascular Treatment of Acute Ischemic Stroke) was partly funded by Stichting Toegepast Wetenschappelijk Instituut voor Neuromodulatie (TWIN), Erasmus MC, University Medical Center, Maastricht University Medical Center, and Amsterdam University Medical Center.
Competing interests DWJD reports funding from the Dutch Heart Foundation, Brain Foundation Netherlands, The Netherlands Organisation for Health Research and Development, Health Holland Top Sector Life Sciences & Health, and unrestricted grants from Penumbra Inc., Stryker European Operations BV, Medtronic, Thrombolytic Science, LLC, and Cerenovus for research, all paid to his institution. CBLMM reports grants from CVON/Dutch Heart Foundation, European Commission, TWIN Foundation, Dutch Health Evaluation Program, and Stryker, paid to his institution and is a minority shareholder of NICO.LAB. WHvZ received consultation fees from Stryker and Cerenovus, paid to his institution. PJvD received consultation fees from Stryker, paid to his institution.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.