Article Text

Statistics from Altmetric.com
We read with great interest the recently published article in the journal entitled ‘Safety of the Apollo Onyx delivery microcatheter for the embolization of brain arteriovenous malformations: results from a prospective post-market study’. This study yielded overall fantastic technical, angiographic results with low morbidity and mortality rates.1 The primary endpoints for which the trial was powered were clearly defined as follows: unintentional catheter tip detachment with clinical sequelae, catheter rupture/break/fracture with clinical sequelae, or retained catheter body in the vasculature. Secondary endpoints, both acute (30 days) and long term (12 months), are also presented and specified. Patients not experiencing an adverse event and without any catheter retained were considered successfully concluded. The study failed to document any cases of migration of the retained microcatheter tip after embolization. The authors identified that the device-related complications or adverse events were lower in their study than in previously published literature.
The primary purpose of this commentary is to congratulate the authors for the well-conducted study and the results it yielded. However, we would like to use the opportunity to issue alarming attention to the JNIS readership over some worrying real-world and single-centre data regarding the safety of the Apollo microcatheter. Our institution is a perfect case example of a mid-volume cerebrovascular centre. For 8 years (January 2013 to January 2021) over 200 patients underwent endovascular embolization with detachable tip microcatheters and non-adhesive liquid embolic agents (LEAs). Our experience is generally limited to the Apollo Onyx delivery microcatheter or 323 catheters because it remains the only locally available detachable tip microcatheter. With the Apollo microcatheter, we successfully obtained experience with the most commercially available non-adhesive LEAs—Onyx 18, Squid 12, all formulations of PHIL and Menox 18.2 3 We acknowledge that gaining experience with various embolization techniques like pressure cooker and combined LEAs4 via the same delivery catheter and overcoming the learning curve of the notorious transvenous approach were thanks to the feasibility of the Apollo microcatheter. During that period, we experienced and reported in referred journals similar technical and clinical results regarding cerebral arteriovenous malformation (AVM) endovascular embolization.
Up until recently (May 2020) a retained catheter body into the vasculature was encountered only once. In this case, the microcatheter was intentionally dismantled at the puncture site without even attempting to mechanically detach the Apollo. The decision to leave the catheter body in the vasculature was based on the calibre of the feeding artery, the nature of the target nidal component, and the increased chance of traction-related cerebral vascular damage with unpredictable consequences. Long-term follow-up of this patient for almost 5 years after the endovascular embolization failed to document any device related complications—parent vessel occlusion or peripheral and groin long-term vascular damage.
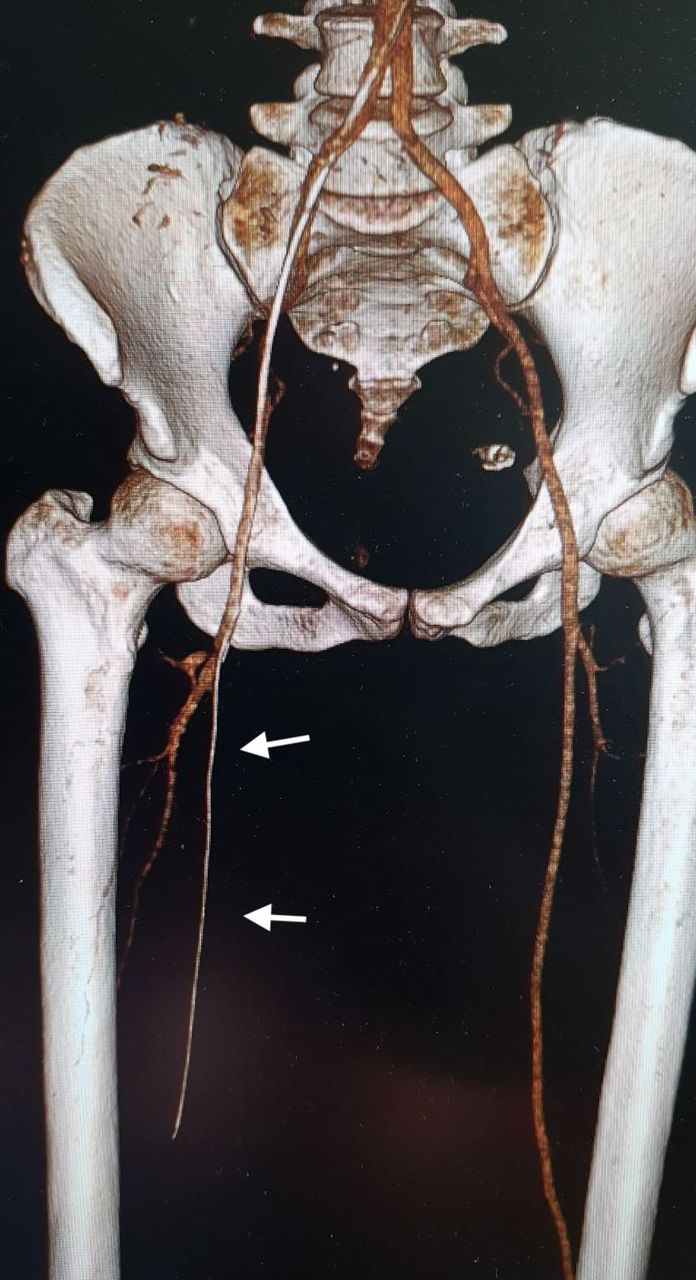
From May 2020 to May 2021, we observed eight consecutive detachment issues with the Apollo microcatheter. In these cases, we failed to successfully detach the tip of the catheter despite extensive pulling and the fact that the detachable portion of the catheter remained ‘untouched’ by the used non-adhesive LEA (online supplemental videos 1,2). All eight catheters had to be left in situ with a cut-off proximally at the femoral puncture site. Given the relative increase in thromboembolic complications from the retained microcatheters, all the patients commenced regular aspirin 100 mg daily. Within 90 days of the embolization, two patients underwent emergent operative removal of the retained Apollos, resulting in limb amputation and stent-graft implantation. The bodies of the two catheters were found embedded within the distal thoracic abdominal aorta and stuck into the proximal posterior tibial artery (figure 1).
Supplementary video
Supplementary video

{kind=link}
Computed tomography (CT) angiography with 3D volume rendering reconstructions of the lower limbs revealing a lengthy foreing body within the femoral/popliteal artery of the right leg.
To avoid any bias, we performed a quantitative investigation of the applied embolic agents during all cases. Vials with Onyx 18 (eV3- Covedien, Irvine, CA) and Menox liquid embolic system (Meril Life Sciences, India Pvt Ltd) were tested for various quality attributes, that is, viscosity measurement, solidification time, material expansion, tantalum suspension, dimethyl sulfoxide (DMSO) radiopacity, and fragmentation tests. All the conducted tests met standard requirements.
We reviewed results from the medical device reports submitted to MAUDE (Manufacturer and User Facility Device Experience) US Food and Drug Administration between May 2015 to May 2021 involving Apollo microcatheter entrapment. Although some of the encounters were not reported in detail, we identified 15 cases of retained microcatheters due to failed catheter retraction. Nine of those cases were reported during the period May 2015 to May 2018.
Similar device faults and catheter technical malfunctions have been reported.5 6 However, this is the backbone of technological progress and the driving force of innovation in our field. Enhanced technical properties and offspring devices were born due to collaboration between scientists, physicians, and regulatory authorities.7 8
Sometimes, this kind of report draws attention before an alarming trend has occurred.9 Most recently, a rallying cry from our community pointed out some dangerous features of a specific distal access catheter, wich led to immense and appropriate action from the manufacturer and the regulatory authorities.10–12 These types of articles have the power to turn the neurovascular armamentarium into something better than it was before.
When it comes to detachable tip microcatheters, technical failures have been observed with Apollo’s major competitor (Sonic, Balt).13
In conclusion, any human activity involves some risk to life or health. Although it is possible to reduce the absolute risk of a particular activity, it is impossible to reach ‘zero risk’ or ‘absolute safety’ that is often demanded. The failure of this microcatheter could potentially lead to severe complications; hence this information should be shared with colleagues by putting ‘safety’ into perspective.
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. Not applicable.
Ethics statements
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Please change contributors:
Conceptualization: AS, SS. Investigation and clinical results assessment: AS, SS, KM. Writing - original draft: AS, SS. Critical review : KM, SS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.