Article Text

Abstract
Background We report outcomes of spontaneous intracranial hypotension (SIH) patients who underwent transvenous embolization of cerebrospinal fluid-venous fistulas (CSFVFs) confirmed on digital subtraction myelography (DSM) performed at our institution.
Methods This is a retrospective evaluation of a prospectively collected database of SIH patients who underwent transvenous embolization of CSFVFs. Only patients who had fistulas confirmed on DSM performed at our institution were included. All patients had a baseline MRI and an MRI performed at least 90 days post-embolization, as well as clinical evaluation using the six item Headache Impact Test (HIT-6) and the Patient Global Impression of Change (PGIC) scales. Paired t-test was used to report changes in Bern MRI scores and HIT-6 scores at follow-up.
Results 40 patients were included (29 female, 11 male). Mean age was 57.4±10.3 years. Mean Bern score improved from 5.7±3.0 at baseline to 1.3±2.0 at follow-up (p<0.0001). Mean HIT-6 score at baseline was 67.2±11.1 and at follow-up was 41.5±10.1 (p<0.0001). Median PGIC was 1, with 36 patients (90.0%) reporting at least minimal improvement and 32 patients (82.5%) reporting much or very much improvement. Complications included persistent local site pain in 12 patients (30%), suspected rebound intracranial hypertension requiring medical intervention in 7 patients (17.5%), and asymptomatic tiny Onyx emboli to the lungs in 3 patients (7.5%).
Conclusions Transvenous embolization of CSFVFs using Onyx is safe and effective, resulting in significant improvement in headache and overall clinical outcomes in nearly 90% of patients, and substantial improvements in brain MRI abnormalities.
- fistula
- intracranial pressure
- liquid embolic material
Data availability statement
No data are available. NA.
Statistics from Altmetric.com
Introduction
Spontaneous intracranial hypotension (SIH) is a debilitating disease resulting from non-iatrogenic spinal cerebrospinal fluid (CSF) leaks.1 2 While the classical presentation is orthostatic headache, there are myriad other debilitating symptoms including vertigo, tinnitus, vision changes, back pain, and cognitive impairment. As most patients are diagnosed between the ages of 30 and 50 years, SIH is particularly devastating from social and economic perspectives.3
CSF-venous fistula (CSFVF) is an increasingly recognized cause of SIH. The exact pathogenesis of these lesions is unclear, with hypotheses that they represent aberrant connections between the nerve root sleeve and paraspinal veins or are secondary to increased CSF drainage via spinal arachnoid granulations that rupture into adjacent radicular veins. With the increased adoption of digital subtraction myelography (DSM) and decubitus CT myelography, we have been diagnosing these lesions with increasing frequency.4–6
Several treatment options have been proposed for CSFVF, including surgical ligation, nerve root skeletonization, and blood/fibrin patching.7 Surgical ligation has been shown to be effective in treating CSFVF by means of disconnecting the venous outflow pathway from the thecal sac. We recently reported the results of the first five patients to undergo a novel transvenous embolization approach to treatment of CSFVF.8 That publication spurred considerable interest in this technique. Now we report a larger series of transvenous embolization of CSFVF, including both patient-reported clinical outcomes and imaging follow-up.
Methods
Patient selection
Following institutional review board approval, we retrospectively reviewed a prospectively collected database of patients with SIH secondary to high probability CSFVF diagnosed on DSM performed at our institution. All patients were evaluated by a neurologist with special expertise in CSF dynamics disorders and underwent comprehensive imaging evaluation including total spine MRI and brain MRI with and without contrast. Following localization of the CSFVF on DSM, patients underwent transvenous embolization of the CSFVF using a previously described technique.9
Digital subtraction myelography technique
Our technique for DSM has been described elsewhere.5 Briefly, all DSMs were performed on an Allur Xper FD 20/20 fluoroscopy unit (Philips Healthcare, Best, The Netherlands) with spinal angiography set to 1 frame per 1–2 s. A tiltable table was used to adjust spine angling, and in most cases a wedge-shaped cushion was used to position the patient’s hips superior to the shoulders. All DSMs were performed with a single plane. In general, a 20 ga spinal needle was used to access the thecal sac at L2/3 or below, then 10 mL of saline was slowly injected. Following this, 5–6 mL of Omnipaque 300 was injected in rapid fashion while the imaging system was centered on the thoracic spine and angiography was performed. Another 5–6 mL of contrast was injected and angiography performed after re-centering the imager on the thoracolumbar region. Most patients were imaged on consecutive days with one side down being performed on day 1 and the other side down performed on day 2. Most patients also had post-DSM CT performed on one or both days.
Patient imaging evaluation
All patients underwent baseline and 3 month follow-up brain MRI with and without intravenous contrast. MRI sequences included pre-contrast sagittal T1, FLAIR (fluid attenuated inversion recovery), T2, and GRE (gradient-recalled echo) and post-contrast T1 weighted imaging. Brain MRIs were analyzed for evidence of SIH according to the methods put forth by Dobrocky et al (Bern score).10 The following imaging findings were analyzed: venous sinus distension, pachymeningeal enhancement, presence of subdural fluid collections, effacement of suprasellar cistern (defined as ≤4.0 mm) or pre-pontine cistern (≤5.0 mm), and reduced mamillopontine distance (≤6.5 mm). Three imaging findings were considered major (2 points each): pachymeningeal enhancement, venous sinus engorgement, and suprasellar cistern effacement. Three were considered minor (1 point each): subdural fluid collection, prepontine cistern effacement, and reduced mamillopontine distance. Patients were then classified as low, intermediate, or high probability of finding a spinal CSF leak based on total Bern score ≤2 points, 3–4 points, or ≥5 points, respectively, on a scale of 9 possible points.
Patient clinical evaluation
All patients underwent comprehensive neurological evaluation before and after endovascular therapy. Patients were queried on positional symptoms, headache, hearing loss, tinnitus, and cognitive disturbance. Patients also routinely completed the six item Headache Impact Test (HIT-6) questionnaire at baseline and 3 month follow-up.11 HIT-6 score severities were divided into 36–49 (little or no impact), 50–55 (some impact), 56–59 (substantial impact), and ≥60 (severe impact). Patient Global Impression of Change scores (PGIC) were also collected. This is a validated 7-point Likert-type scale that assesses a patient’s overall sense of improvement following an intervention.12 13
Endovascular technique
Details of the technique for embolization are provided in the technical video and originally published technical report. For embolization of the fistulas, our approach was to selectively catheterize the paraspinal vein that was identified as draining the fistula on the DSM and then embolize that vein using Onyx. Access was generally obtained in the right common femoral vein. A 6 French (Fr) benchmark catheter was then advanced into either the azygous vein (for thoracic fistulas), ascending lumbar vein (lumbar fistulas), or vertebral vein (cervical fistulas) over a long 5 Fr vertebral catheter. Following guide catheter placement, we advanced either a Headway Duo microcatheter or a Scepter XC microcatheter over a Synchro microguidewire into the paraspinal vein. Once the microcatheter was past the anatomical landmark of the pedicle, a venogram of the paraspinal vein was performed. Next, we proceeded with Onyx embolization using either Onyx 18 or 34 depending on proximity of the microcatheter tip to the radicular vein. If the microcatheter was within 5 mm of the exact site of the CSFVF, Onyx 34 was generally used. If the microcatheter was >5 mm away, then Onyx 18 was used. A follow-up CT was performed immediately for all patients to confirm the level and extent of the Onyx cast.
Statistical analysis
Descriptive statistics are reported as mean±SD for continuous variables and N (%) for categorical variables. To compare continuous outcomes (Bern SIH score and HIT-6 score), we used a paired t-test to determine if there was improvement in imaging findings of SIH. Data were normally distributed.
Results
Patient population
Baseline patient characteristics are summarized in table 1. A total of 50 fistulas were treated in 40 patients (29 female, 11 male). Mean age at treatment was 57.4 years. Mean body mass index at time of presentation was 28.4±5.3 kg/m2. No patients had a genetic or clinically diagnosed connective tissue disorder. Five patients had undergone prior surgery for alternative sites of leakage. At clinical presentation, the most common symptom was headache, almost always with orthostatic and/or Valsalva worsening. Other symptoms were less common (table 1). On DSM, 34 fistulas were on the right thoracic spine, 12 were on the left thoracic spine, and the remainder were in the cervical and lumbar spine. Seven patients had multiple fistulas treated concurrently.
Baseline patient characteristics
Periprocedural results
Thirty-one cases were performed with conscious sedation and nine cases were performed under general endotracheal anesthesia. All awake patients reported some intraoperative pain during Onyx injection, centered around the level of the embolization. On postoperative CT, Onyx was seen to have been successfully delivered into the foraminal vein in 36 patients. In four patients it was only in the paraspinal vein. Regarding intraoperative complications, there were two cases of paraspinal vein perforation, both treated with Onyx embolization with no immediate clinical sequelae. There were three cases in which small amounts of Onyx were seen in tiny fifth order subsegmental pulmonary arteries on postoperative CT, also asymptomatic. In no case did Onyx go into the intrathecal space. All patients were discharged the same day as the procedure.
Post-procedural complications/treatment failures
In total, seven patients had possible rebound intracranial hypertension severe enough to require medical management with acetazolamide. In all patients, they developed severe headaches when in the recumbent position, which improved when upright (opposite of an orthostatic headache), which was refractory to medical therapy with non-steroidal anti-inflammatory drugs or acetaminophen. Only two underwent a lumbar puncture to confirm an elevated opening pressure, and the rest were managed remotely without diagnostic tests confirming the presence of rebound hypertension. All but two patients were able to discontinue acetazolamide within 3 months. Thirty percent of patients reported some local pain at the site of the embolization 3 months after embolization, but no patient required long-term medical therapy and in no case was it debilitating. Three patients had new leaks discovered at different levels on DSMs after embolization. Two patients were retreated, one enjoyed persistent improvement and one continues to suffer from headache and other SIH symptoms. The third is pending re-treatment. Two patients were found to have a persistent CSFVF from the level of the embolization on a follow-up DSM. One was treated successfully and one was treated but continues to experience symptoms and brain sag and is undergoing further evaluation to identify the site of the leak.
Imaging outcomes
All patients had a postoperative MRI performed 1–4 months after embolization (median and mode were 3 months). Mean preoperative Bern score was 5.7±3.0 at baseline and improved to 1.3±2.0 at follow-up (p<0.0001). Six had no change in Bern score (four had a Bern score of 0 at baseline so no improvement was expected). No patients had worsening in the Bern score on follow-up imaging. Examples are provided in figures 1 and 2.

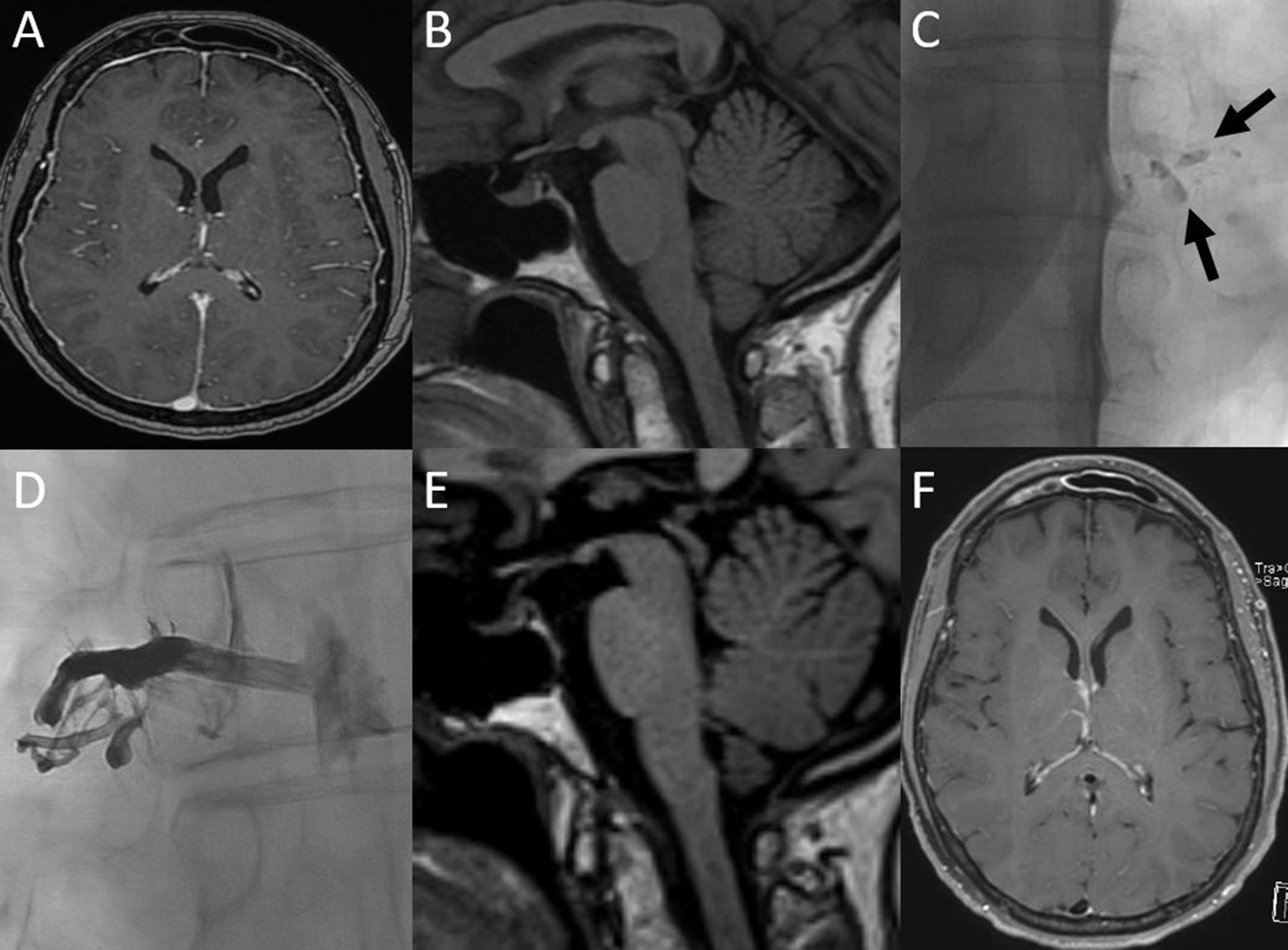
Example of Onyx cast and MRI results of cerebrospinal fluid-venous fistula (CSFVF) embolization in a patient in their 50s, who presented with severe orthostatic headaches and cognitive changes which limited their ability to work. The patient also had tinnitus. (A) Sagittal T1 MRI showing signs of brain sag with decreased mamillopontine distance, effacement of suprasellar cistern, cerebellar tonsillar ectopia, and effacement of the prepontine cistern. (B) Axial T1 post-contrast MRI showing smooth dural enhancement. (C) Digital subtraction myelogram showing a CSFVF at right T9 (arrow). (D) Post-embolization X-ray showing Onyx cast at right T9. (E) Post-treatment axial T1 post-contrast MRI showing resolution of pachymeningeal enhancement. (F) Post-treatment sagittal T1 MRI showing resolution of brain sag. The patient’s symptoms resolved.
{kind=link}
{kind=link}
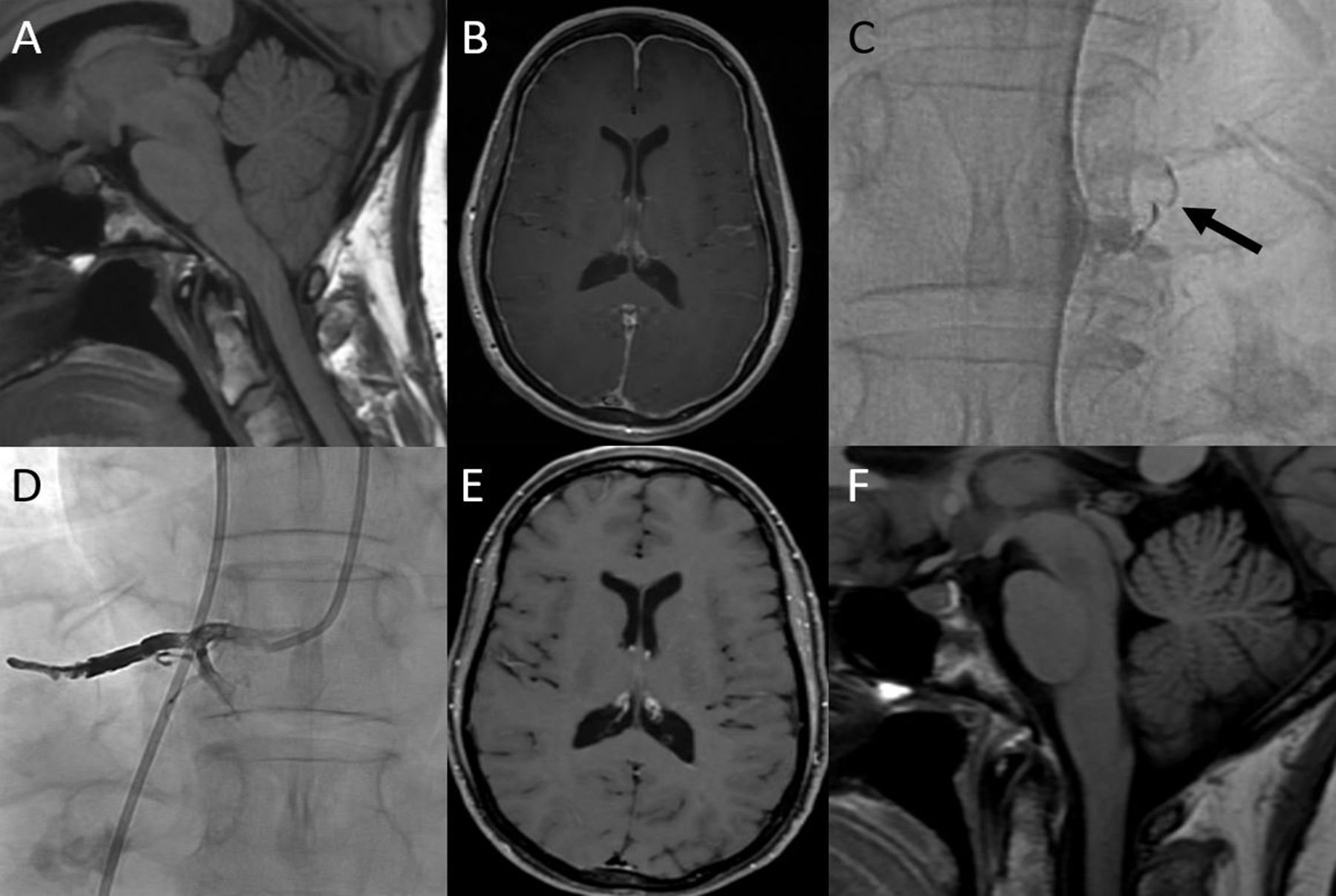
Example of cerebrospinal fluid (CSF) hypotension presenting with mainly pachymeningeal enhancement in a patient in their 40s, who presented with severe orthostatic headaches and cognitive changes which limited their ability to work. (A) Axial T1 post-contrast MRI showing smooth dural enhancement. (B) Sagittal T1 MRI showing signs of brain sag with minimally decreased mamillopontine distance and some tonsillar ectopia, but the degree of severity is very mild. (C) Digital subtraction myelogram showing a CSF-venous fistula at right T8 (arrows). (D) Post-embolization X-ray showing Onyx cast at right T8. (E) Post-treatment sagittal T1 MRI showing improvement in the mamillopontine distance. Note how the pituitary is more flat now than on the previous MRI and the degree of tonsillar ectopia is improved. (F) Post-treatment axial T1 post-contrast MRI showing resolution of pachymeningeal enhancement. The patient had persistent headaches post-embolization which were thought to be related to rebound hypertension and has been treated with acetazolamide. After 6 weeks of acetazolamide treatment all headaches resolved and the patient has been headache-free for 6 months.
Clinical outcomes
Mean HIT-6 score at baseline was 67.2±11.1 and at follow-up was 41.5±10.1 (p<0.0001). Median PGIC was 1, with 36 patients (90.0%) reporting at least minimal improvement, and 33 patients (82.5%) reporting much or very much improvement. Thirty-five patients had improvement by at least one degree on the HIT-6 scale at 3 months, while four patients had stable scores and one patient had clinical worsening. Two of the patients with unchanged HIT-6 scores did not have headaches at baseline.
Discussion
Our series of 40 patients with SIH who underwent transvenous embolization of one or more CSFVF has several important findings. First, the treatment was highly effective with 90% of patients achieving substantial improvement in their symptoms, of which headache was the most common. Second, more than 90% of patients had improvement of brain MRI findings as assessed by the Bern score, and this was in concordance with the improvement in clinical symptoms. Third, the treatment was safe, with all patients being treated in the outpatient setting and no major hemorrhagic or spinal ischemic complications occurring. Common clinical complications included suspected rebound intracranial hypertension in 17.5% of patients, and modest pain at the level of the embolization not requiring prolonged medical therapy in 30% of patients. Overall, these findings suggest that transvenous embolization should be considered for patients with CSFVF.
Several treatment options are currently available for CSFVF. Spinal surgery has been the mainstay of treatment essentially since CSFVF was initially described in 2014. Surgical intervention typically includes laminectomy, facetectomy, and ligation of the nerve root and associated veins. By completely disconnecting the fistula, including both the CSF-filled nerve root sleeve and the draining veins, surgical intervention can result in immediate and complete obliteration of CSFVF. A recent series of 42 patients from our institution who underwent surgical ligation of CSFVF found that 49% were headache-free and another 27% had at least 50% improvement at 5 months. Furthermore, approximately 80% had improvement or resolution of MRI findings of CSF hypotension.7
Other minimally invasive treatment options such as epidural blood patch and fibrin glue injection have been reported as potential treatment options for CSFVF and are thought to work by compressing the fistula. These are effective in only a minority of patients.14 In fact, one recently published systematic review and meta-analysis including individual patient data has recently shown that in general, epidural blood patch and/or fibrin glue provides little to no relief, with <15% of patients getting any permanent relief and only 45% of patients getting temporary relief. Another limitation of fibrin glue and epidural blood patch is that in general, multiple treatments are required (mean 2.5 treatments), and despite this, a vast majority of patients still must undergo surgery.15
As demonstrated in this report, occlusion of the draining veins with a liquid embolic agent such as Onyx leads to a reduction in shunting sufficient to result in symptomatic and radiographic cure. This effect could be due to direct occlusion of the fistula by the liquid embolic agent or by creating local venous hypertension that reverses the favorable pressure gradient for CSF to leak into the vein.16 Given that the anatomy of venous drainage of the nerve root sleeve has a plexus-like organization, we have opted to use Onyx to embolize these fistulas as the Onyx can permeate into tinier veins and venules, especially in its more dilute formulation (Onyx 18). We build a plug with Onyx 34 because this keeps the Onyx 18 from refluxing into the azygous vein and then into the lungs.
Not all treated patients experienced excellent outcomes. We suspect there may be a few reasons for this. First, we had at least one patient who developed a new leak that was not previously detected on DSM following the embolization procedure. We suspect that some patients may be prone to development of additional spinal CSF leaks due to underlying disorders of connective tissue matrix or other reasons. It may also be that a mild degree of intracranial hypertension following closure of a CSFVF precipitates the development of additional CSFVF. In some patients, the intracranial hypertension following treatment could be a manifestation of underlying idiopathic intracranial hypertension and not ‘rebound hypertension’ but rather a return to the pre-fistula state of elevated pressures. Objective data are scarce, but there have been anecdotal reports of headaches due to intracranial hypertension in patients with Ehlers-Danlos syndrome, and this and other connective tissue diseases are supposed risk factors for spinal CSF leaks and CSFVF. Alternatively, rebound intracranial hypertension could develop as a result of compensation from a chronic state of CSF depletion in patients whose CSF pressure was normal before the development of CSFVF.17 18 Clinically meaningful suspected rebound intracranial hypertension requiring medical therapy occurred in approximately 15% of patients in our series. In some patients this was so severe that it temporarily overshadowed the benefits of closure of the CSFVF. Technical failure could preclude excellent clinical outcomes in some patients. Since the spinal venous plexus is richly anastomosed, we believe that failure to deliver Onyx into the foraminal vein could result in persistent CSFVF even if the paraspinal vein is closed. This was demonstrated in one patient in our series. Lastly, we know that DSM is not 100% sensitive or specific in the diagnosis of CSFVF. In some cases, a patient may have had multiple CSFVFs, including some which were occult on DSM, and closure of one may not have been sufficient. We suspect this to be the case in most treatment failures given that, even with surgical ligation, treatment efficacy is in the order of 75–80%.
Limitations
Our case series has limitations. First, the follow-up duration ranges from 2–4 months in these patients. The long-term effects of this treatment have yet to be elucidated. Given that Onyx is a permanent embolic agent, and that these fistulas are slow flow shunts with very small pressure gradients, we have no reason to believe that fistulas would recanalize. We suspect that it is more likely that patients would develop additional fistulas at other levels, which could later be embolized. Second, because patients are referred to us from multiple centers, we do not have uniform pre-treatment MRI protocols, with some scans performed at 1.5 T.
Conclusion
We report a large case series of transvenous paraspinal vein embolization of CSFVFs. This novel treatment approach resulted in clinical and radiographic improvement in 90% of patients with no permanent complications. Further studies are needed to confirm our technique and to study the durability of this treatment effect.
Supplemental material
Data availability statement
No data are available. NA.
Ethics statements
Patient consent for publication
Ethics approval
This study was approved as a retrospective study analyzing outcomes of patients undergoing treatment of CSF leaks. Mayo Clinic IRB 19-002405.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors WB made substantial contributions to the conception and design of the work, acquisition, analysis and interpretation of data as well as drafted the work and gave final approval of the published version and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. JC-G, LS, JLDA, IG, NK and MW made substantial contributions to the acquisition, analysis and interpretation of data AND revised it critically for important intellectual content and gave final approval of the published version and agrees to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. WB is responsible for the overall content and is the guarantor of the entire work. He accepts full responsibility for the work and conduct of the study, had access to the data and controlled the decision to publish.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests WB consultant for Medtronic, Microvention, Stryker, Cerenovus, MIVI. No other financial relationships.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.