Article Text

Abstract
Background The benefit of complete reperfusion (modified Thrombolysis in Cerebral Infarction (mTICI) 3) over near-complete reperfusion (≥90%, mTICI 2c) remains unclear. The goal of this study is to compare clinical outcomes between mechanical thrombectomy (MT)-treated stroke patients with mTICI 2c versus 3.
Methods This is a retrospective study from the Stroke Thrombectomy and Aneurysm Registry (STAR) comprising 33 centers. Adults with anterior circulation arterial vessel occlusion who underwent MT yielding mTICI 2c or mTICI 3 reperfusion were included. Patients were categorized based on reperfusion grade achieved. Primary outcome was modified Rankin Scale (mRS) 0–2 at 90 days. Secondary outcomes were mRS scores at discharge and 90 days, National Institutes of Health Stroke Scale score at discharge, procedure-related complications, and symptomatic intracerebral hemorrhage.
Results The unmatched mTICI 2c and mTICI 3 cohorts comprised 519 and 1923 patients, respectively. There was no difference in primary (42.4% vs 45.1%; p=0.264) or secondary outcomes between the unmatched cohorts. Reperfusion status (mTICI 2c vs 3) was also not predictive of the primary outcome in non-imputed and imputed multivariable models. The matched cohorts each comprised 191 patients. Primary (39.8% vs 47.6%; p=0.122) and secondary outcomes were also similar between the matched cohorts, except the 90-day mRS which was lower in the matched mTICI 3 cohort (p=0.049). There were increased odds of the primary outcome with mTICI 3 in patients with baseline mRS ≥2 (36% vs 7.7%; p=0.011; pinteraction=0.014) and a history of stroke (42.3% vs 15.4%; p=0.027; pinteraction=0.041).
Conclusions Complete and near-complete reperfusion after MT appear to confer comparable outcomes in patients with acute stroke.
- stroke
- thrombectomy
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the principal investigator upon reasonable request.
Statistics from Altmetric.com
Introduction
Timely reperfusion of the penumbra is the cornerstone of acute ischemic stroke (AIS) treatment. Due to its strong correlation with clinical outcome, recanalization has been deemed an important biomarker of therapeutic activity in AIS clinical trials.1 Advances in endovascular mechanical thrombectomy (MT) devices and associated higher recanalization rates led to concomitant improvements in patient outcomes.2–5 The American Heart Association guidelines define successful reperfusion as a modified Thrombolysis in Cerebral Infarction (mTICI) score of 2b or higher, but improved functional outcome has been reported beyond the 50% reperfusion threshold.6–9
The mTICI 2c grade (90–99% reperfusion) was added to differentiate outcomes of patients with near-complete reperfusion from those with closer to 50% reperfusion.10 11 There is mounting evidence that suggests patients with mTICI grade 2c or 3 reperfusions have better outcomes than those with an mTICI 2b result.6 9 12–15 However, the clinical distinction between mTICI 2c and 3 is unclear. Should neurointerventionalists seek to achieve picture-perfect angiographic reperfusion at the cost of longer procedural times, more passes, and potentially higher complication rates? The aim of this multicenter retrospective cohort study was to compare outcomes between mTICI 2c versus 3 reperfusions in MT-treated patients with AIS outside the clinical trials setting.
Methods
Patient population
This is a retrospective study derived from the Stroke Thrombectomy and Aneurysm Registry (STAR) comprising data from 33 stroke centers. Individual patient data were de-identified and independently verified by each contributing center. The data were then pooled and analyzed by the Medical University of South Carolina. The study was approved by the institutional review board (IRB) of each participating center, and the requirement for written consent was waived. The study period was between 2013 and 2020. This study follows the guidelines set out by the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement.
Adult patients (age ≥18 years) were included in the study if they presented with AIS due to anterior circulation arterial occlusion and underwent MT with resultant mTICI 2c or 3 reperfusion. Patients without a recorded 90-day modified Rankin Scale (mRS) score were excluded from the analysis. Patient selection for MT and post-procedural stroke care was performed according to the protocols of the participating centers. Modern MT devices, comprising stent retrievers and aspiration catheters, were used in all procedures. The patients were categorized into two cohorts, mTICI 2c or mTICI 3, based on the reperfusion grade achieved at the end of the procedure.
Patient and treatment parameters
Pre-procedural variables included patient demographics, baseline characteristics, and presentation findings. Patient demographics comprised age, sex, and race. Baseline characteristics comprised medical comorbidities (diabetes mellitus, hypertension, atrial fibrillation, prior stroke, and hyperlipidemia) and pre-stroke mRS score. Presentation findings comprised admission National Institute of Health Stroke Scale (NIHSS), primary vessel occlusion location, and the Alberta Stroke Program Early CT Score (ASPECTS). CT and CT angiography with or without perfusion data were interpreted independently by neuroradiologists, neurologists, and neurointerventionalists at each participating center.
Procedural variables included symptom onset to puncture time, intravenous tissue plasminogen activator (IV-tPA) administration, primary MT technique used (stent retriever, contact aspiration, or combination), intra-arterial tissue plasminogen activator (IA-tPA) administration, use of balloon guide catheter, number of MT attempts, and total procedure time. The reperfusion grade was assessed by the treating neurointerventionalist based on comparison of the initial (pre-MT) versus final (post-MT) catheter digital subtraction angiography (DSA). The revised mTICI grading system was used, such that mTICI 2c was defined as near-complete (90–99%) reperfusion except for slow flow in a few distal cortical vessels or presence of small distal cortical emboli, and mTICI 3 was defined as complete reperfusion of all branches.10 11
Outcome parameters
The primary outcome was mRS 0–2 (functional independence) at 90 days (±14). Secondary outcomes included good outcome (mRS 0–2) at hospital discharge, excellent outcome (mRS 0–1) at hospital discharge and 90 days, mRS at hospital discharge and 90 days, NIHSS at discharge, symptomatic intracerebral hemorrhage (ICH), and procedure-related complications (eg, access site hematoma, vessel perforation).
Statistical analysis
Statistical analyses were performed using the IBM SPSS Statistics software, version 25. Baseline characteristics between the unmatched mTICI 2c and 3 cohorts were compared using Pearson’s χ2 test for categorical variables and Student’s t-test or Mann–Whitney U test for continuous variables, as appropriate. Associations between mTICI grade and outcomes were assessed using logistic, ordinal, and linear regression models, as appropriate, and corresponding ORs, β values, and 95% CIs were reported. Predictors of good outcome were assessed in a multivariable logistic regression model comprising mTICI grade, adjusted for baseline characteristics. The independent variables were tested for multicollinearity using tolerance and variance inflation factor. The overall fit of the model was assessed using the Hosmer–Lemeshow goodness-of-fit test. To address potential bias associated with missing data, multiple imputation by chained equations with m=10 was performed. Imputed values for sex (0.04%), age (0.04%), race (18%), diabetes mellitus (8.6%), hypertension (6.8%), atrial fibrillation (7%), hyperlipidemia (6.9%), prior stroke (23%), pre-stroke mRS (30%), admission NIHSS (1%), ASPECTS (34.5%), IV-tPA administration (6%), and symptom onset to puncture time (21%) were generated using conditional regression models with the auxiliary variable of mRS at 90 days. Parameter estimates from analyzing the imputed datasets were pooled according to Rubin’s rules.16
The mTICI 2c and 3 cohorts were then matched using case–control matching in a 1:1 ratio for variables demonstrating between-cohort differences with p<0.100 in univariate analysis or a standardized difference of ≥0.20. A standardized difference of <0.20 between the matched cohorts in baseline characteristics was considered adequate balance. Associations between mTICI grade and outcomes in the matched cohorts were assessed using logistic, ordinal, and linear regression models, as appropriate, and corresponding ORs, β values, and 95% CIs were reported. Exploratory subgroup analyses of the matched cohorts were calculated for the primary outcome using unadjusted logistic regression models and models adjusting for age, sex, atrial fibrillation, ASPECTS, NIHSS, primary vessel occlusion location, symptom onset to puncture time, number of attempts, IV-tPA administration, pre-stroke mRS, and primary MT technique without the subgroup-defining variable within categorized analyses. Interactions of exploratory subgroup analyses were tested using the subgroup-defining variable (variable × mTICI grade) with mTICI 2c as reference, adjusting for the variables above. Statistical significance was defined as p<0.05 and all tests were two-tailed.
Results
Characteristics and outcomes of unmatched mTICI 2c versus mTICI 3 cohorts
From a total of 6233 patients in STAR, 2442 patients were eligible for the final analyses including 519 and 1923 patients in the unmatched mTICI 2c and 3 cohorts, respectively; the baseline characteristics of the two cohorts are shown in online supplemental table I. Atrial fibrillation (p=0.004) and prior stroke (p=0.018) were less common in the mTICI 3 cohort. The MT techniques used were different between the two cohorts (p<0.001). Balloon guide catheters (p<0.001) were more commonly used and mean total procedure time (p=0.026) was longer in the mTICI 3 cohort.
Supplemental material
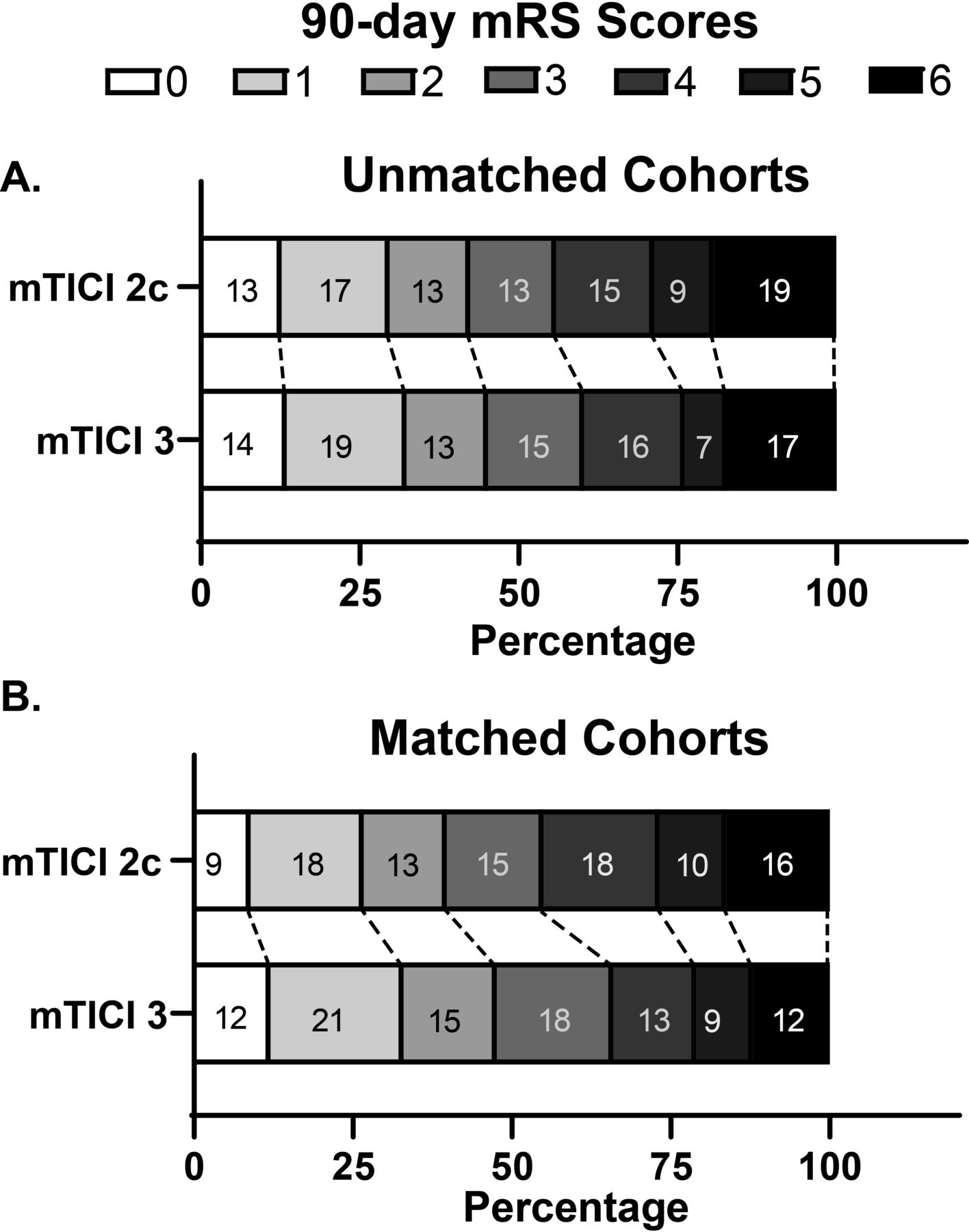
Table 1 compares the primary and secondary outcomes between the unmatched mTICI 2c and 3 cohorts. The two unmatched cohorts had similar rates of the primary outcome (42.4% vs 45.1%; OR 1.118, 95% CI 0.919 to 1.360, p=0.264; figure 1A). Secondary outcomes including functional and neurological outcomes at discharge and 90 days, ICH, and procedure-related complications were also comparable between the two unmatched cohorts.

(A) 90-day mRS distributions of unmatched mTICI 2c versus 3 cohorts. (B) 90-day mRS distributions of matched mTICI 2c versus 3 cohorts. mTICI, modified Thrombolysis in Cerebral Ischemia; mRS, modified Rankin Scale.
Comparisons of outcomes between unmatched mTICI 2c and mTICI 3 cohorts
Predictors of the primary outcome
Online supplemental table II describes the non-imputed and imputed multivariable models predicting the primary outcome of mRS 0–2 at 90 days. Older age (p<0.001), diabetes mellitus (p=0.001), higher pre-stroke mRS (p<0.001), higher admission NIHSS (p<0.001), longer symptom onset to puncture time (p=0.017), use of combined (aspiration and stent retriever) MT technique (p=0.029), higher number of attempts (p=0.030), and procedure-related complications (p=0.009) were negative independent predictors of the primary outcome in the non-imputed model. White race (p=0.001), hyperlipidemia (p=0.045), and higher ASPECTS (p<0.001) were independent predictors of the primary outcome in the same model.
After adjusting for missing data in the imputed model, older age (p<0.001), diabetes mellitus (p=0.027), higher pre-stroke mRS (p<0.001), and higher admission NIHSS (p<0.001) remained negative independent predictors while white race (p=0.019) and higher ASPECTS (p<0.001) remained positive independent predictors of the primary outcome in the imputed model. Reperfusion status (mTICI 2c vs 3) was not predictive of the primary outcome in either the non-imputed (aOR 1.021, 95% CI 0.736 to 1.425, p=0.902) or imputed (aOR 0.898, 95% CI 0.576 to 1.401, p=0.636) multivariable models.
Characteristics and outcomes of the matched mTICI 2c versus mTICI 3 cohorts
Online supplemental table III compares the baseline characteristics between the matched mTICI 2c and 3 cohorts, which each comprised 191 patients. The baseline characteristics were well balanced between the matched cohorts. Table 2 compares the primary and secondary outcomes between the matched mTICI 2c and 3 cohorts. Although mTICI 3 reperfusion resulted in an absolute increase in the proportion of patients with the primary outcome of 7.8%, this difference was not significant (39.8% vs 47.6%; OR 1.377, 95% CI 0.918 to 2.066, p=0.122; figure 1B). mRS at 90 days was lower in the matched mTICI 3 cohort based on shift analysis (median 3 vs 3; OR 0.702, 95% CI 0.493 to 0.999, p=0.049). The remainder of the secondary outcomes were comparable between the two matched cohorts.
Comparisons of outcomes between matched mTICI 2c and mTICI 3 cohorts
Subgroup analyses for the primary outcome
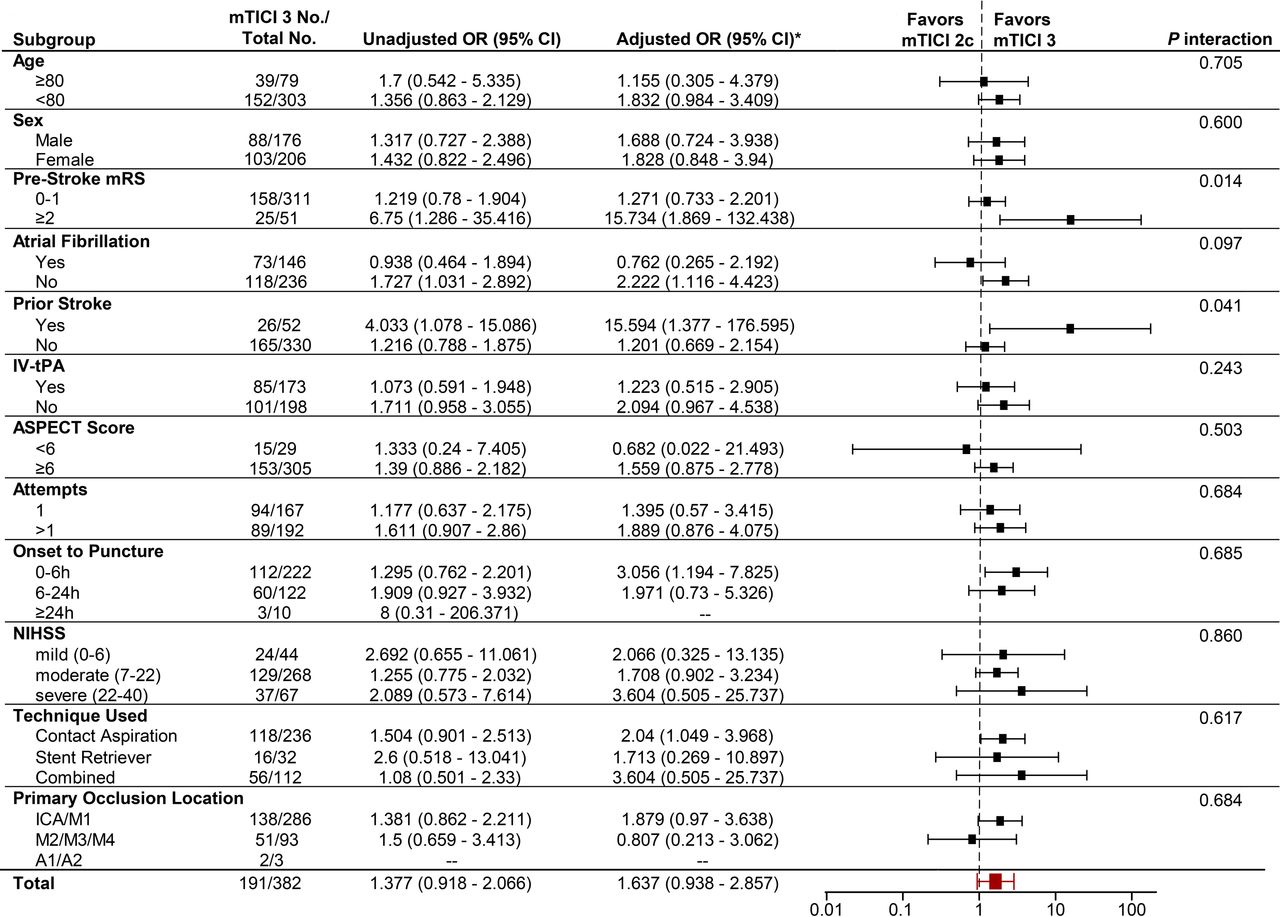
Exploratory subgroup analyses showed increased odds of the primary outcome in patients with pre-stroke mRS ≥2 who achieved mTICI 3 versus 2c reperfusion (n=9/25, 36% vs n=2/26, 7.7%; aOR 15.734, 95% CI 1.869 to 132.438, p=0.011; pinteraction=0.014; figure 2). There was also a greater likelihood of the primary outcome in patients with a history of stroke who achieved mTICI 3 versus 2c reperfusion (n=11/26, 42.3% vs n=4/26, 15.4%; aOR 15.594, 95% CI 1.377 to 176.595, p=0.027; pinteraction=0.041). Increased odds of the primary outcome were observed for patients who achieved mTICI 3 versus 2c reperfusion in subgroups of no atrial fibrillation (n=69/118, 58.5% vs n=53/118, 44.9%; aOR 2.222, 95% CI 1.116 to 4.423, p=0.023), symptom onset to puncture time of 0–6 hours (n=54/112, 48.2% vs n=46/110, 41.8%; aOR 3.056, 95% CI 1.194 to 7.825, p=0.020), and contact aspiration technique use (n=64/118, 54.2% vs n=52/118, 44.1%; aOR 2.040, 95% CI 1.049 to 3.968, p=0.036), but the interactions between reperfusion status and each subgroup category were not significant.
{kind=link}
{kind=link}
Subgroup analyses of primary outcome according to reperfusion status of the matched mTICI 2c vs 3 cohorts. IV-tPA, intravenous tissue plasminogen activator; mRS, modified Rankin Scale; ASPECT, Alberta Stroke Program Early CT; ICA, internal carotid artery; mTICI, modified Thrombolysis in Cerebral Ischemia; NIHSS, National Institute of Health Stroke Scale; SR, stent retriever. *Adjusted for age, sex, atrial fibrillation, ASPECT score, NIHSS score, primary vessel occlusion location, symptom onset to puncture time, number of attempts, IV tissue plasminogen activator administration, pre-stroke mRS, and primary mechanical thrombectomy technique.
Discussion
Modern MT devices have improved both the frequency and extent of successful reperfusion in patients with AIS.4 5 10 However, the infarct core and distal emboli prevent complete reperfusion (ie, mTICI 3) in many cases, especially when the post-MT DSA is adjudicated by an experienced imaging core laboratoy.10 As the mTICI grading scale used in the pivotal MT trials did not distinguish between 50% and near-complete reperfusion, American Heart Association guidelines continue to define successful reperfusion as mTICI ≥2b (≥50% revascularization).2 3 7 Consequently, patients with small distal emboli and near-complete reperfusion have traditionally been categorized as mTICI 2b based on the original grading scale. However, the clinical course of patients with near-complete reperfusion likely resembled patients with complete reperfusion more closely than those with 50% reperfusion. To address the lack of granularity in the original mTICI grading scale, Noser et al proposed a revision that included a 2c grade, which was defined as 'near complete perfusion without clearly visible thrombus but with delay in contrast run-off'.11 Contemporary MT studies, including the present one, use the more recent definition of mTICI 2c proposed by Goyal et al of 'near-complete perfusion except for slow flow in a few distal cortical vessels or presence of small distal cortical emboli'.10
Subsequent studies have corroborated the applicability of the revised mTICI grading scale. In a recent analysis of the MR CLEAN registry comprising 2807 patients, LeCouffe et al observed a positive correlation between the revised mTICI reperfusion grade and functional outcome at 90 days.6 Although patients with mTICI 2c reperfusion had higher odds of better functional outcome compared with those with mTICI 2b reperfusion, this difference was not statistically significant. In the same study, patients with mTICI 2c had significantly better functional outcomes than those with mTICI 2b in the sensitivity analysis that excluded those with mTICI ≥2b reperfusion on initial DSA (ie, patients assigned mTICI ≥2b grade on initial DSA demonstrating resolution of target occlusion before MT). In a retrospective study of 129 patients with internal carotid artery or middle cerebral artery (MCA) M1 segment occlusions who underwent MT, Tung et al observed a greater improvement in discharge NIHSS and lower mean 90-day mRS in patients with mTICI 2c compared with those with 2b reperfusions.17 In a study of 152 MT-treated anterior circulation large vessel occlusions, Naragum et al similarly reported lower 90-day mRS and higher rates of good outcome (mRS 0–2 at 90 days) in patients with mTICI 2c or combined mTICI 2c/3 reperfusions compared with those with mTICI 2b.13 Good neurological outcome (NIHSS <5) at discharge, substantial neurological improvement (NIHSS ≤1 or NIHSS reduction ≥8 between admission and discharge) and functional independence (mRS ≤2) at discharge were also more frequent in patients with MCA occlusions with mTICI 2c versus 2b reperfusions.14 An mTICI grade cut-off of <2c has been shown to be a stronger predictor of poor outcome (mRS >2 at 3 months) than a cut-off of <2 b.15 Liebeskind et al further categorized the mTICI 2b grade into 2b50 (50–66% reperfusion) and 2b67 (67–89% reperfusion).8 Although the mRS distributions differed between mTICI 2b50 and 2b67 reperfusions in their multivariable model, mRS distributions between mTICI 2b67 versus 2c and 2c versus 3 reperfusions were similar. As evidence points towards comparable outcomes between near-complete and complete reperfusions, investigators have proposed the combined mTICI 2c/3 grade as the new angiographic goal for MT in AIS.6 10 13–15 17 However, direct outcome comparisons between mTICI 2c versus mTICI 3 reperfusions are limited in the literature, and small sample sizes and differences in baseline characteristics have precluded rigorous analyses. Furthermore, it is unclear whether specific AIS subgroups may benefit from complete versus near-complete reperfusion.
In this multicenter retrospective cohort study of the prospectively maintained STAR database, we directly compared the outcomes of MT-treated patients with AIS with mTICI 2c versus 3 reperfusions. In doing so, this study represents the first ever matched analysis of mTICI 2c versus 3 post-MT outcomes. We also explored potential interactions between reperfusion status (mTICI 2c vs 3) and multiple subgroups. The primary and secondary outcomes of the unmatched mTICI 2c versus 3 cohorts were similar, although baseline differences in atrial fibrillation, prior stroke, MT techniques used, use of balloon guide catheter, and total procedure time were present. Reperfusion status was not associated with the primary outcome in either the non-imputed or imputed multivariable models comprising all baseline variables. Due to potential confounding effects of differences in baseline characteristics, the two cohorts were matched to control for these differences. However, in the matched cohorts, the primary outcome rate remained similar between the matched mTICI 2c and 3 cohorts. Although the primary outcome rate was 7.8% higher in the matched mTICI 3 cohort, the clinical significance of this difference is unknown.
Secondary outcomes were also comparable between the matched cohorts, except the shift analysis for 90-day mRS favored mTICI 3 reperfusion (p=0.049). There were significant interactions between reperfusion status and each of pre-stroke mRS and prior stroke, such that mTICI 3 reperfusion was associated with a higher rate of the primary outcome in both subgroups. As such, pursuit of more aggressive revascularization may be warranted in patients with a history of stroke or pre-stroke disability. Taken together, near-complete and complete reperfusion after MT for AIS in the real-world setting seem to provide comparable outcomes.
The limitations of this study should be recognized. The results were susceptible to reporting bias as they relied on the accuracy and reliability of data contributed by each center. Selection criteria for MT were determined at the discretion of each contributing center, which could have introduced heterogeneity and selection bias in our study cohort. Despite our best efforts to balance baseline differences and mitigate biases between the patients with mTICI 2c and mTICI 3 using case–control matching, there may be unmeasured variables that were unaccounted for. Procedural characteristics that can influence the degree of reperfusion, including difficulties in navigating to the occlusion site and extent of clot burden, may not have been fully captured in our data. The decision to pursue revascularization of occluded distal branches could not be determined, as the MT stopping point for each center and neurointerventionalist is subject to variation. As we did not have a centralized core laboratory, all imaging data (including mTICI grades) were self-reported by the treating neurointerventionalist, resulting in the lack of independent and systematic adjudication of angiographic results. This represents a major limitation of the study, which may overestimate the proportion of mTICI 3 and 2c results.18 In addition, the revised mTICI grading scale that includes 2c was not universally adopted by all centers, so some mTICI 2c outcomes may have been categorized as grade 3. Consequently, these may have diluted a potential outcome difference between the mTICI 2c and 3 cohorts, thereby effectively increasing the type II error rate.
When determining the threshold of successful reperfusion and procedural stopping point, operator adjudication of the post-MT DSA could be more pertinent in the real-world setting, as the decision to pursue further recanalization is made intraoperatively by the treating neurointerventionalist rather than an imaging core laboratory. We were unable to correlate clinical and radiographic findings at follow-up as final infarct volumes were not captured by the database. Furthermore, follow-up mRS scores were assigned by the treatment team of each respective center, who may not be blinded to the clinical and imaging findings, potentially contributing to detection bias. Conclusions inferred from the findings of the secondary outcomes and exploratory subgroup analyses should be interpreted with caution, as the uncorrected multiple comparisons performed within the study could elevate the false discovery rate. Finally, our findings may not be generalizable to patients with anterior cerebral artery occlusions and those who underwent MT ≥24 hours from symptom onset, as these cases comprised only small minorities of the overall study cohort.
Conclusions
In patients with anterior circulation AIS who underwent MT, complete and near-complete reperfusion appear to confer comparable outcomes. MT-treated patients with pre-stroke disability and those with a history of stroke may have better functional outcomes after complete reperfusion. As endovascular stroke techniques and technologies continue to evolve, future studies could consider mTICI 2c as a benchmark of success.
Data availability statement
Data are available upon reasonable request. The data that support the findings of this study are available from the principal investigator upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @ChalhoubReda, @PascalJabbourMD, @AdamArthurMD, @brainvesseldoc, @DrMichaelLevitt, @WaldoGuerrero82, @Starke_neurosurgery
Collaborators on behalf of the STAR collaborators Dileep R Yavagal, Eric C Peterson, Daniel Raper, Patrick A Brown, M Reid Gooch, Nabeel Herial, Ajith Thomas, Justin Moore, Felipe Albuquerque, Louis J Kim, Melanie Walker, Michael Chen, Stephan Munich, Daniel Alan Hoit, Violiza Inoa-Acosta, Christopher Nickele Lucas, Elijovich Fernanda, Rodriguez-Erazú, Jan Liman, Michael Cawley, Gustavo Pradilla, Brian Howard, Brian Walcott, Zeguang Ren, Ryan Hebert, João Reis, Jaime Pamplona, Rui Carvalho, Mariana Baptista, Ana Nunes, Russell Cerejo, Ashis Tayal, Parita Bhuva, Paul Hansen, Norman Ajiboye, Alex Brehm, Sami Al Kasab, Jonathan Lena, Kimberly Kicielinski.
Contributors Design and conception: C-JC, MSP. Data collection: All authors. Statistical analysis: RC, C-JC. Interpretation of results: All authors. Drafting of manuscript: All authors. Revision of manuscript: All Authors. Approval of final manuscript: All authors. Study supervision: MSP, AMS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests MRL: Grants from the NIH (R01NS105692, R01NS088072, U24NS100654, UL1TR002319, R25NS079200) and the American Heart Association (18CDA34110295). Unrestricted educational grants from Medtronic, Stryker and Philips Volcano. Consultant for Medtronic. Minor equity/ownership interest in Proprio, Cerebrotech, Synchron. Adviser to Metis Innovative. JAG: Grants from the Georgia Research Alliance. Consultant for Cognition Medical. AJY: Grants from Medtronic, Cerenovus, Penumbra, and Stryker. Consultant for Penumbra and Cerenovus. Equity interest in Insera Therapeutics. RWC: Proctor for Medtronic and Cerenovus. AMS: Research support from Penumbra, Stryker, Medtronic, and Siemens. Consultant for Penumbra, Stryker, Terumo, and Arsenal. MM: Consultant for Medtronic and Cerenovus. Stock ownership in Serenity Medical, Synchron, and Endostream. RMS: Grants from the NREF, Joe Niekro Foundation, Brain Aneurysm Foundation, Bee Foundation, the NIH (R01NS111119-01A1, UL1TR002736, KL2TR002737), the National Center for Advancing Translational Sciences, the National Institute on Minority Health and Health Disparities, and Medtronic. Consultant for Penumbra, Abbott, Medtronic, InNeuroCo and Cerenovus. Others: None.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.