Article Text

Abstract
A 14-year-old boy with Loeys–Dietz syndrome (LDS) had an acute neurologic decline 6 days after a subarachnoid hemorrhage. Cerebral angiography at presentation did not show an aneurysmal source of the hemorrhage. However, on post-bleed day 6 the patient experienced an acutely worsening headache and subsequently lost consciousness. Head CT showed new subarachnoid blood and repeat angiography demonstrated a basilar tip aneurysm. Endovascular coil embolization was performed and his neurologic status improved postoperatively until post-bleed day 9 when he became unresponsive. A CT angiogram demonstrated severe proximal vasospasm. After an unsuccessful attempt to treat the vasospasm medically, the patient was transported to the neurointerventional suite for intra-arterial vasodilator treatment, which also failed to ameliorate the vasospasm. The endovascular surgeons were then faced with the conundrum of attempting a high-risk cerebral angioplasty in a pediatric patient with LDS or returning to maximal medical treatment for severe refractory vasospasm.
- Aneurysm
- Angiography
- Angioplasty
- Balloon
Statistics from Altmetric.com
Background
Loeys–Dietz syndrome (LDS) is a rare connective tissue disorder (CTD) characterized by cardiovascular, craniofacial, skeletal and neurocognitive abnormalities.1 Patients with LDS also have diffuse vascular abnormalities including an increased incidence of intracranial aneurysms.2 ,3 Due to the inherent vascular fragility in any CTD4–6 along with the significant vascular tortuosity characteristic of LDS, intracranial aneurysms represent a unique challenge in this patient population. There are a limited number of case reports in the literature describing successful treatment of unruptured LDS-associated aneurysms using both open microsurgical clipping3 ,6 and endovascular coiling.7 This is the first report of a successfully treated ruptured aneurysm, as well as the first report of successful angioplasty for refractory vasospasm in a patient with LDS.
Case presentation
A 14-year-old boy with LDS presented with a 1-day history of headache accompanied by nausea/vomiting. The location of the headache was occipital without radiation, and the pain was increasing in severity. He denied associated fever, diarrhea, abdominal pain or focal neurologic symptoms. He also denied any neck trauma, including hyperextension or rotation.
His past medical history included myxomatous mitral/tricuspid valves with aortic root dilation. His past surgical history included clubfoot repair at 1 year. All immunizations and vaccinations were up to date and there were no known allergies.
Physical examination showed an otherwise healthy young man with Marfanoid features who was afebrile with stable vital signs and a Glasgow Coma Scale (GCS) score of 14. The patient was intact and neurologic examination was non-focal; however, consciousness declined in the emergency room, necessitating intubation.
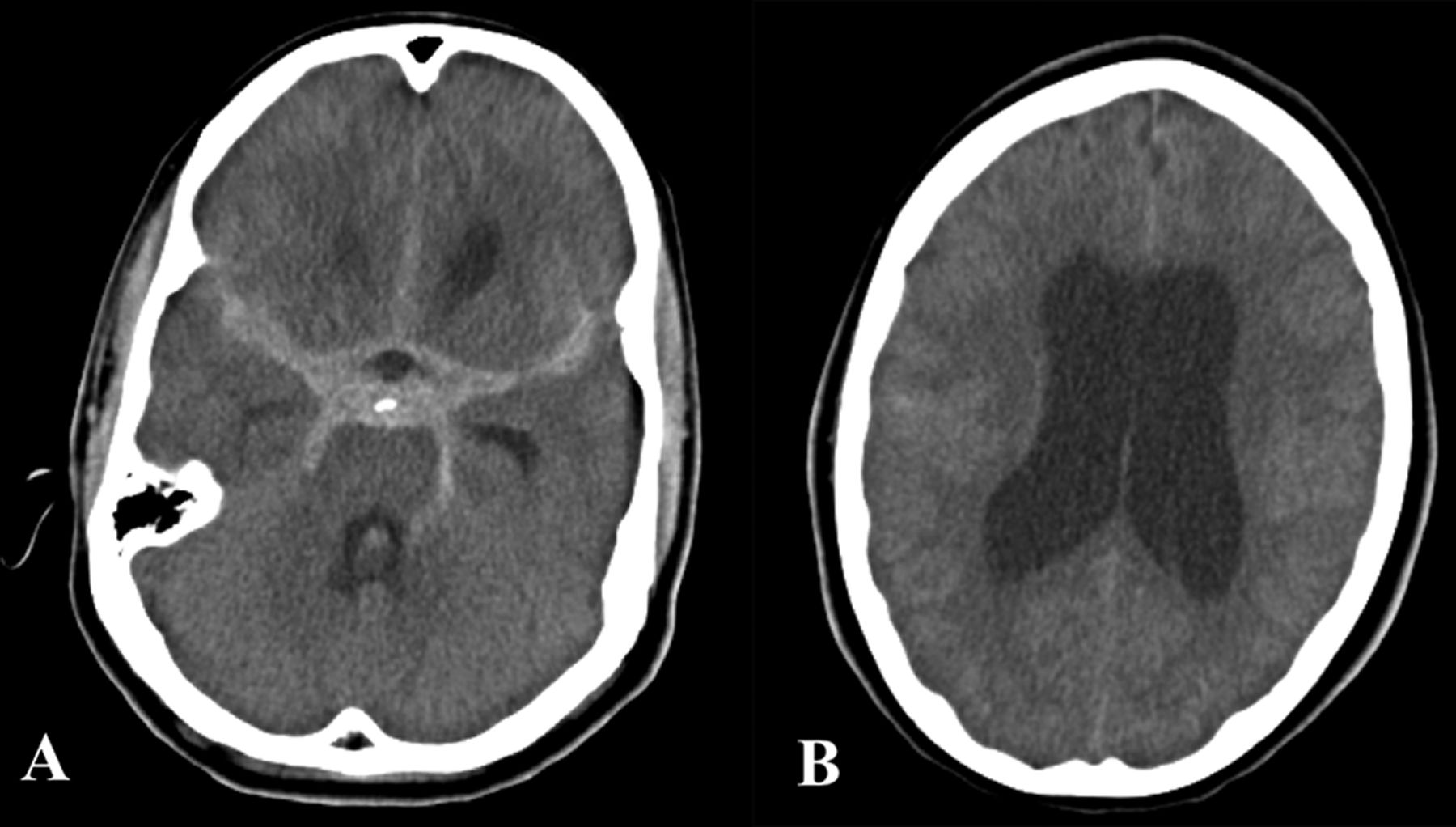
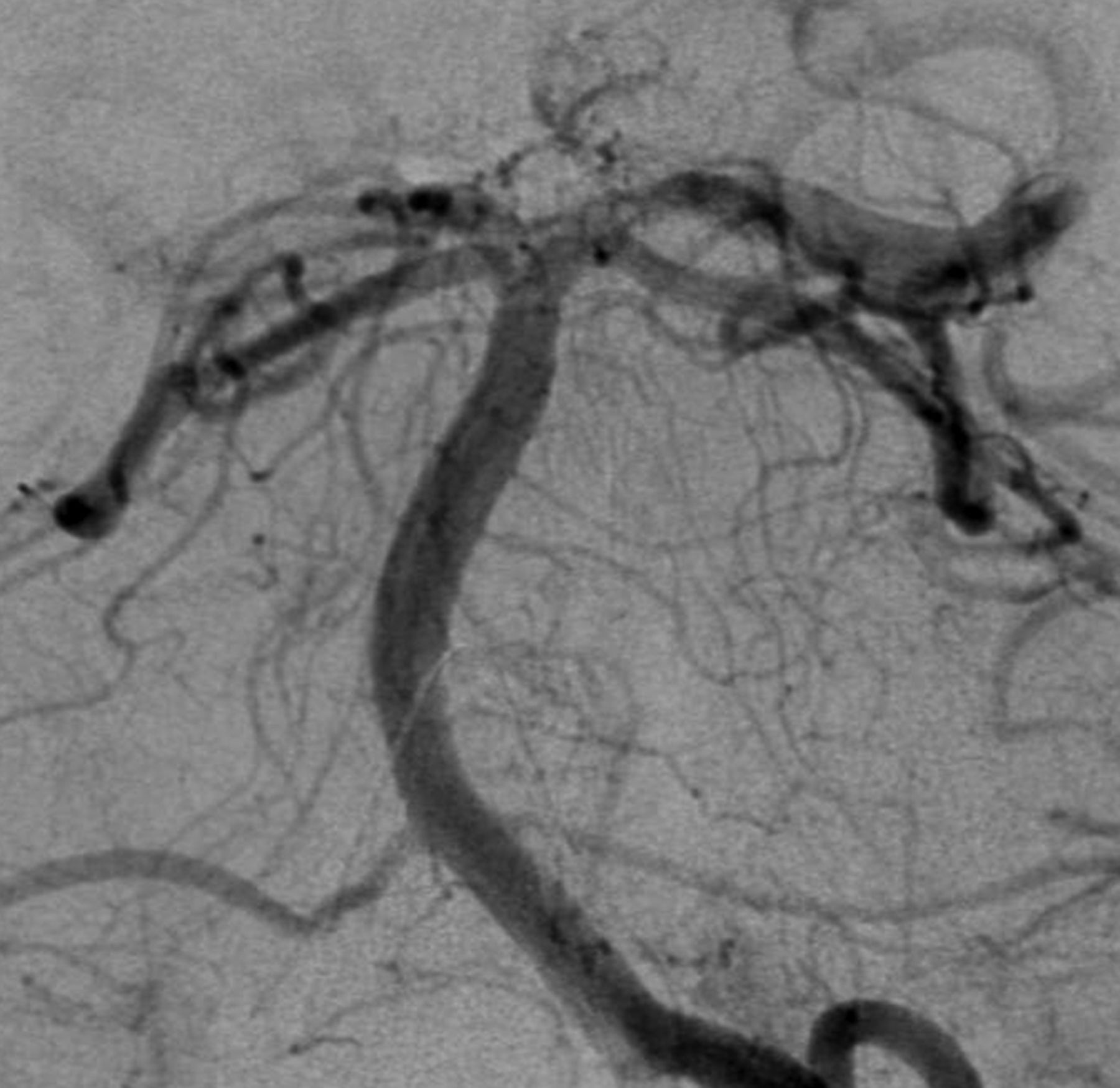
Emergency non-contrast head CT (NCHCT) showed diffuse subarachnoid hemorrhage (modified Fisher grade 3; figure 1A). Moderately severe hydrocephalus was also noted (figure 1B). Diagnostic cerebral angiography performed after placement of a right frontal external ventricular drain did not indicate an underlying aneurysm (figure 2).

(A) Non-contrast head CT scan obtained at the time of admission, demonstrating substantial subarachnoid hemorrhage involving the basal, suprasellar and sylvian cisterns and the interhemispheric fissure. (B) A higher slice in the admission head CT scan demonstrating significant dilation of the bilateral lateral ventricles.
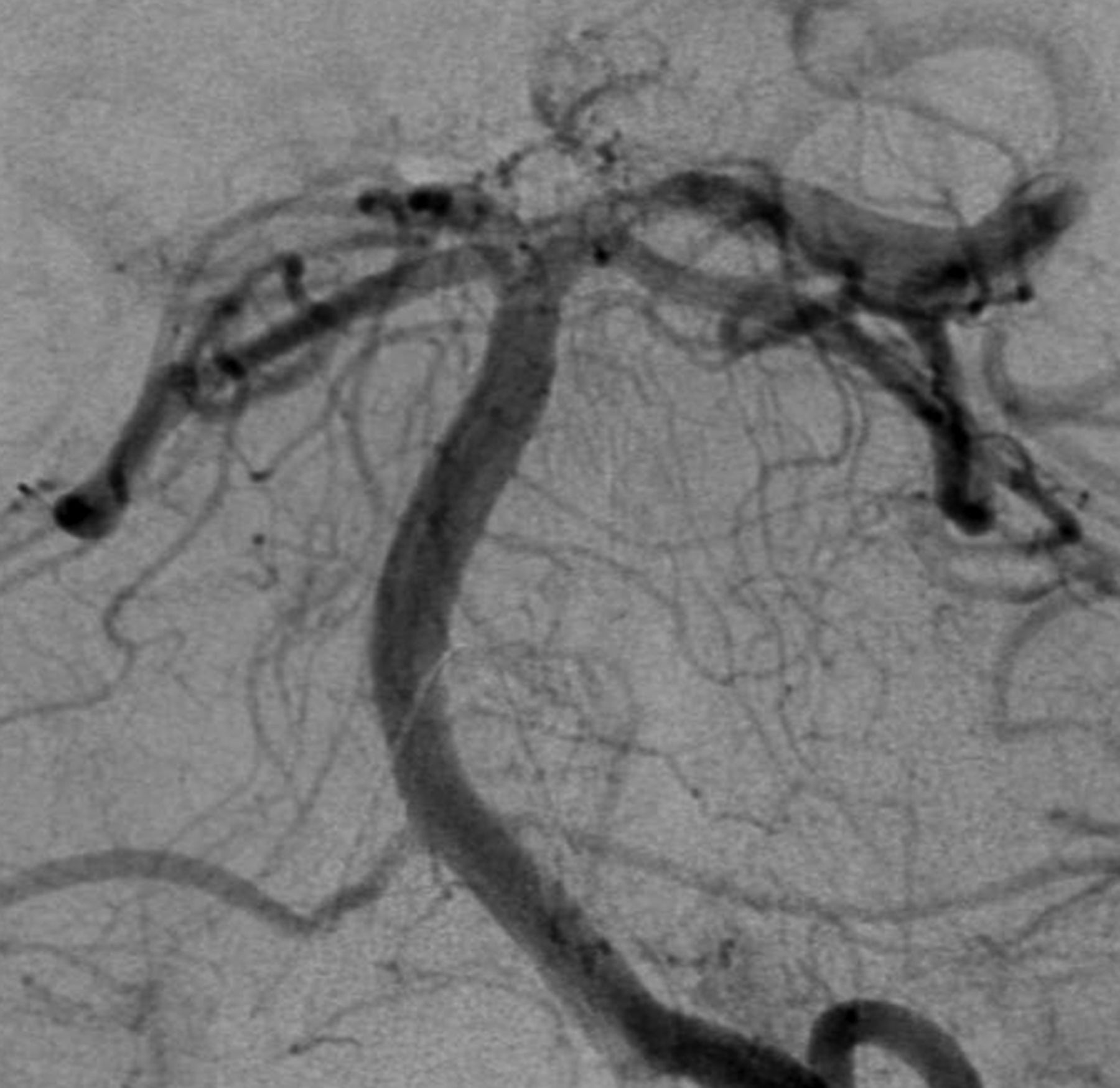
Cerebral angiography with a right vertebral artery injection demonstrating posterior circulation of normal appearance with no visible aneurysms.
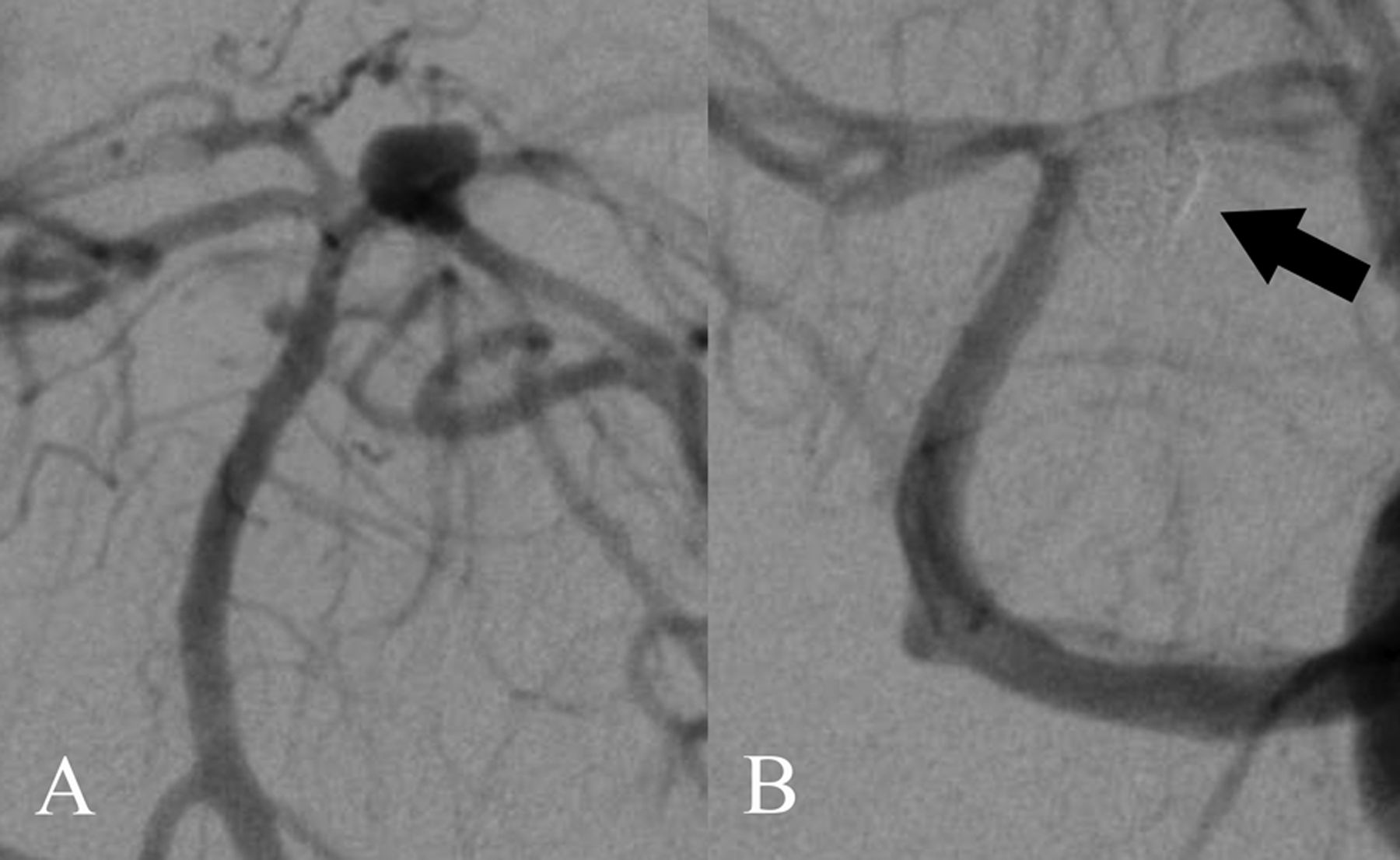
The patient was transferred to the neurointensive care unit (NICU) where his neurologic status steadily improved. On post-bleed day (PBD) 6 the patient experienced acute-onset severe headache and altered mental status that rapidly progressed to loss of consciousness. NCHCT showed acute rebleeding, with increased blood in the basal cisterns bilaterally and in the third and fourth ventricles. A left frontal external ventricular drain was placed and the patient was transported to the neurointerventional suite. Repeat angiography showed a 4×4×3 mm basilar apex aneurysm projecting ventrally (figure 3A), which was treated by endovascular coil embolization. Subsequent arteriography showed complete occlusion of the aneurysm (figure 3B).
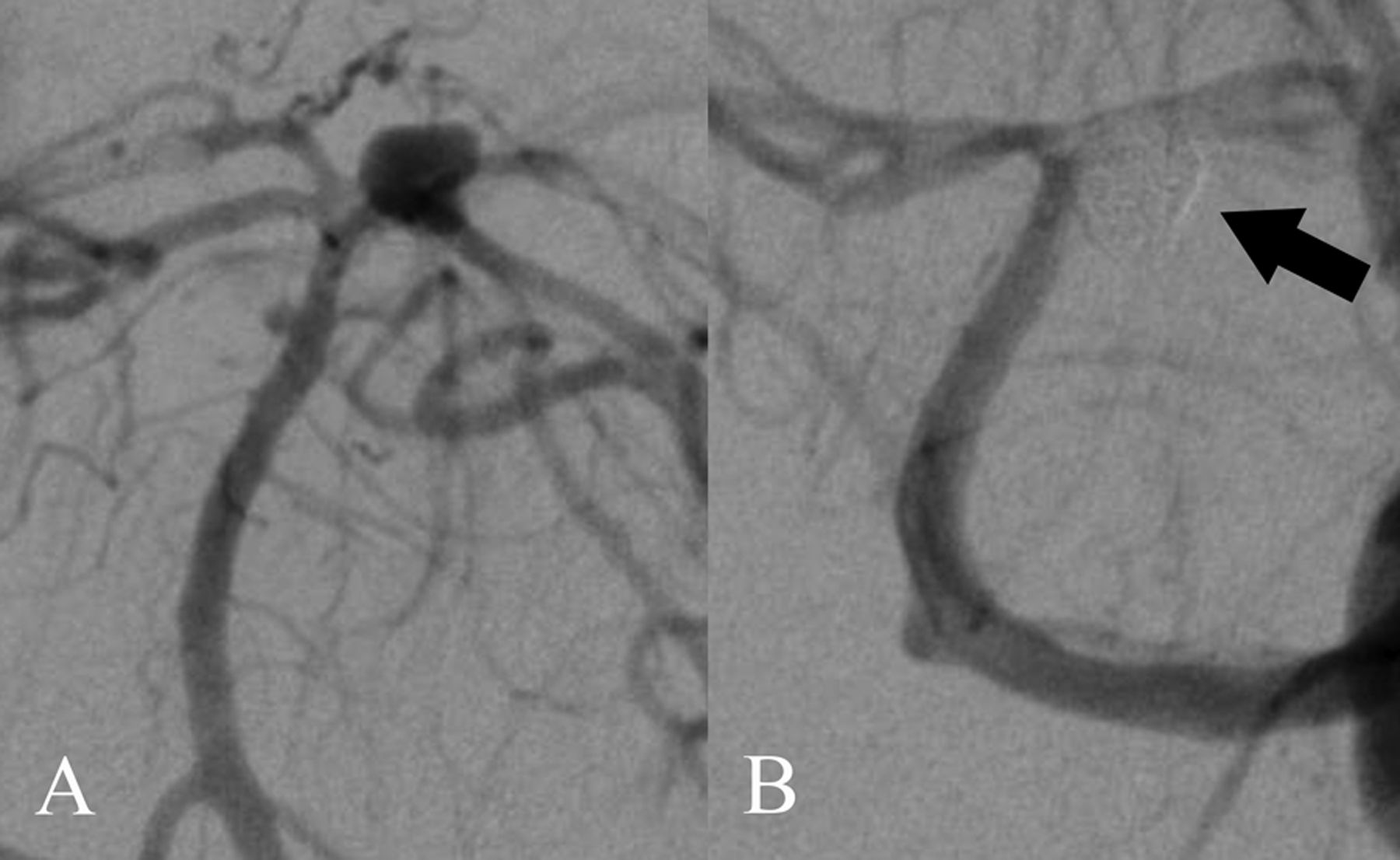
(A) Cerebral angiography with a left vertebral artery injection illustrating a ventrally projecting basilar artery apex aneurysm that was not visible on the angiogram 6 days previously. (B) Angiographic imaging obtained immediately after coil embolization of basilar artery apex aneurysm, demonstrating complete aneurysmal occlusion.
The patient was transferred back to the NICU in a stable condition. He was able to follow commands until PBD 9 when he was found to be aphasic, stuporous and unable to follow commands. The patient was sent for further radiographic investigation to assess for possible hydrocephalus, vasospasm, rebleed or stroke.
Investigations
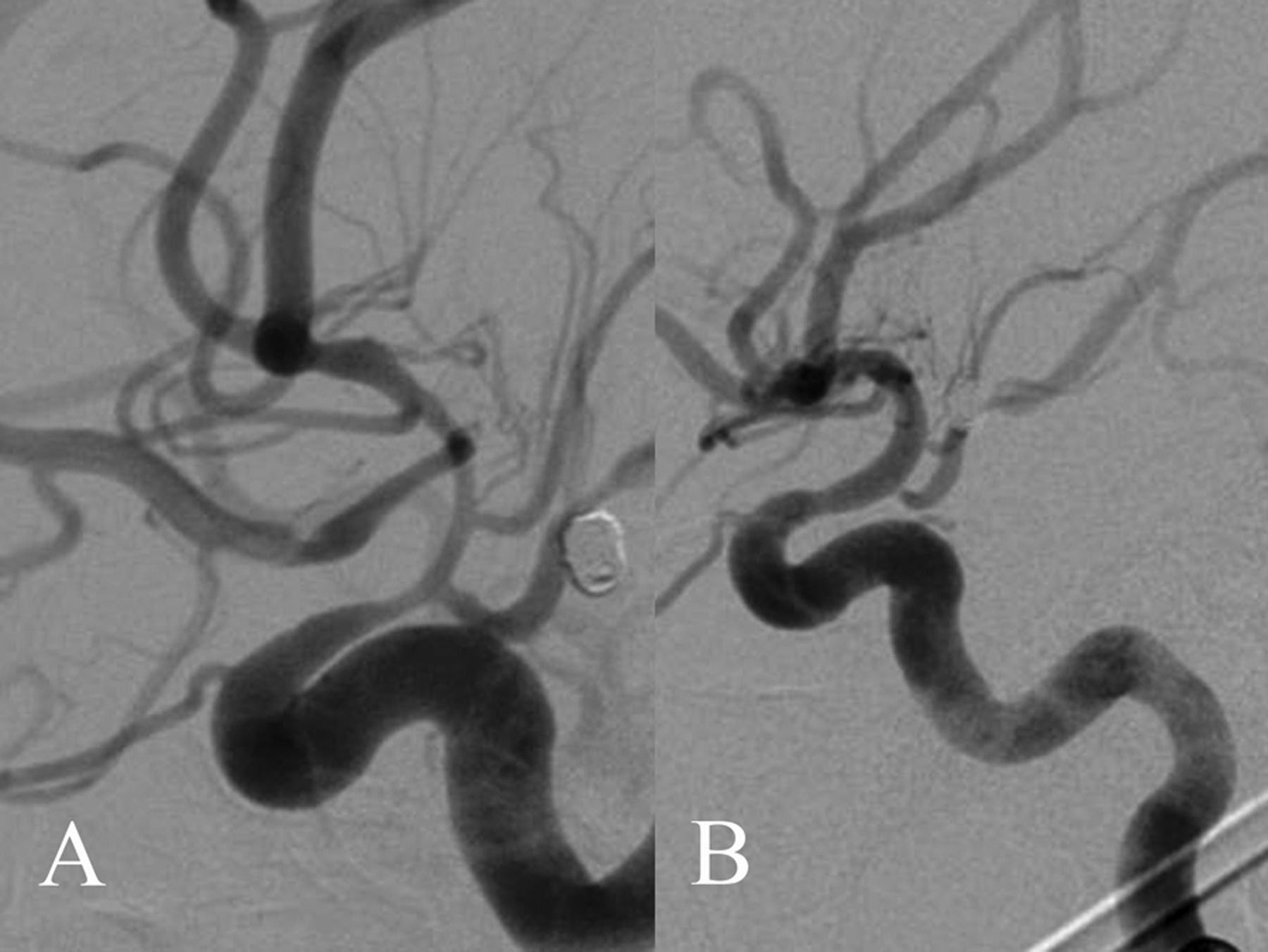
NCHCT demonstrated no significant changes compared with the previous scan. CT angiography (CTA) showed moderate to severe narrowing of the right supraclinoid internal carotid artery and narrowing of the proximal anterior and middle cerebral arteries bilaterally. Catheter angiography showed severe bilateral large vessel symptomatic vasospasm (figure 4A).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Cerebral angiography with a left internal cerebral artery injection illustrating widespread vasospasm in the anterior cerebral circulation, most pronounced in the supraclinoid internal carotid artery (ICA). (B) Angiographic image obtained immediately after angioplasty and vasodilator infusion therapy showing marked improvement of supraclinoid ICA vasospasm.
Differential diagnosis
The differential diagnosis at the time of the delayed neurologic decline (PBD 9) was: (1) hydrocephalus; (2) vasospasm; (3) rebleed; (4) thromboembolic stroke; (5) seizure; or (6) infection.
Treatment
The primary concerns were hydrocephalus and vasospasm. NCHCT did not show ventricular dilation. CTA demonstrated diffuse vasospasm of the large cerebral arteries. A trial of increased blood pressure was attempted with no improvement. Intra-arterial verapamil also failed to ameliorate the vasospasm (figure 4A). Thus, balloon angioplasty of the vasospastic vessels was performed.
This procedure was carried out using a standard balloon angioplasty technique. An EV3 HyperGlide 3×10 mm angioplasty balloon was prepared with a 0.010 inch X-pedion microguidewire to guide the catheter sequentially into each of the target vessels. Following gentle balloon angioplasty, intra-arterial verapamil (1 mg/mL normal saline) was infused to augment the mechanical treatment.
Despite concerns that the patient's CTD would predispose to vessel injury during balloon angioplasty, the procedure was well tolerated without any unintended iatrogenic cerebral branch occlusion, contrast extravasation or new mass effect. Post-procedural imaging demonstrated marked improvement of radiographic vasospasm (figure 4B).
Outcome and follow-up
Follow-up CTA on PBDs 10, 12 and 13 showed mild residual vasospasm and durable occlusion of the basilar tip aneurysm. There have been no additional neurointerventional procedures.
Discussion
Many CTDs, including LDS, carry an increased risk of cerebral aneurysm formation,3 and retrospective data indicate that LDS-associated aneurysms have a higher risk of rupture than equivalent-sized aneurysms in the general population.6 Consequently, there has been a trend towards early and aggressive surgical intervention for known unruptured LDS-associated aneurysms. Although the optimal surgical management of LDS-associated aneurysms is not well-established, relevant case reports emphasize the advantages of an open microsurgical approach.3 ,6 The justification is that CTDs are associated with a greater degree of vessel friability and fragility and therefore this patient population may be at increased risk of arterial injury with endovascular manipulation. In fact, there have been a number of case reports of significant morbidity/mortality following endovascular interventions in patients with CTDs.8 ,9 Nonetheless, Levitt et al7 recently demonstrated success in coiling such aneurysms in two patients with LDS, indicating that an endovascular approach may be considered in carefully selected LDS patients.
Patients with LDS presenting with ruptured intracranial aneurysms comprise a distinct patient population in whom endovascular intervention may be considered. The literature strongly supports early surgical intervention in aneurysmal subarachnoid hemorrhage to reduce the risk of hemorrhage10; thus, in patients with aneurysmal anatomy that is particularly favorable for an endovascular approach, the benefit of a familiar approach may outweigh the risks associated with endovascular manipulation. Furthermore, in patients with severe refractory vasospasm, more aggressive endovascular intervention (ie, angioplasty) may be indicated.
In summary, our experience supports the previous report by Levitt et al7 which demonstrated the safety and feasibility of neuroendovascular intervention in carefully selected patients with LDS. Furthermore, this is the first report of cerebral angioplasty being performed in a patient with LDS, suggesting that this is a viable treatment option in patients with LDS with severe refractory vasospasm.
Key messages
-
The differential diagnosis for acute neurologic change following subarachnoid haemorrhage is broad and includes rebleeding, vasospasm, hydrocephalus, thromboembolic stroke, seizure and infection.
-
Cerebral vasospasm is an active process of vasoconstriction with serious neurologic consequences that must be treated quickly with rapid escalation to endovascular intervention if necessary.
-
Cerebral angioplasty is a high-risk but feasible procedure for the management of vasospasm in patients with Loeys–Dietz syndrome and should be cautiously considered when all other treatment options have been exhausted.
References
Footnotes
-
Republished with permission from BMJ Case Reports Published 6 January 2014; doi:10.1136/bcr-2013-010857
-
Contributors PMM was the primary attending involved in the care of the patient whose case was presented. He revised the paper and is the guarantor. CPK was the primary resident involved in the care of the presented patient. He also was the primary writer of the paper. ESS and CD contributed background research, assistance with drafting of the paper and revisions of the paper.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed