Article Text

Abstract
Introduction Despite successful recanalization with mechanical thrombectomy (MT) for acute anterior ischemic stroke (AAIS), the number of passes may impact clinical outcome.
We analyzed the impact of more than three MT passes (>3) in a trial that evaluated contact aspiration (CA) versus stent retriever (SR) as the first-line technique in AAIS.
Methods We included patients with mTICI 2b/3 recanalization after MT for isolated intracranial occlusions. The primary outcome was the percentage of patients with a 90-day modified Rankin Scale (mRS)≤2. Secondary outcomes included overall distribution of 90-day mRS, parenchymal hematoma on 24 hours' brain imaging (PH), and 90-day mortality.
Results Among the 281 patients included and even after adjustment on time to recanalization, significantly more patients with >3 passes had PH than patients with ≤3 passes in multivariate analysis (adjusted OR, 3.62; 95% CI, 1.55 to 8.44). When the analyses were stratified according to CA vs. SR, patients with >3 passes had a stronger risk of PH than patients with ≤3 passes, only in the SR first-line-treated group (adjusted OR, 9.24; 95% CI, 2.65 to 32.13) and not in the CA first-line-treated group (adjusted RR, 1.73; 95% CI, 0.57 to 5.19). A negative association of borderline significance (P=0.07) between >3 passes and favorable outcome was observed only in SR first-line-treated patients (adjusted OR, 0.33; 95% CI, 0.09 to 1.11).
Conclusions After three passes of SR and unlike for three passes of CA, there is an increased risk of PH and a trend toward a worse clinical outcome.
- device
- thrombectomy
- technique
- stroke
Statistics from Altmetric.com
Introduction
After the demonstration of the superiority of mechanical thrombectomy (MT) over standard medical management alone, the current challenges in the field focus on reducing time to recanalization, optimizing imaging methods for patient selection, and evaluating the best technical approach.1 2 Indeed, the first studies on large patient registries have pointed to rapid recanalization of the target-occluded vessel as the ‘Holy Grail’.3 4 However in the randomized contolled trials (RCTs), all mTICI scores of 2b or 3 were considered as successful recanalization, regardless of the number of passes used.1 5
A few small retrospective studies have shown that the number of passes required to reach such ’successful' recanalization could be related to the clinical outcome of patients.6–11 Hence, difficult recanalization after numerous passes could explain the so-called ’futile' recanalizations, where patients do not achieve clinical independence at 3 months (mRS >2), despite having reached an mTICI 2b/3 score after MT.12 Such ‘futile’ recanalizations account for more than 20% of cases in RCTs and constitute a critical target for efforts to improve the results of stroke management in the MT era.1
The ASTER trial aimed to compare the efficacy and safety of first-line MT using the contact aspiration technique versus the standard stent retriever (SR) technique.13 Patients underwent their assigned endovascular procedure (CA or SR) with three passes before switching to another strategy.14 This trial included more than 300 patients treated with two standardized, validated MT strategies, and thus represents adequate material to isolate and study the implication of more than three MT passes in the results of endovascular treatment for acute ischemic stroke patients. Here we aimed to analyze the effect of successive MT passes by including only TICI2B/3 patients and thus focusing on these so-called ‘futile’ recanalizations.
Methods
Study design
The trial design has already been published.14 The ASTER trial is a prospective, randomized, multicenter, controlled, open-label, blinded endpoint (PROBE) clinical trial designed to compare first-line MT strategy, CA and SR, in terms of recanalization rates at the end of the endovascular procedure. Eight high-volume, comprehensive stroke centers in France included patients all of which regularly perform both CA and SR. The study, was registered with ClinicalTrials.gov (Identifier NCT02523261) and conducted in accordance with the Declaration of Helsinki and Good Clinical Practice. The study protocol and the consent form were approved by the Comité de Protection des Personnes Ile de France VI (ID 2015-A00830 −49).
Patient population
Patients admitted with a suspicion of ischemic stroke secondary to occlusion of the anterior circulation within 6 hours of symptom onset were included. Inclusion and exclusion criteria of the ASTER trial were published in the protocol.
For the present analysis, we analyzed patients who benefit from MT for isolated intracranial occlusion (ICA, MCA-M1, or MCA-M2) on first-line imaging and achieving mTICI 2b/3 recanalization at the end of the endovascular procedure. An independent and experienced core laboratory analyzed all baseline imaging and angiographic results blindly.
Interventions
In line with the recommendations of the American Stroke Association and the European Stroke Organization, enrolled patients were given intravenous rt-PA (if they were eligible) and were transferred quickly to the catheter laboratory for urgent MT.15 Patients underwent their assigned endovascular procedure (CA or SR) under general anesthesia or conscious sedation. Both techniques were conducted in accordance with good practice recommendations (minimum of three passes before switching to another strategy: use of a proximal occlusion balloon with the SR). The CA approach was previously reported.16 17
Outcomes
The primary outcome for the present post-hoc analysis of the ASTER trial was the percentage of patients with favorable outcome defined as a 90-day modified Rankin Scale (mRS) score 0 to 2. Secondary outcomes included the degree of disability assessed by overall distribution of the 90-day mRS (shift analysis combining scores of 5 and 6), any intracerebral hemorrhage, parenchymal hematoma (according to the European Cooperative Acute Stroke Study 3 classification) and subarachnoid hemorrhage within 24 hours, and 90-day all-cause mortality.
Statistical analysis
All analyses were performed among the patients with isolated anterior circulation occlusion (MCA and/or ICA) and successful recanalization by a mechanical device (at least one pass, and at least mTICI 2b grade at the end of the endovascular procedure).
Categorical variables were expressed as frequencies and percentages, and continuous variables as means (SD) or medians (IQR) for non-normal distribution. Normality of distributions was assessed graphically and by using the Shapiro–Wilk test. Baseline characteristics were described and compared according to the number of passes (≤3 versus>3) using the Chi-Square or Fisher’s exact tests for categorical variables, and Student’s t or Mann–Whitney U tests for continuous variables, as appropriate.
Using ≤3 passes to achieve successful recanalization as the reference, we assessed the prognostic value of >3 passes on favorable outcome, any intracerebral hemorrhage, parenchymal hematoma, subarachnoid hemorrhage, and 90-day mortality using univariable binary logistic regression models. The prognostic value of >3 passes on the degree of disability (shift analysis after combining 90-day mRS of 5 and 6)18 was assessed using an ordinal logistic regression model. Associations between >3 passes and outcomes were further investigated in multivariable mixed logistic (binary or ordinal) regression models including center as random effect and the following pre-specified confounders as fixed effects: first-line MT strategy (CA vs SR), age, admission NIHSS and ASPECTS, pre-stroke mRs≥1, intravenous rt-PA, onset to recanalization time, and recanalization grades (mTICI 2b vs 2 c/3). We investigated the heterogeneity in the association between >3 passes and outcomes according to first-line MT strategy (CA vs SR) by including the corresponding interaction term in the multivariable logistic regression models.
Statistical testing was conducted at the two-tailed alpha level of 0.05, except tests for heterogeneity, in which an alpha level of 0.10 was chosen. Data were analyzed using the SAS software package, release 9.4 (SAS Institute, Cary, NC).
Results
Between October 2015 and October 2016, a total of 381 patients were randomized in the ASTER trial. Of them, 281 patients were eligible to be included in the present study (online supplementary figure 1). Reasons for exclusion were: no MT performed (n=45), patients with tandem occlusion (n=11), and failure to reach successful recanalization (mTICI 0-2a, n=44). The median number of passes to achieve successful recanalization was two (IQR, 1 to 3) and the median time from clot contact to successful recanalization was 18 min (IQR, 8 to 38). Sixty-nine (24.6%) patients achieved successful recanalization after more than three passes. Parenchymal hematoma within 24 hours occurred in 43 patients (15.2%; 95% CI, 10.9 to 19.5; PH1 [n=27]; PH2 [n=16]). Among the 270 patients with 90-day follow-up information, 143 patients had a favorable outcome (53.0%, 95% CI, 47.0 to 59.0) and 42 died (15.6%; 95% CI, 11.2 to 19.9).
Supplementary file 1
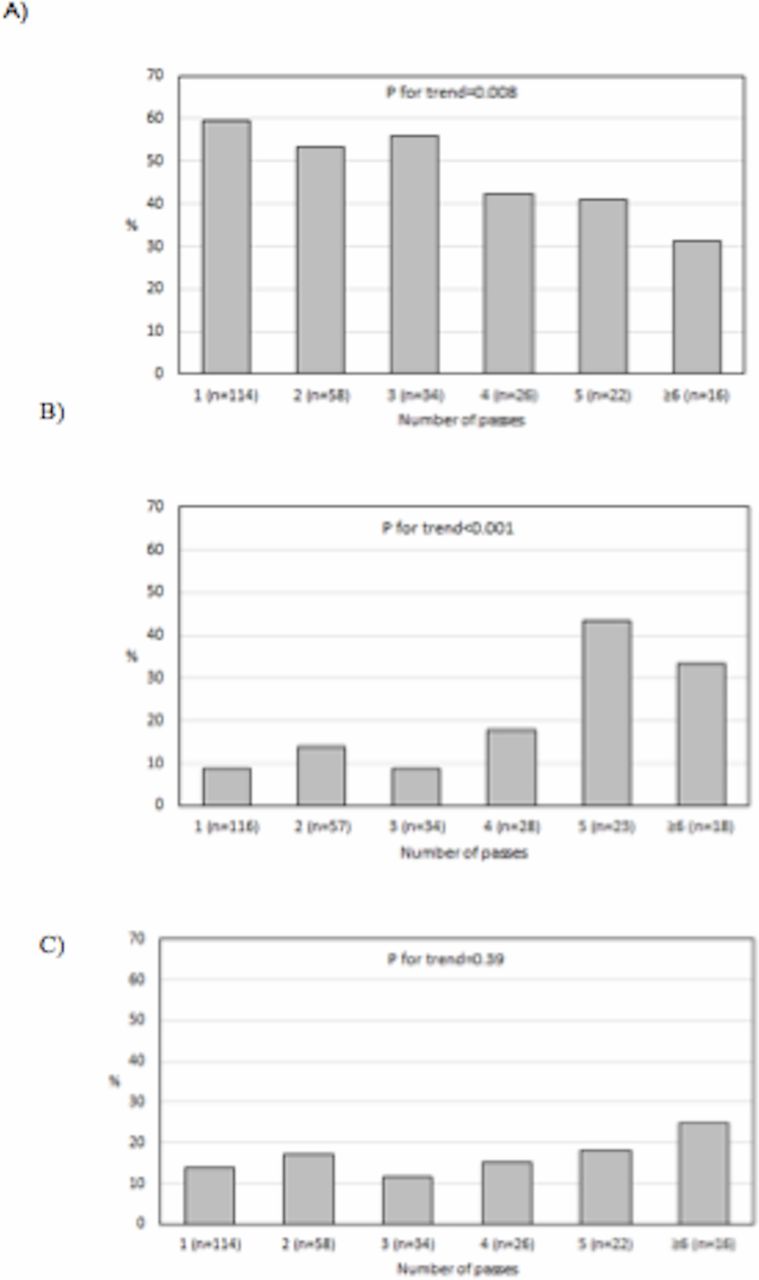
Baseline characteristics are described in table 1 for the overall study sample and number of passes (≤3 versus>3). From the study of baseline characteristics, only ASPECTS differed significantly between patients with and without more than three passes: patients requiring more than three passes to achieve successful recanalization had a lower ASPECTS score than patients requiring three or less passes. Patients having undergone more than three passes had less often been treated with CA as first-line strategy, and as expected, reached complete recanalization less often and had greater time to recanalization than patients with three or less passes. Rate of favorable outcome, any intracerebral hemorrhage, parenchymal hematoma, and 90-day all-cause mortality according to number of MT passes to achieve successful recanalization are reported in figure 1. In univariate analysis, patients with more than three passes had a favorable outcome less often than patients with three or less passes (39.1% vs 57.3%, P=0.012). However, after pre-specified adjustment on confounding factors (center, first-line MT device, age, NIHSS, ASPECTS, intravenous rt-PA, onset to recanalization time, and mTICI grades), this difference was no longer significant (adjusted OR, 0.64; 95% CI, 0.29 to 1.43). Similar results were found when analyzing the degree of disability (online supplementary figure 2), with an adjusted OR for 1-point improvement of 0.73 (95%CI, 0.41 to 1.29). As shown in table 2, in univariate analysis, significantly more patients submitted to more than three passes presented intracerebral hemorrhage or parenchymal hematoma than patients having undergone three or less passes. However, only the difference in parenchymal hematoma remained significant in multivariate analysis (adjusted OR, 3.62; 95% CI, 1.55 to 8.44). No such difference was observed with all-cause mortality (table 2).

Rate of favorable outcome (A), parenchymal hematoma (B), and 90-day all-cause mortality (C) according to number of thrombectomy device passes to achieve successful recanalization (mTICI 2b/3).
Characteristics of patients with successful recanalization after thrombectomy, overall and according to number of passes (≤3 vs>3)
Comparison in outcomes according to number of passes (≤3 vs.>3) among patients with successful recanalization (mTICI 2b/3) after mechanical thrombectomy
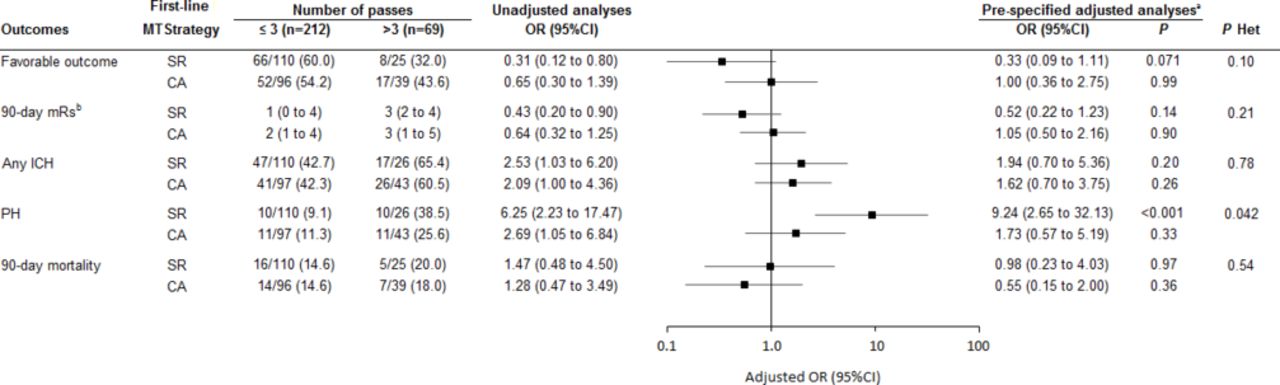
When the analyses were stratified according to the first-line therapy (CA vs SR), there was a significant heterogeneity in effect size of >3 passes for parenchymal hematoma (figure 2). We observed that patients having undergone more than three passes presented more parenchymal hematoma than patients with three or less passes in the SR first-line-treated group (adjusted OR, 9.24; 95% CI, 2.65 to 32.13) while no such difference was found in the CA first-line-treated group (adjusted RR, 1.73; 95% CI, 0.57 to 5.19). Regarding favorable outcome, the heterogeneity test in effect of >3 passes according to first-line strategy did not reach significance (P=0.10). However, we observed a negative association between >3 passes and favorable outcome in SR first-line-treated patients (adjusted OR, 0.33; 95% CI, 0.09 to 1.11) whereas no such association was observed in CA first-line-treated patients (adjusted OR, 1.00; 95% CI, 0.36 to 2.75).
{kind=link}
{kind=link}
Pronostic values of >3 passes to achieve successful recanalization (mTICI 2b/3) on outcomes according to first-line thrombectomy strategy (contact aspiration versus stent retriever). acalculated using mixed (binary or ordinal) logistic regression models including center as random effect, age, admission NIHSS, ASPECTS, pre-stroke mRS ≥1, intravenous rt-PA, onset to recanalization time, and mTICI grades (2b vs 2 c/3). bshift-analysis (median and IQR values and OR per 1-point improvement in mRS are reported). ASPECTS, Alberta stroke program early CT score; CA, contact aspiration; NIHSS, National Institutes of Health Stroke Scale; mRS, modified Rankin scale; mTICI, modified treatment in cerebral infarction score; PH, parenchymal hematoma; rt-PA, recombinant tissue plasminogen activator; SR, stent retriever.
Discussion
The main finding of our analysis is that, after adjustment for classical factors and, above all, the time between symptom onset and recanalization, after three passes of SR, unlike after three passes of CA, there is an increased risk of parenchymal hematoma and a trend toward a worse clinical outcome. This points to the importance in MT of the number of passes, irrespective of time factors. This conclusion was possible because we focused on ‘futile’ recanalizations by including only TICI2b/3 patients.
Successive MT passes may cause vascular injury, which is associated with increased risk of parenchymal hematoma. A previous study analyzed 632 patients and found that more patients with SICH had undergone >3 passes, when compared with patients without SICH.10 However, no accurate adjustment on time between onset of symptoms and recanalization was applied in that study. Indeed, patients with a lower number of passes had a faster procedure time, which may also have contributed to better results of treatment. Hence, in a collaborative-pooled database analysis, each 30 min decrease in time between symptom onset and recanalization was associated with a 20% reduction in intracranial hemorrhage.3 In order to isolate as far as possible the effect of passes, we also adjusted our analysis to final TICI results because emerging results have recently emphasized that an mTICI 3 leads to better outcomes in terms of mRS at 3 months than an mTICI 2b.19
CA and SR were both used in the enrolled group, but it appears that these two methods are quite different in their mechanism of action, which may also affect the degree of vessel damage. The device may be responsible for dissection undetectable on angiography, or endothelial injury leading to ongoing in situ thrombosis. SR stent retrievers dragged through an atherosclerotic lesion may be more harmful than contact aspiration. Furthermore, another potential mechanism for an increasing rate of parenchymal hematoma could be chronic hypo perfusion in the distal territory in cases of reduced auto regulation leading to reperfusion hemorrhage.20–23
Recently Zaidat et al showed, in the NASA registry, that patients with mTICI 3 after one pass had a better clinical outcome, lower mortality, and fewer procedural adverse events.24 However, this retrospective study included patients who were treated with heterogeneous strategies, and radiological/clinical outcomes were self-adjudicated. A few small retrospective studies have shown that the number of passes required to reach successful recanalization was associated with clinical outcome.6 Linfante et al also reported that ≥3 passes was an independent predictor of poor 90-day outcome associated with age ≥80 years, ICA/basilar occlusion site, initial NIHSS score ≥18, absence of intravenous rt-PA infusion, and use of rescue therapy.7
Furthermore, our study has several assets. First, our data were recorded in a prospective, randomized, multicenter, controlled trial that included a large number of patients treated with MT. Second, in the ASTER trial, the MT strategy applied for each patient included was recorded. This enabled us to isolate the effect of passes in a very homogenous population and to analyze the results according to the first-line strategy allocated (CA or SR). We also excluded tandem and extracranial occlusions to analyze the passes targeting the primary intracranial occlusion site.
Our work has some limitations. First, probably because of too small a sample size in the SR group, we only found a borderline negative association between >3 passes and favorable outcome. Second, we studied all parenchymal hematoma (PH 1 and PH2) instead of only symptomatic hemorrhages. Indeed, PH1 is common in the natural risk of large infarcts, and most of the parenchymal hemorrhages were small (27 PH1 compared with 16 PH2). PH1 are often asymptomatic within the territory of the acute infarct. Third, there was no thrombus histology data available to further characterize the relationship of passes with thrombus type.25 26 Lastly, we were unable to analyze the vessel permeability at 24 or 48 hours after MT. This would have been of interest in investigating a link between numerous passes and potential delayed re-thrombosis that could participate in worsening of the clinical outcome.
Conclusion
After three passes of SR and, unlike after three passes of CA, there is an increased risk of parenchymal hematoma and a trend toward a worse clinical outcome. Furthermore, the number of SR passes is not only a surrogate marker for delay to recanalization but also an independent factor related to the results of the procedure. Hence, when opting for MT with SR, one should try as far as possible to reach an optimal recanalization within three passes in order to limit the risk of parenchymal hematoma. Even if a good recanalization is still the final aim of MT, we provide here arguments for attempting to choose, at the outset, the most suitable strategy in order to minimize the number of passes. This may depend on the type of occlusion. Further research should focus on developing means of determining the optimal endovascular strategy for each patient to obtain recanalization with a minimal number of passes (supplementary figure and table).
Supplementary file 2
Acknowledgments
We thank Malek Ben Maacha, clinical research associate (Department of Diagnostic and Interventional Neuroradiology, Rothschild Foundation, France) for serving as the main clinical research associate for the trial and we thank Mary Osborne-Pellegrin for her help in editing the final draft of the article. These persons did not receive specific compensation for their work related to this study.
References
Footnotes
Contributors RB conceived the study and wrote the manuscript. SS, MM, RF, RB, BG, MK, GM, SB, HD, AC, MP, and BL have collected data and critically reviewed the manuscript. JL and MK performed the statistical analysis.
Funding The ASTER trial research was sponsored by Fondation Ophtalmologique Adolphe de Rothschild. An unrestricted research grant was provided by Penumbra, Alameda, California.
Competing interests None declared.
Patient consent Obtained.
Ethics approval ClinicalTrials.gov (Identifier NCT02523261), was conducted in accordance with the Declaration of Helsinki and Good Clinical Practice. The study protocol and the consent form were approved by the Comité de Protection des Personnes Ile de France VI (ID 2015-A00830 -49). In the present study, we conducted a post-hoc analysis of the data from the ASTER trial.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data are available upon request from the corresponding author.
Collaborators The ASTER trial investigators are: Piotin M, Blanc R, Redjem H, Ciccio G, Smajda S, Mazighi M, Fahed R, Desilles JP, Lapergue B, Rodesch G, Consoli A, Coskun O, Di Maria F, Bourdain F, Decroix JP, Wang A, Tchikviladze M, Evrard S, Turjman F, Gory B, Labeyrie PE, Riva R, Mounayer C, Saleme S, Costalat V, Bonafé A, Eker O, Gascou G, Dargazanli C, Bracard S, Tonnelet R, Derelle AL, Anxionnat R, Desal H, Bourcier R, Daumas-Duport B, Berge J, Barreau X, Margnat G, Djemmane L, Labreuche J, Duhamel A.