Article Text

Abstract
Background Complete packing of intracranial aneurysms has demonstrated a significant decrease in aneurysm recurrence rates with increased volumetric filling. The HydroCoil Embolization System (HES) was developed to increase volumetric filling within the aneurysm sac to maintain long term occlusion. To further enhance ease of HES deployment, a new next generation embolic coil, the HydroFill coil, was developed.
Objective To report the first clinical experience with the HydroFill coil, focusing on safety and effectiveness, with immediate and long term follow-up on cases performed at a single institution by a single operator.
Methods Retrospective angiographic and clinical analysis was performed on a non-randomized single arm registry of the first consecutive 11 patients with 14 intracranial saccular aneurysms treated during a 9 month period.
Results The immediate angiographic occlusion rate according to the Raymond scale was 100%. Overall packing density of all coils used was 13–135% (mean 64%). The immediate complication rate was 9% (1/11 patients), secondary to a parent vessel occlusion which resolved after intravenous administration of eptifibatide (Integrilin) without neurological sequelae. The angiographic/MR angiography follow-up period for this series was 13–30 months, with an overall complete occlusion rate of 86% (12/14 aneurysms). 2/14 aneurysms (14%) converted from complete occlusion to filling of small neck remnants. Of the two, one (7%) was a cavernous aneurysm that was retreated.
Conclusions Although this initial case series is small, this study demonstrates safe deployment of the HydroFill coil in ruptured and unruptured aneurysms without major complications, and with a high rate of occlusion on long term follow-up.
- Aneurysm
- Coil
- Device
- Angiography
- Intervention
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
Since its inception in the early 1990s, endovascular intrasaccular embolization has been well established as a successful alternative to open surgical clipping of intracranial aneurysms.1–8 However, historical publications only demonstrated the usefulness of platinum coils—for example, the first randomized controlled trial, the International Subarachnoid Aneurysm Trial, demonstrated the superiority of endovascular coiling using platinum coils over surgical clipping.4
More recently, the HydroCoil Endovascular Aneurysm Occlusion and Packing Study (HELPS) compared packing density of bare platinum coils with that of HydroCoils (hydrogel coated platinum coils; MicroVention Inc, Tustin, California, USA).9 In this randomized controlled trial, recurrence and retreatment rates at the 6–12 month follow-up were superior in the HydroCoil Embolization System (HES) arm, with overall recurrence rates of 27% compared with 36% in the bare platinum arm, and overall retreatment rates of 2% and 4%, respectively.9
Although there was no significant difference between the two arms with respect to operator assessed angiographic occlusion, HELPS9 also demonstrated that in the HES arm, fewer patients had a major aneurysm recurrence, and ruptured aneurysms had better outcomes. There was a lower thromboembolic rate in the Hydrocoil arm versus the platinum arm (5.6% vs 10%), a higher packing density of 63.9% versus 23.2%, and a trend toward better outcomes in the medium sized aneurysm group.9
These findings may be due to the design of the HydroCoil system, which was developed to increase volumetric filling within the aneurysm sac.10 This hybrid platinum coil consists of a platinum coil covered with an outer layer of hydrogel. The hydrogel material expands over a predetermined amount of time (20 min maximum), reducing the dead spaces between coil loops inside the aneurysm.10 This modified second generation coil system, although not a bioactive coil, has been shown to produce a high occlusion rate with low recanalization rates.11–23
The new HydroFill coil (MicroVention) is similar in design to the existing HydroFrame and HydroSoft coils (MicroVention), with a platinum overcoil and a proprietary hydrogel material within the central lumen of the coil. Once activated, the hydrogel material swells through the winds of the platinum coil (figure 1). In experimental aneurysms, Killer et al24 demonstrated that the HydroFill coil had increased volumetric occlusion versus that of the HydroCoil 10 and platinum groups. There was progressive occlusion in the HydroFill group, with an increase in neointimal formation and thrombus organization.24
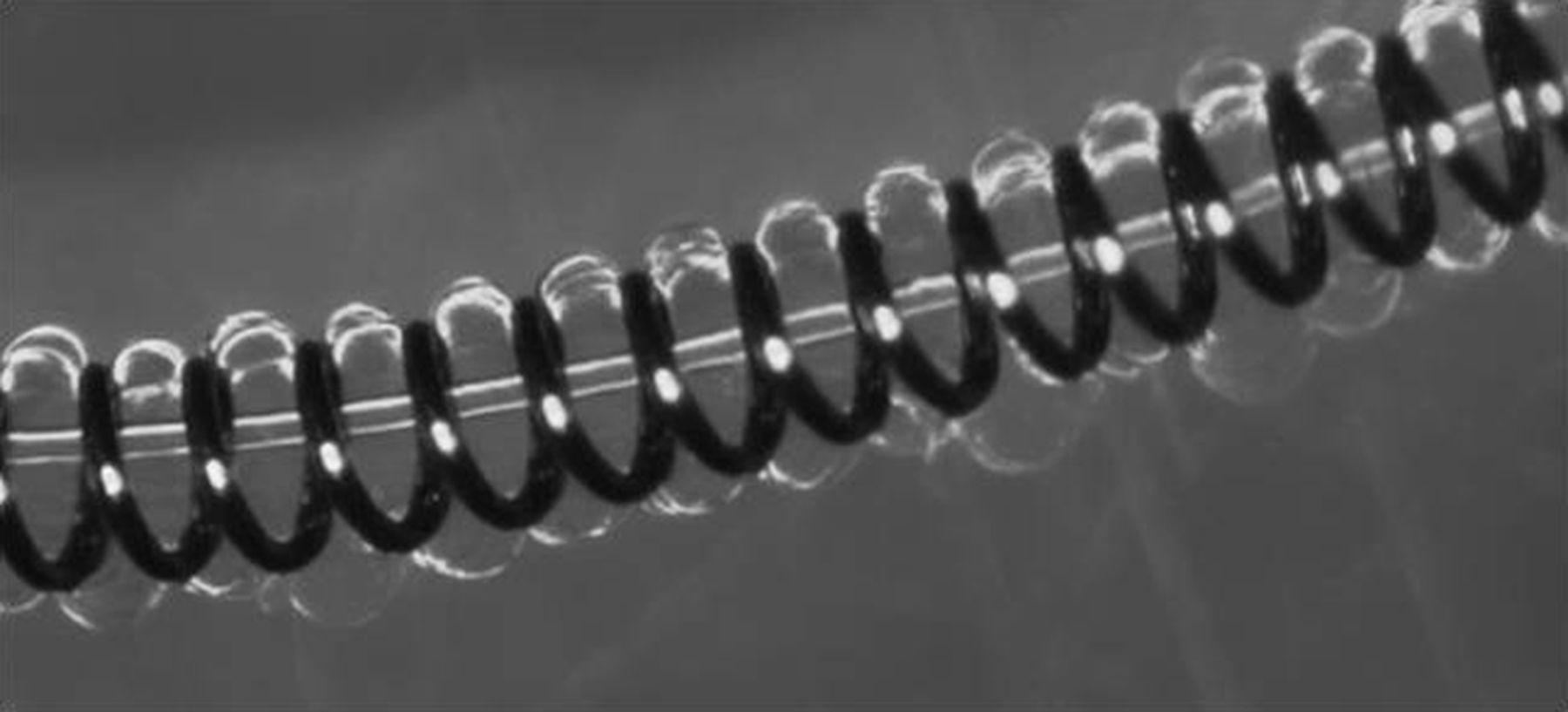
HydroFill Coil—Hydrogel core with a platinum overcoil.
Our aim in this study was to report the first clinical experience with the new HydroFill coil, focusing on its safety and effectiveness, with immediate and long term follow-up on cases performed at a single institution by a single operator.
Materials and methods
Between February 2010 and November 2010, 11 patients (nine women, two men) presenting to Hotel-Dieu Grace Hospital with 14 intracranial aneurysms (10 unruptured, four ruptured) were treated with at least one HydroFill coil. Mean age was 48.5 (range 28–69) years. This was a non-randomized, retrospective study, and no inclusion or exclusion criteria, including aneurysm morphology, were used.
Endovascular treatment
All patients had diagnostic cerebral angiograms performed in multiple angiographic projections (including three-dimensional angiography) during the initial patient workup to characterize the morphology of the entire aneurysm for size and location, including the neck of the aneurysm sac along the parent vessel interface.
A 6 French Burke Envoy guide catheter (Codman Neurovascular, Raynham, Massachusetts, USA) was placed into the parent vessel harboring the target aneurysm. This guide catheter allowed the delivery of two coaxial microcatheters (balloon catheter and microcatheter) simultaneously through a single guide catheter.25 ,26 An Excelsior 1018 or SL-10 (Stryker-Neurovascular, Kalamazoo, Michigan, USA) was the primary microcatheter used to deploy the embolic coils within the aneurysm sac. All aneurysms were treated with a simple single catheter technique without the need for balloon remodeling.
The general treatment strategy was to frame with a platinum Microplex framing coil (MicroVention) or a HydroFrame coil, fill with one or more HydroFill coils, and finish with a HydroSoft coil. All coils deployed had a secondary outer diameter ranging from 0.012 to 0.015 inches in this series. The aneurysms were treated with endosaccular placement of multiple coils, including the HydroFill coil. If the specific target aneurysm had a wide neck, the aneurysm was framed first with platinum or HydroFrame to form a stable coil basket; however, if the target aneurysm had a small neck, the aneurysm was coiled using the HydroFill coil as the primary coil. All aneurysms were treated until angiographic occlusion was achieved, or until no further coils could be safely deployed within the sac.
Although each aneurysm in this series was not similar in shape, a simple volume calculation was used for each aneurysm:
The HydroCoils used in this series had an outer diameter of 0.012–0.015 inches prior to hydrogel expansion. The volume of the coils was then calculated by the following formula. However, this assumes that there is full circumferential expansion of each coil:
The complete aneurysm packing density was then calculated by using this formula:
Patients were not treated with any extra antiplatelet therapy secondary to the use of the hydrogel coils. No perioperative antiplatelet therapy was routinely administered, as none of the patients had pre-existing stents.
Angiographic/MR angiography follow-up observation
The immediate angiographic imaging post treatment as well as follow-up imaging was evaluated and classified using the Raymond27 and modified Roy5 Scales by an independent radiologist (BDA) who was not associated with the endovascular treatments. Follow-up imaging consisted of digital subtraction angiography (DSA) or contrast enhanced MR angiography (CE-MRA). As some studies28 ,29 have indicated that CE-MRA is superior to DSA in evaluating recurrences, the standard of care at our institution in the follow-up period is CE-MRA unless clinically indicated to use DSA for evaluation. However, an immediate CE-MRA was not utilized prior to discharge but only utilized as the follow-up imaging technique.
Results
The aneurysms were successfully occluded utilizing a combination of a platinum frame, HydroFrame, HydroFill, and/or HydroSoft coils. The HydroFill coil was placed successfully in all patients without any difficulty in deployment. The immediate occlusion rate in all aneurysms (14/14) was 100%, corresponding to class 1 according to the Raymond Scale.5 ,27
The overall total calculated filling volume with all coils deployed ranged from 13% to 135% (mean 64%). The breakdown of the HydroFill coil was 5–116% (mean 41%). Although the calculated filling volume was more than 100% in some aneurysms, those volumes included total circumferential expansion of the hydrogel which does not always happen within the aneurysm sac as the hydrogel is a soft pliable material and does not swell if it comes in contact with a solid surface, such as the aneurysm wall or other coil loops. Aneurysm sizes and calculated packing densities are summarized in table 1.
Aneurysm size and calculated volume fill
Angiographic/MR angiography follow-up observation
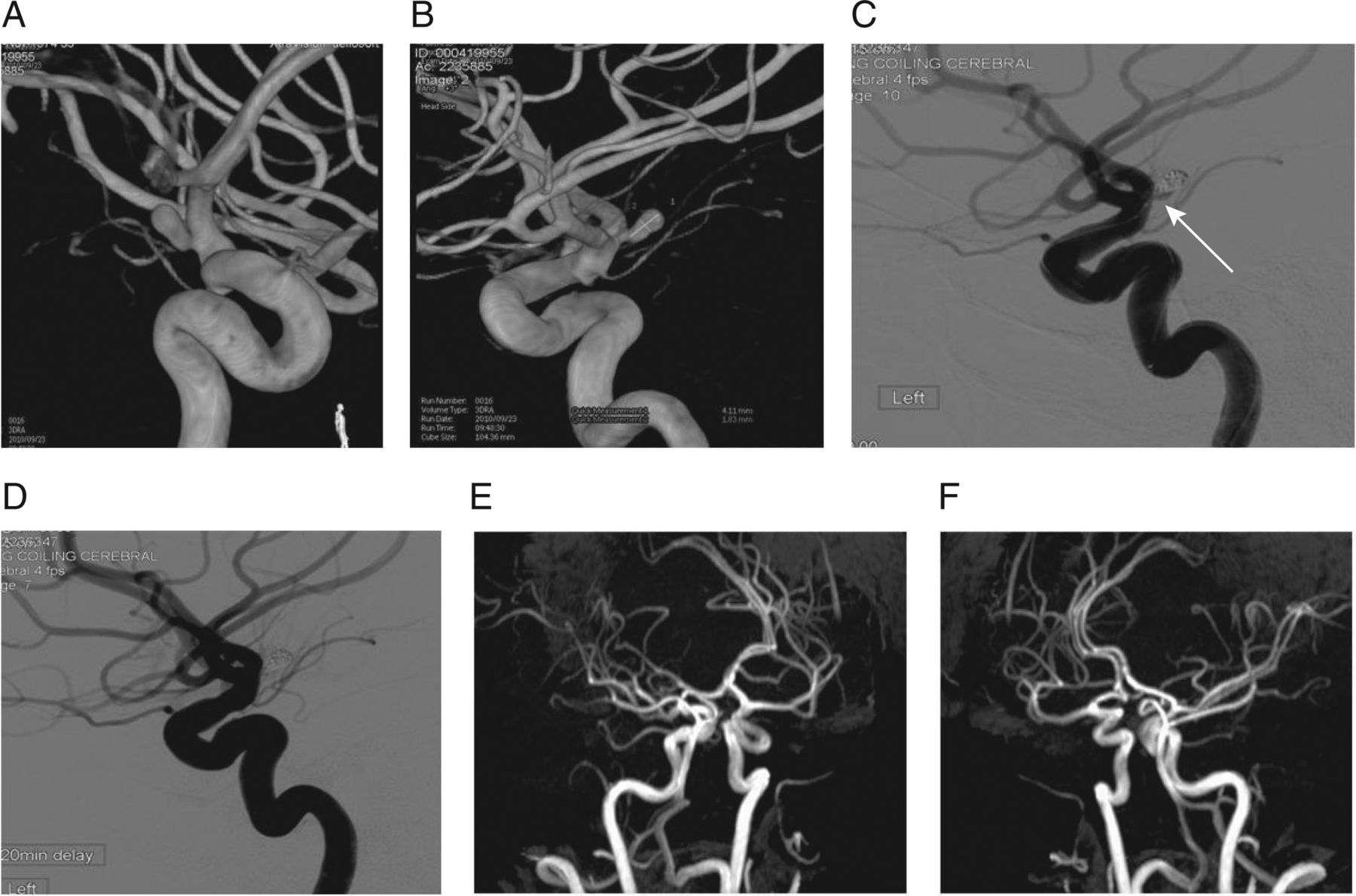
The 13–30 month follow-up imaging (mean 21.7 months) demonstrated that 12/14 (86%) aneurysms were classified as class 1 and remained stable (figure 2). However, 2/14 (14%) converted from class 1 to class 3. One aneurysm (patient No 3, left anterior communicating artery) had a 3 mm neck remnant but was deemed to be stable over the follow-up period and no retreatment was completed. The other aneurysm (patient No 7, cavernous internal carotid artery aneurysm) had a 2–3 mm recanalized segment which was retreated at an outside hospital with a pipeline embolization device (Covidien, Irvine, California, USA).
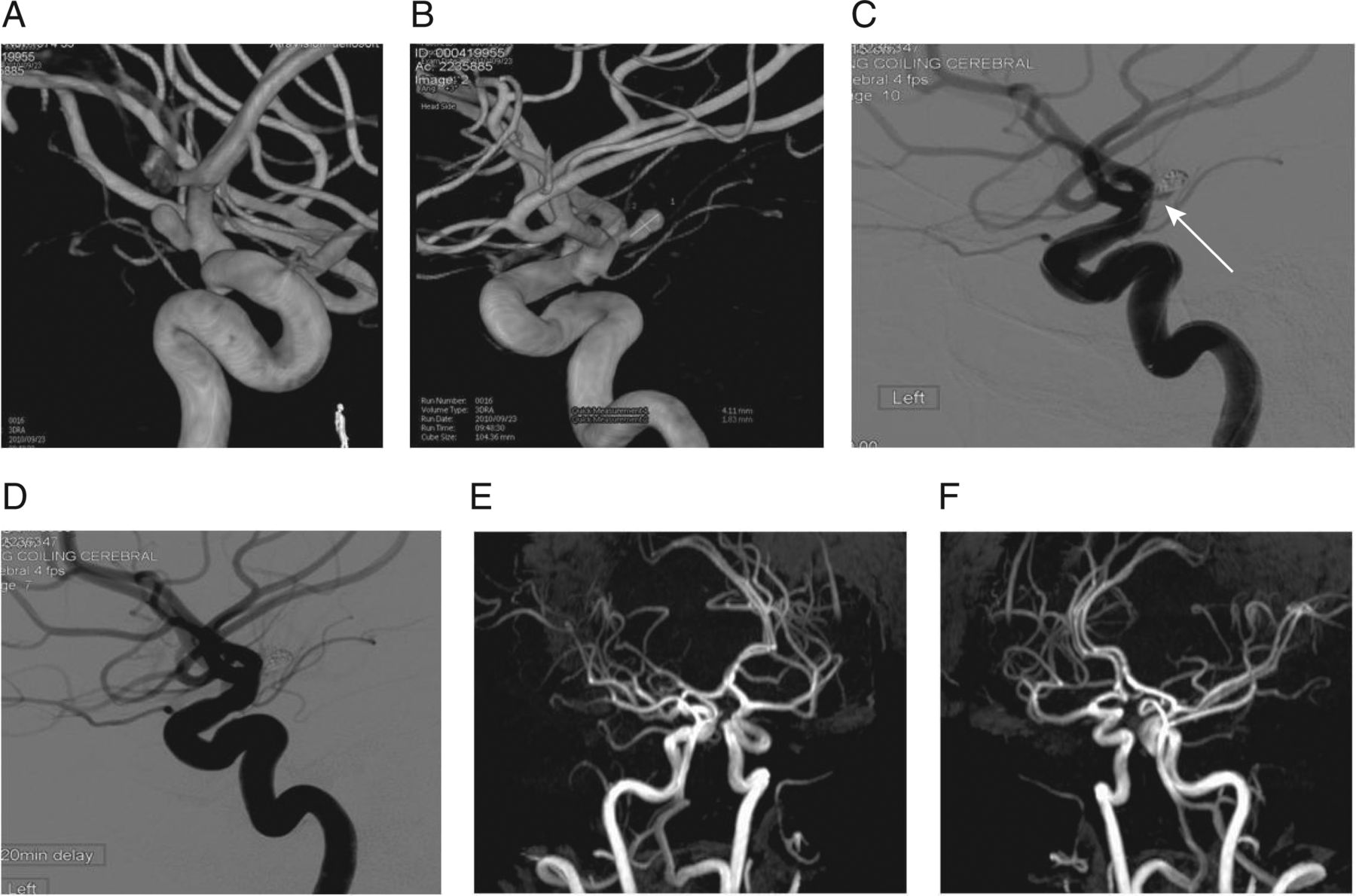
Acute subarachnoid hemorrhage (patient No 9). Left internal carotid angiogram shows a posterior wall A1 segment aneurysm (A, B). Immediate post embolization image (C) demonstrates near complete occlusion with small neck remnant (arrow). Twenty minute delayed control angiogram (D) demonstrates total occlusion of the entire sac. Eighteen month contrast enhanced MR angiography demonstrates continued stable occlusion of the aneurysm sac (E, F).
Complications
All procedure related complications as well as follow-up related morbidity were documented from chart review, clinical evaluation, angiography, and/or CE-MRA. The overall morbidity and mortality in this cohort of patients was 9% (1/11 patients) and 0%, respectively. The single complication in this series (patient No 5) had transient right hemiparesis immediately post coiling secondary to a partial occlusion of the right pericallosal artery along the neck of the previously coiled aneurysm. The occlusion appeared to be a filling defect which was associated with a thrombus on the control angiogram and did not represent swelling of the hydrogel into the parent vessel. All coil loops were contained within the aneurysm sac. The patient received 11.3 mg of eptifibatide (Integrilin) as an intravenous bolus, followed by an infusion of 15 mg/h for a period of 24 h. The patient was also given heparin for 24 h (titrated to maintain an activated partial thromboplastin time of 60–85 s), and was monitored in the intensive care unit overnight. A CT scan 24 h post treatment demonstrated a low density area in the superior frontal gyrus which was suggestive of a small area of ischemic infarct. However, the patient recovered to his presenting neurological baseline and was discharged from the hospital at 36 h post treatment without any neurological sequelae.
There were no other thromboembolic complications seen in this series or during the follow-up period.
Discussion
This is our first initial experience with the next generation HydroFill coil. Although this is a small series utilizing the HydroFill coil, it appears to be safe and effective, either as the primary embolic agent or in conjunction with other embolic coils. The recanalization rate of 2/14 (14%) compares favorably with that of other coils in the HELPS trial,9 which demonstrated 6–12 month follow-up recurrence rates of 27% in the HES arm and 36% in the bare platinum arm.
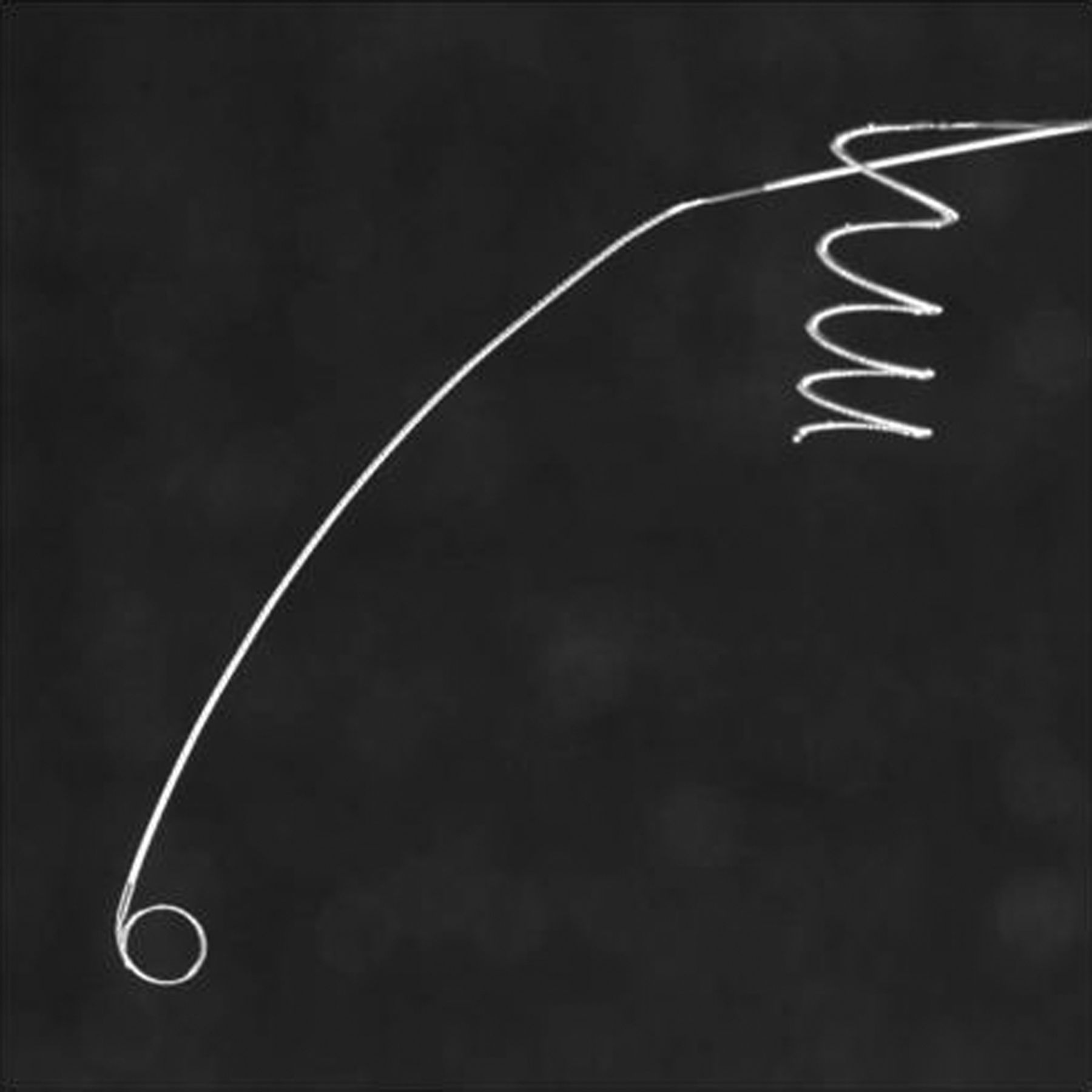
Unlike the pre-existing HydroCoils (HES 10/14/18 coils), which are stiffer and more difficult to deploy, the HydroFill does not require any additional preparation prior to insertion and deployment (figure 3). The HydroFill coil is already pre-softened, and can be inserted and deployed similar to that of a platinum coil. The coil has the manufactured ability to expand from 0.016 to 0.018 inches over a period of 20 min, once exposed to the patient's blood.
{kind=link}
{kind=link}
{kind=link}
Un-prepped HydroCoil Embolization System 10 and HydroFill prior to insertion.
However, the HydroFill coil has a limited repositioning time of 10–30 min, depending on the microcatheter used. The limited repositioning time may be outweighed by the increased volumetric filling within the aneurysm sac, which can lead to more durable treatment with fewer recurrences compared with the use of platinum coils.13 ,16 ,20 Killer et al24 also demonstrated more stable occlusion with neointimal formation utilizing the HydroFill coil, which may lead to a more stable occlusion with a decrease in recurrence rates and retreatments.
Conclusion
Although this initial case series is small, this study demonstrates safe deployment of the HydroFill coil in ruptured and unruptured aneurysms without major complications, and with a high rate of occlusion on long term follow-up. More clinical data should be collected to further validate the results of this series of patients and assess the impact on angiographic/clinical outcome.
Acknowledgments
The authors would like to thank Jackie Massender for data collection, as well as Jack Lossing and Jon Polkinghorne for their assistance with image collection.
Footnotes
-
Contributors JWDS: study design, data collection/analysis, manuscript drafting and review, and guarantor of the study. THB: study design, data analysis, and manuscript drafting and review. SYL: data analysis, and manuscript drafting and review. BDA: data collection/analysis and manuscript review.
-
Competing interests THB is an employee of MicroVention/Terumo.
-
Provenance and peer review Not commissioned; externally peer reviewed.