Article Text

Abstract
Large and giant paraclinoid aneurysms are challenging to treat by either surgical or endovascular means. Visual dysfunction secondary to optic nerve compression and its relationship with aneurysm size, pulsation and thrombosis is poorly understood. We present a patient with a giant paraclinoid aneurysm resulting in bilateral visual loss that worsened following placement of a Pipeline Embolization Device and adjunctive coiling. Visual worsening occurred in conjunction with aneurysm thrombosis, increase in maximal aneurysm diameter and new adjacent edema. Her visual function spontaneously improved in a delayed fashion to better than pre-procedure, in conjunction with reduced aneurysmal mass effect, size and pulsation artifact on MRI. This report documents detailed ophthalmologic and MRI evidence for the role of thrombosis, aneurysm mass effect and aneurysm pulsation as causative etiologies for both cranial nerve dysfunction and delayed resolution following flow diversion treatment of large cerebral aneurysms.
- Aneurysm
- MRI
- Flow Diverter
Statistics from Altmetric.com
Background
There have been few case reports describing the pathophysiology of compressive cranial neuropathies following flow diversion of cerebral aneurysms. We present a case of particular interest to neurointerventionists because it details several key phenomena that occurred after treatment with a Pipeline Embolization Device (PED; ev3-Covidien, Mansfield, Massachusetts, USA) of a giant paraclinoid aneurysm: (1) progressive increase in aneurysm size due to thrombosis, resulting in worsening optic nerve compression and visual function associated with an increase in adjacent cerebral edema; (2) reduction in aneurysm pulsations after treatment based on MRI findings; (3) progressive improvement in bilateral vision with resolution of pulsation artifact, reduction in aneurysm size and resolution of cerebral edema. Furthermore, this case report is enhanced by the inclusion of detailed ophthalmologic examinations and MRI.
Case presentation
A woman in her sixties presented with progressive left visual field loss with a presumed diagnosis of glaucoma. She was neurologically intact on examination except for 20/30 vision in the right eye and could only count fingers in the left eye.
Investigations
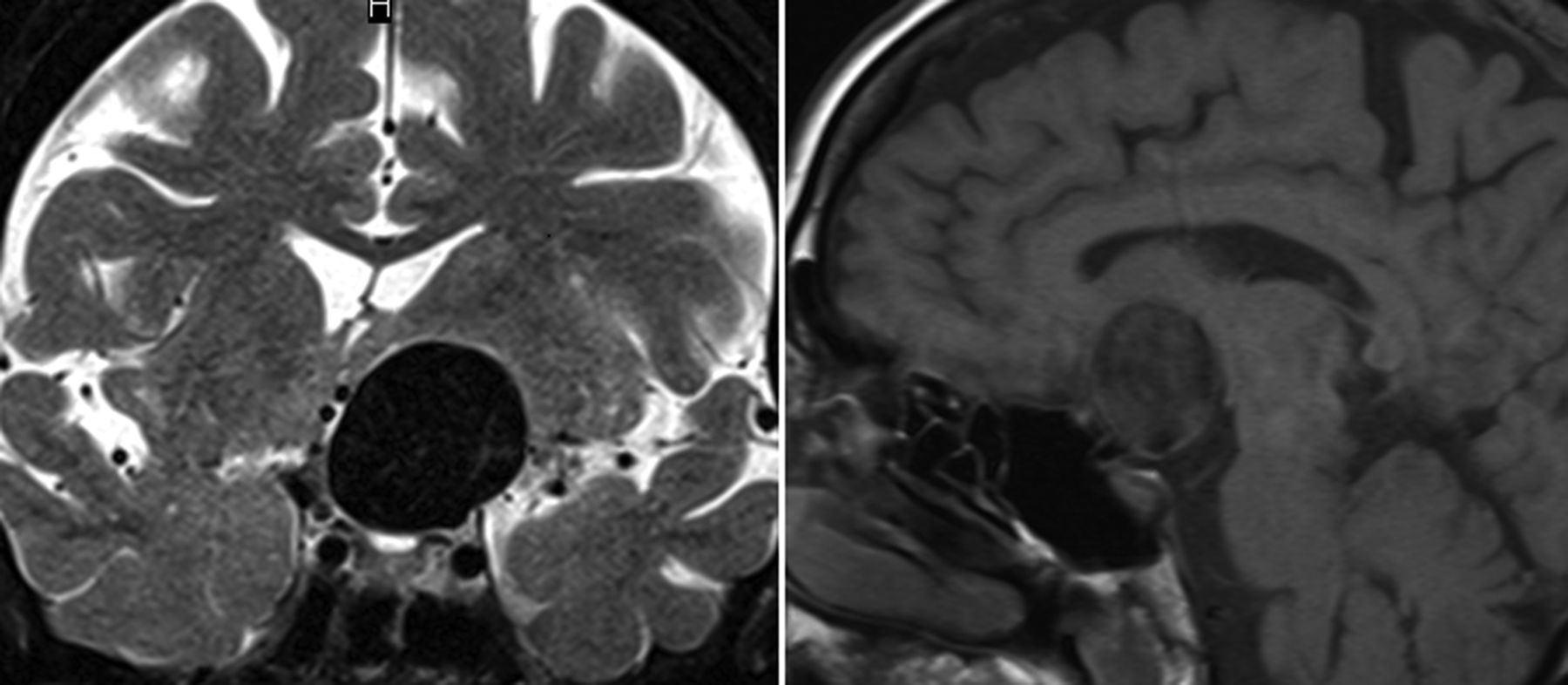
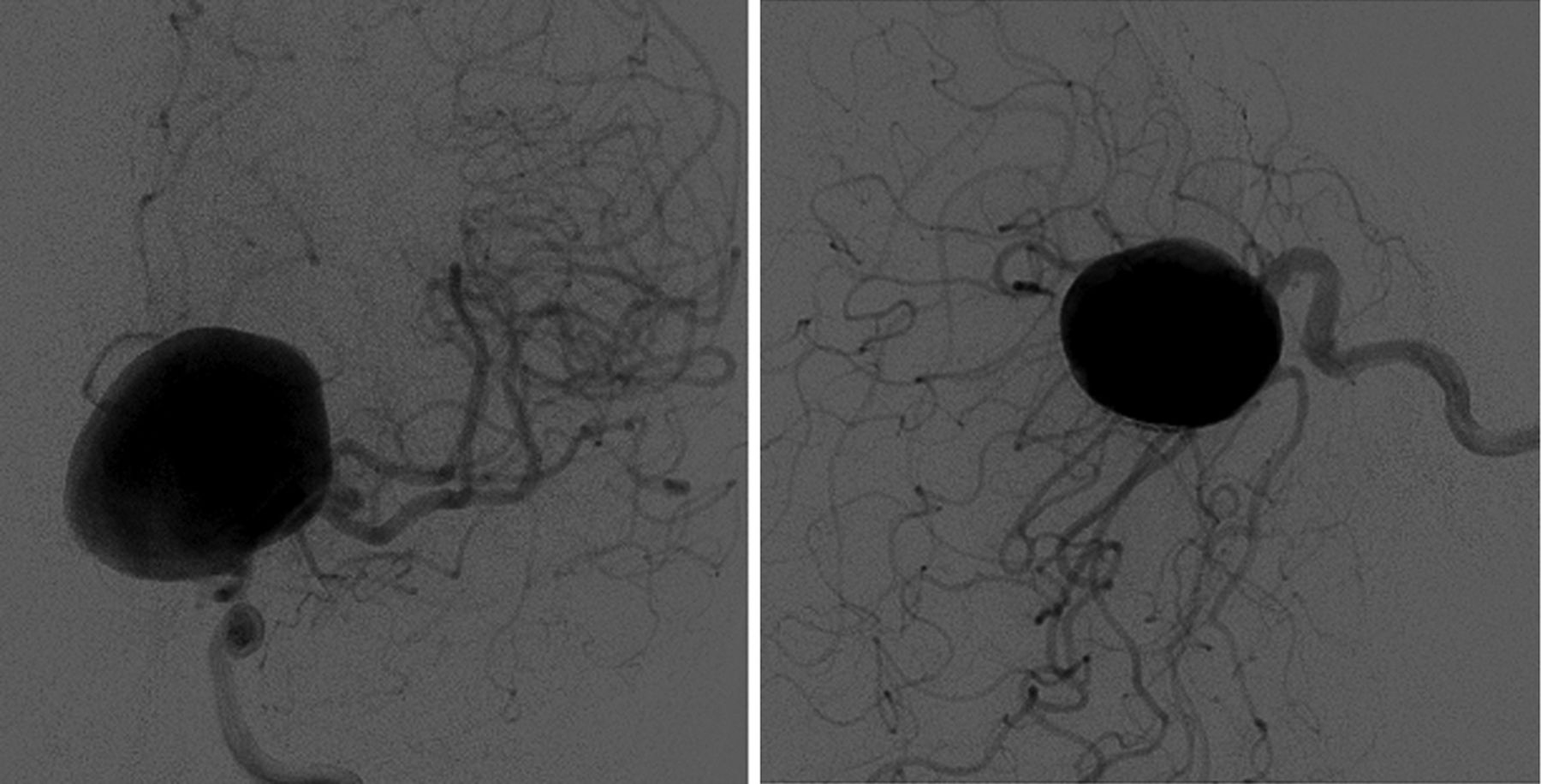
MRI of the brain demonstrated a giant left ophthalmic aneurysm resulting in significant mass effect on the left frontal lobe with pulsation artifact (figure 1). Digital subtraction angiography (DSA) showed a 3.0×2.2×2.3 cm aneurysm arising from the dorsal ophthalmic segment of the internal carotid artery (figure 2). The aneurysm neck was 15.4 mm. A second smaller M1 bifurcation aneurysm was also identified on DSA.

MRI of the brain on presentation. A giant internal carotid artery aneurysm is seen on T2-weighted coronal (left panel) and T1-weighted sagittal (right panel) sequences.
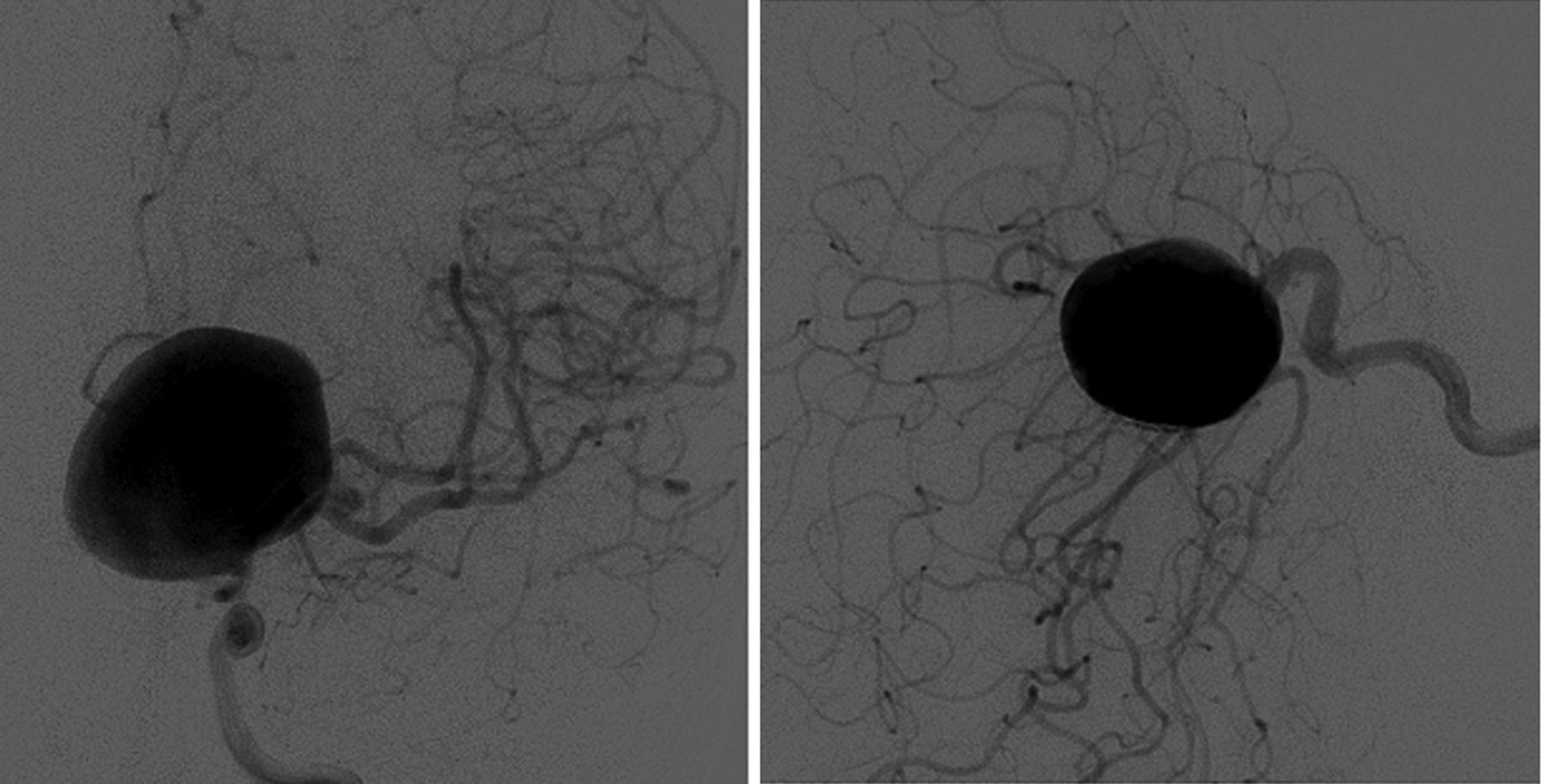
Anteroposterior (left panel) and lateral (right panel) digital subtraction angiograms demonstrating the giant internal carotid artery aneurysm.
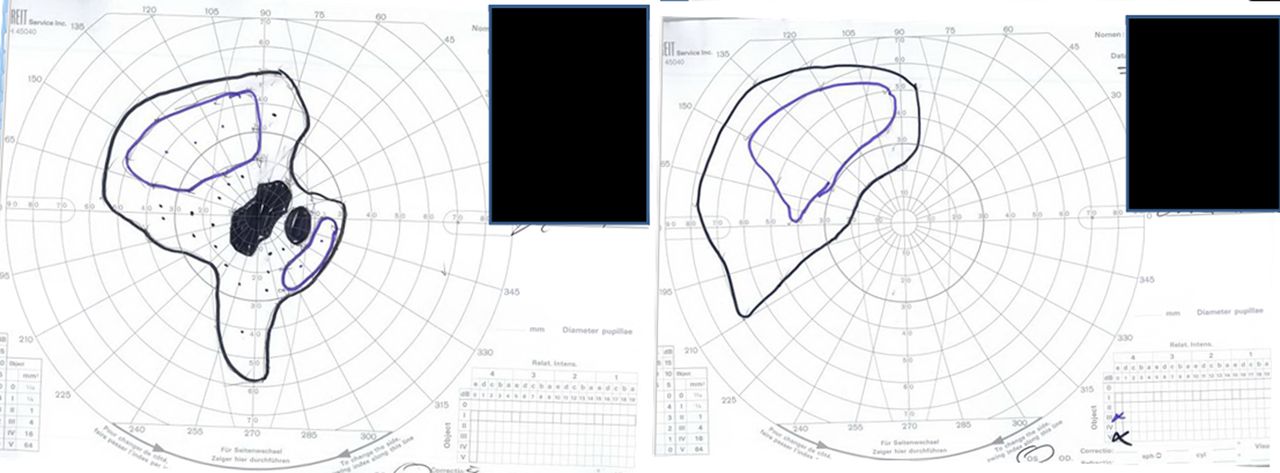
A detailed ophthalmologic evaluation was performed which showed normal intraocular pressures and a left afferent pupillary defect (APD). The fundus examination showed large tilted optic disks with peripapillary atrophy. Optical coherence tomography showed subtle thinning of the nerve fibers superiorly in both eyes (figure 3). Goldmann visual field (GVF) examination showed a junctional scotoma pattern with right upper quadrant loss in the right eye and central scotoma in the left eye, indicative of pressure on the juncture between the left optic nerve and optic chiasm (figure 4).

Optical coherence tomography showing subtle thinning of the nerve fibers superiorly in both eyes.
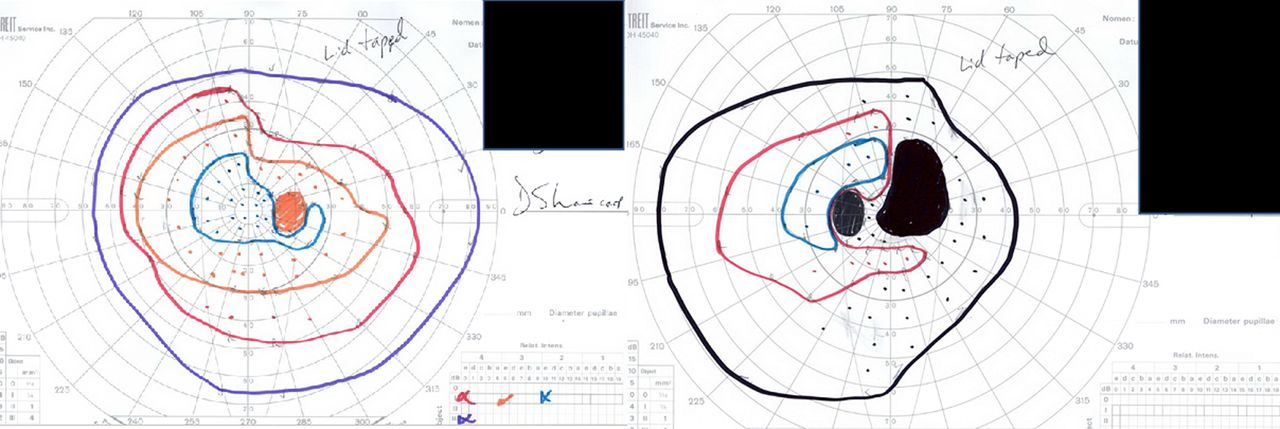
Goldmann visual field examination demonstrating a junctional scotoma pattern with right upper quadrant loss in the right eye and central scotoma in the left eye, indicative of pressure on the juncture between the left optic nerve and optic chiasm.
Treatment
Endovascular embolization was offered using a combined approach of flow diversion with adjunctive coil embolization. The patient underwent uncomplicated PED deployment across the neck of the aneurysm with a 4.5×30 mm PED followed by coil embolization of the aneurysm. A microcatheter was jailed in the aneurysm, the PED was deployed across the neck of the aneurysm and then 10 bare platinum coils were deployed inside the lumen of the aneurysm. The procedure was uncomplicated (figure 5).
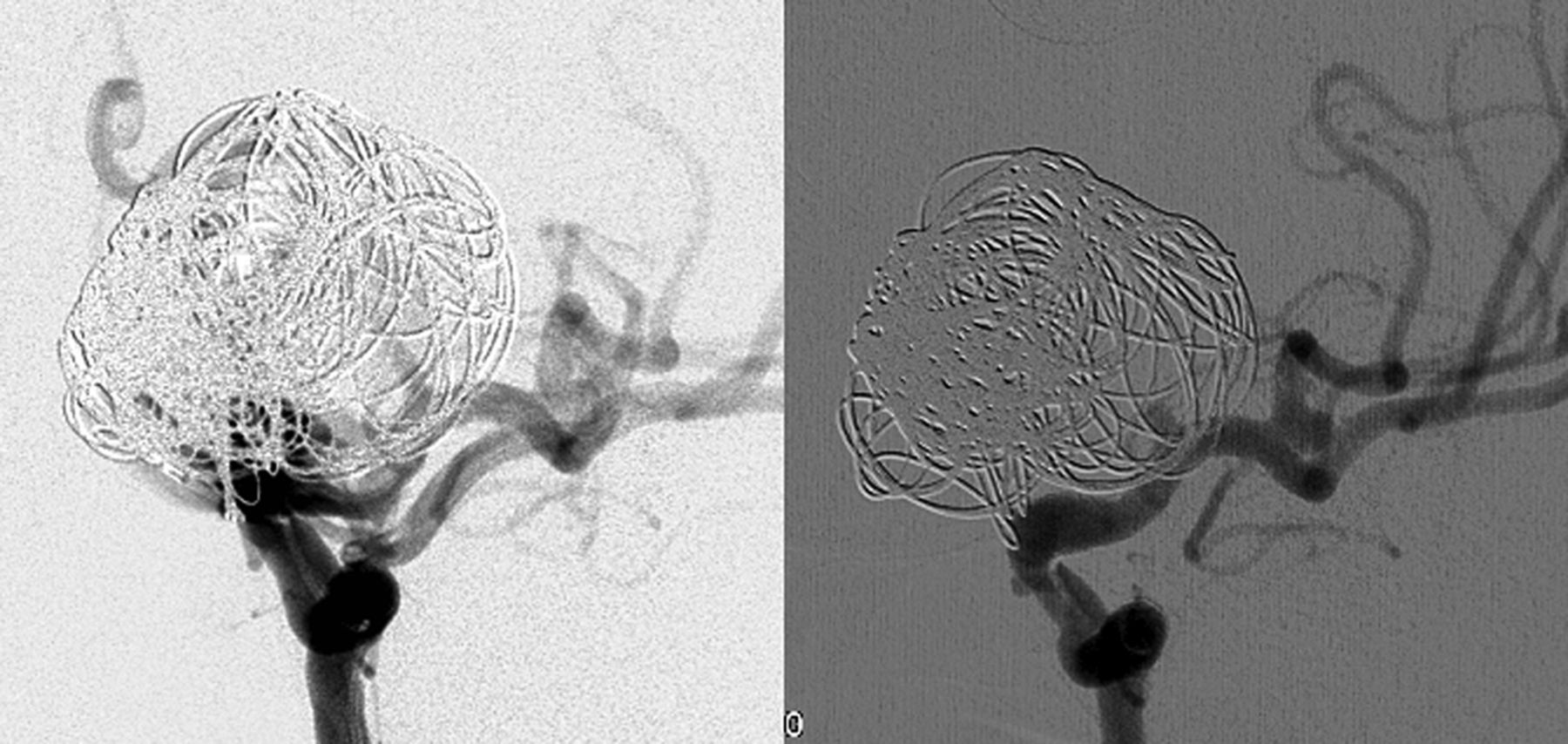
Final oblique angiographic injection (right panel) after deployment of the Pipeline Embolization Device and adjunctive coiling and 6-month follow-up angiogram (left panel) showing complete aneurysm occlusion.
Outcome and follow-up
Immediately after the procedure the patient reported decreased vision in both eyes compared with her preoperative visual function. Dexamethasone therapy was initiated but her vision continued to deteriorate. Three months after the procedure she subjectively reported only seeing shapes and light in both eyes. On formal examination she was counting fingers at 60 cm in the right eye and 30 cm in the left eye. She demonstrated a left APD with stable nerve fiber layers (NFL) since the previous visit. The GVF showed a limited small visual field island in the upper temporal field for the left eye and central scotoma with a limited visual field island to the nasal field for the right eye (figure 6).

Post-procedure Goldmann visual field examination demonstrating a limited small visual field island in the upper temporal field for the left eye and central scotoma with a limited visual field island to the nasal field for the right eye.
Repeat MRI demonstrated an increase in aneurysm size with a circumferential increase in the maximal transverse diameter to 35 mm compared with 30 mm at baseline. Internally, the appearance of the aneurysm was consistent with thrombosis and the extensive pulsation artifact present on the baseline examination had resolved. The visual apparatus was slightly more obscured by the aneurysm enlargement and mild surrounding edema and there was persistent marked compression and displacement.
The patient returned 6 months after her procedure with further visual deterioration. Ophthalmologic examination showed further worsening of her visual acuity to hand motion perception only in both eyes. Due to the progressive visual worsening, craniotomy for aneurysm resection and optic nerve decompression was discussed with the patient, but the patient elected to forego additional surgery due to concerns over potential complications associated with open surgical intervention.
Eight months after surgery the patient noted partial visual improvement in the right eye with an improved visual acuity to 20/60. Furthermore, stability of NFL was noted as well as a significantly improved GVF.
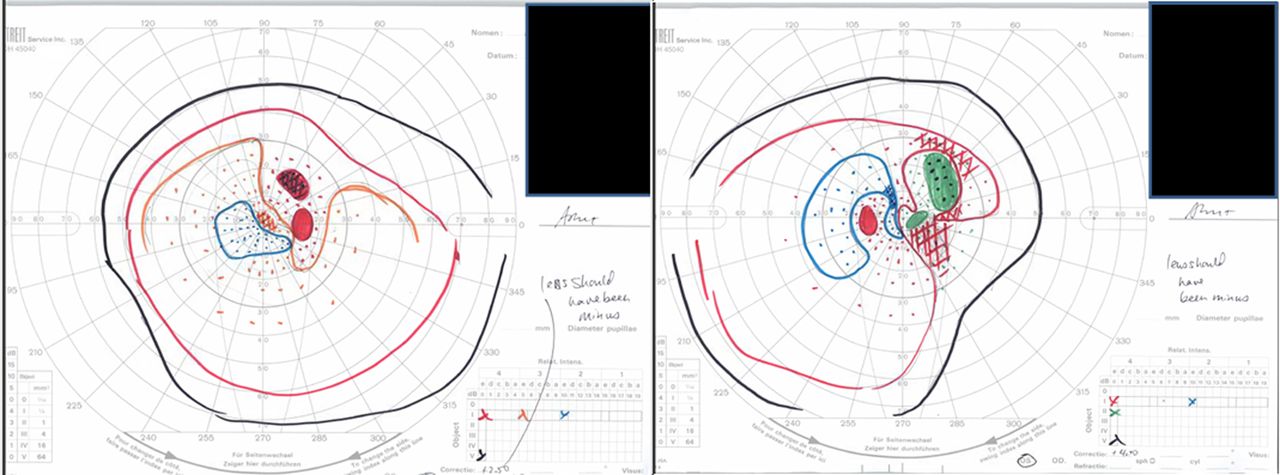
Fifteen months after her embolization procedure the patient returned with marked subjective visual improvement in both eyes. The examination showed best corrected vision of 20/20 in the right eye and 20/40 in the left eye. She recovered to full color vision in the right eye but no color vision in the left eye. She had no APD. The GVF showed marked expansion in both eyes (figure 7). An MRI of the brain was repeated and showed internal thrombosis with a decrease in aneurysm volume to baseline size and absence of pulsations. There was persistent mass effect on the optic apparatus, but this was decreased from the initial follow-up examination (figures 8 and 9).

Goldmann visual field examination at 15 months post-procedure demonstrating marked improvement in both eyes.

MRI of the brain with T2 coronal imaging before the intervention (left panel), at 5 months (center panel) and at 15 months (right panel) after the procedure. The baseline examination demonstrates complete flow void due to the high flow state within the aneurysm. There is no surrounding brain edema. The 5-month follow-up examination shows aneurysm enlargement, internal signal inhomogeneity consistent with developing thrombosis and new edema within the deep white matter. The 15-month follow-up examination shows an overall decrease in aneurysm size, more complete internal thrombosis and resolution of edema within the deep white matter.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MRI demonstrating resolution of phase encoding pulsation artifact after treatment. Left panel: T1 axial baseline image demonstrating the marked phase encoding pulsation artifact due to turbulent flow in the giant aneurysm. Right panel: the image obtained at delayed follow-up shows near complete resolution of the phase encoding pulsation artifact following endovascular treatment.
Discussion
While improvements in microneurosurgical and endovascular techniques have reduced the morbidity and mortality associated with treatment of large or giant ophthalmic aneurysms, the incidence of visual complications with either treatment is estimated at approximately 2–15%.1–6 Patients with large or giant aneurysms and significant visual loss preoperatively often demonstrate little improvement even after successful treatment.7
This case demonstrates several interesting phenomena. First, progressive aneurysmal thrombosis after flow diversion and adjunctive coiling was seen leading to further optic apparatus compromise from mass effect and edema, followed by delayed reduction in mass effect over time with elimination of pulsations. While progressive aneurysm thrombosis and increasing mass effect after flow diversion have been reported previously,8 this case clearly illustrates this phenomenon and the potential for further neurologic deterioration after aneurysm thrombosis. In many cases, compressive cranial neuropathies improve after endovascular treatment, even though the aneurysm volume has not been reduced. However, there are also case reports describing the development of new cranial neuropathies following embolization of cerebral aneurysms.9 ,10 Increasing aneurysmal volume following treatment, leading to symptomatic cranial nerve compression, may be secondary to either progressive aneurysm thrombosis, as suggested by this case, or rarely from increasing mass effect due to inflammation or hematoma secondary to persistent vaso vasorum.10 While it is possible that continued contrast stasis seen within the aneurysm after PED deployment may be a potential risk factor for delayed aneurysm rupture, the relationship between persistent stasis and the rate of (or final volume after) aneurysm thrombosis is unclear.
Second, there are relatively few reports demonstrating bilateral vision loss after flow diversion embolization of aneurysms. The contralateral vision loss after treatment is evidence that there was an actual increase in aneurysm volume and mass effect after flow diversion, a controversial point which has not previously been proven. This was demonstrated by MRI to be due to increased aneurysm volume with mass effect and associated edema on the optic chiasm. The coils were placed into the aneurysm dome with the intention of expediting aneurysm thrombosis to prevent subarachnoid hemorrhage and improve mass effect. It is unclear if the use of coils in conjunction with the PED either hastened or exacerbated thrombosis. There is little published data to support or refute the use of coils in this setting.
Third, this is one of relatively few reports of a patient who had bilateral vision loss after flow diversion with delayed return of vision to better than pre-procedure. On MRI, this was associated with a progressive decrease in aneurysm volume with a decrease in mass effect and edema on the optic chiasm, as well as elimination of aneurysm pulsations.
Fourth, we are fortunate that this is one of relatively few reports to include MRI documentation at several stages of the patient's course (pre-procedure, post-procedure, delayed follow-up), which better defines the pathophysiology by which giant aneurysms cause vision loss. The initial MRI examination showed the overall direct mass effect of the aneurysm on the optic apparatus as well as pulsation artifact, which are probably the primary pathophysiologies producing the vision loss. The progressive swelling of the aneurysm initially after treatment is the most likely cause of the continued visual decline, as there was circumferential enlargement of the aneurysm and near complete obscuration of the optic apparatus on MRI initially following treatment. However, at the 15-month post-treatment examination the aneurysm had a similar size to the baseline presentation, suggesting that additional secondary factors were involved. Additional factors which have been suggested and are likely etiologies in this case are the pulsations of the aneurysm against the nerve and the mild post-treatment surrounding edema, both of which can exacerbate the compressive effects. Return of vision at follow-up was associated with the demonstration by MRI of decreasing mass effect and compression, reduction in aneurysm pulsations and resolution of perianeurysmal edema. These pathophysiologic mechanisms may be applicable to periprocedural sequelae relating to other cranial nerves, not just to the optic nerves.
Key messages
-
Treatment of giant paraclinoid aneurysms with flow diversion technology may result in aneurysm thrombosis and expansion, resulting in worsening cerebral edema and neural compression.
-
Reduction in arterial pulsations and reduction in aneurysm size after treatment may lead to delayed improvement in visual symptoms.
-
Even severe visual loss secondary to compression of the optic apparatus may improve once compression is removed.
References
Footnotes
-
Republished with permission from BMJ Case Reports Published 10 January 2014; doi:10.1136/bcr-2013-010960
-
Contributors All authors made substantial contributions to conception and design, analysis and interpretation of data; drafted or critically revised the article; and gave final approval of the version to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.