Article Text

Abstract
Ehlers–Danlos syndrome (EDS) type IV is a collagen vascular disease with an autosomal dominant inheritance caused by COL3A1 mutation. Patients with EDS type IV can present with organ rupture, spontaneous arterial dissections and ruptured aneurysms. Because of their propensity to form arterial dissections, aneurysms and rupture, they can develop carotid–cavernous fistula (CCF) after minor trauma or spontaneously. In EDS, it has been reported that even conventional catheter diagnostic angiography may result in large artery dissections and vessel rupture. In addition, the treatment of CCF in EDS type IV can result in up to 59% mortality after initial treatment, of which 23% is attributed to direct complications of treatment. We present the case of a patient with EDS type IV who previously had spontaneous dissection and multiple pseudoaneurysms of both the iliac and femoral arteries and the distal abdominal aorta. Several years later the patient developed a direct type A CCF which was successfully treated with endovascular embolization using a transvenous approach with detachable coils. The literature pertaining to CCF in EDS type IV and its treatment is reviewed.
- Angiography
- Coil
- Dissection
- Fistula
- Vein
Statistics from Altmetric.com
Background
The term cutis hyperlastica or Ehlers–Danlos syndrome (EDS) is given to a group of inherited connective tissue disorders caused by a defect in the synthesis of collagen (type I, III or IV) with a prevalence of 1 in 10 000. In particular, EDS type IV is a collagen vascular disease with an autosomal dominant inheritance caused by a COL3A1 mutation that occurs in 5–10% of patients with EDS. Patients with EDS type IV (EDS IV) can present with arterial dissection, ruptured aneurysms, gastrointestinal perforation or organ rupture. Clinically, these patients appear with joint hypermobility, thin translucent skin, easy bruising and, in some individuals, a typical facial appearance. Arterial dissections leading to the formation of aneurysms and arteriovenous fistulae can be secondary to minor trauma but may also occur spontaneously.
Carotid cavernous fistulae (CCFs) are secondary to the formation of a shunt between the internal carotid artery (ICA) or external carotid artery (ECA) and the cavernous sinus. Barrow et al in 1985 proposed an angiographic classification of CCF as direct (type A) and indirect (type B–D). Direct type A CCF can occur as a result of trauma or by a ruptured carotid cavernous aneurysm.1
Because of their propensity to form arterial dissections, aneurysms and rupture, patients with EDS IV can develop CCF after minor trauma or spontaneously. The treatment of CCF in patients with EDS IV is particularly challenging. In fact, in these patients even conventional catheter diagnostic angiography may result in large artery dissections and vessel rupture.2 In addition, the treatment of CCF in EDS IV can result in up to 59% mortality after initial treatment, of which 23% is attributed to direct treatment complications.2 A recent case series of patients with symptomatic CCF reported post-treatment mortality of 4%.3
Case presentation
At an early age the patient developed spontaneous dissection and multiple pseudoaneurysms of both iliac arteries, femoral arteries, the distal abdominal aorta and left subclavian artery (figure 1). The patient was diagnosed with EDS. Because of the risk of treatment in EDS, all the lesions involving the iliac and abdominal aorta were followed conservatively. Several years later the patient developed subacute onset of severe headaches, right auditory bruit, blurred vision in the right eye with conjunctival irritation and retro-orbital pain, and slight worsening of his acuity to 20/60.

CT angiography of the abdomen and pelvis showing the dissections with pseudoaneurysms of bilateral iliac, bilateral femoral and right renal arteries.
Investigations
Head MRI and MR angiography (MRA) showed enlarged venous structures consistent with a diagnosis of CCF.
On general clinical examination the patient had all the features of EDS IV. He had short stature, hypermobile joints and hyperelastic skin and also had soft friable blond hair. Ophthalmologic evaluation showed right eye proptosis with limbal injection and retinal edema on funduscopic examination. He had marked congestion of the superficial frontal and temporal veins, mostly on the right side. A loud retro-orbital bruit synchronous with the patient's pulse was clearly audible on auscultation. The bruit decreased in intensity with compression of the right carotid artery in the neck. He had mild diplopia on extreme horizontal right gaze, suggestive of a partial right VI cranial nerve palsy. The rest of his neurological examination was otherwise unremarkable. Head and neck CT angiography (CTA) showed a right CCF (figure 2).
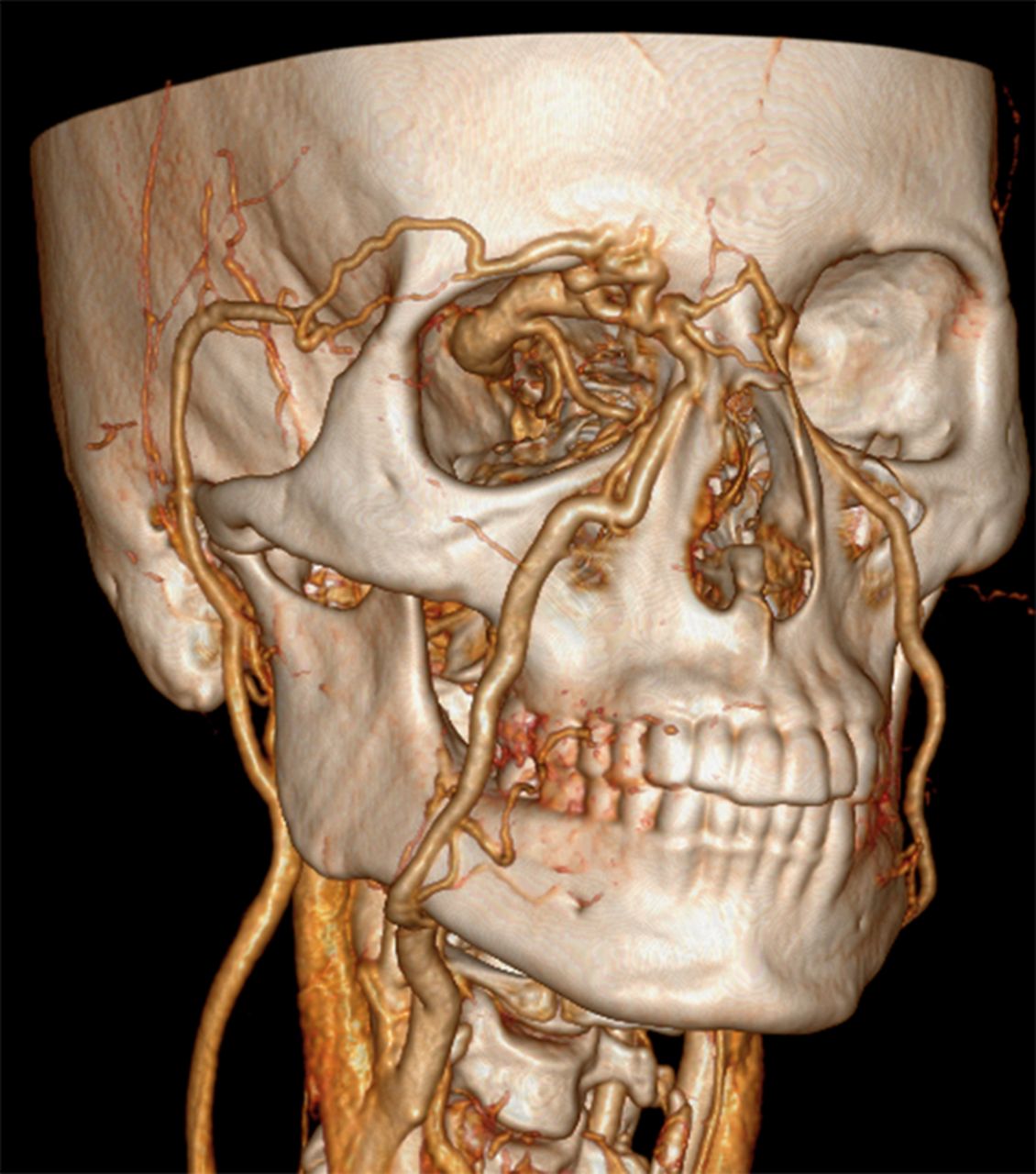
CT angiography of the head showing the direct carotid cavernous fistula from the right internal carotid artery into the cavernous sinus.
Treatment
The procedure was performed under general anesthesia. Because of the spontaneous dissection with several pseudoaneurysm formations of both iliac arteries and the abdominal aorta, alternative access such as the radial and brachial arteries was considered. However, because of the risk of dissection of these arteries as well, it was decided to attempt access via the femoral artery. Angiography from the right ICA was planned in order to map the venous anatomy for navigation, positioning and embolization of the CCF. Careful ultrasonographic and continuous fluoroscopic guidance was performed in order to ensure access to the true lumen of the dissected right femoral artery. In order to decrease the amount of trauma to the artery accessed for navigation, a 4 F 24 cm sheath was inserted into the right femoral arty and a 6 F sheath was then inserted into the left femoral vein, also under ultrasound guidance.
A 4 F Terumo glide catheter (Terumo, New Jersey, USA) with the aid of a Terumo glidewire was then used to access the right common carotid artery. Diagnostic cerebral angiography from the right common carotid artery confirmed the presence of a direct CCF. There was prominent arteriovenous shunting which led to direct opacification of the cavernous sinus, the superior ophthalmic veins (SOVs), inferior and superior petrosal sinuses with retrograde filling of several cortical cerebral veins. Because of the large direct arteriovenous shunt, there was no opacification of the right middle and anterior cerebral artery from the right ICA injection (figure 3).

Right internal carotid artery angiograms showing the high flow shunt into both cavernous sinuses. There was no opacification of the supraclinoid section of the right internal carotid artery or of the right middle cerebral artery.
A 6 F Envoy (Codman, Massachusetts, USA) was then carefully navigated via the 6 F sheath from the left femoral vein and positioned in the right internal jugular vein.
Angiograms were obtained from the right common carotid artery to minimize the intraprocedural risk of dissection and were used as roadmap guidance. From the right jugular vein, an Echelon 10 microcatheter (Covidien, Massachusetts, USA) was carefully advanced into the cavernous sinus via the inferior petrosal vein. Multiple detachable coils were then used to successfully occlude the right SOV and cavernous sinus bilaterally.
Outcome and follow-up
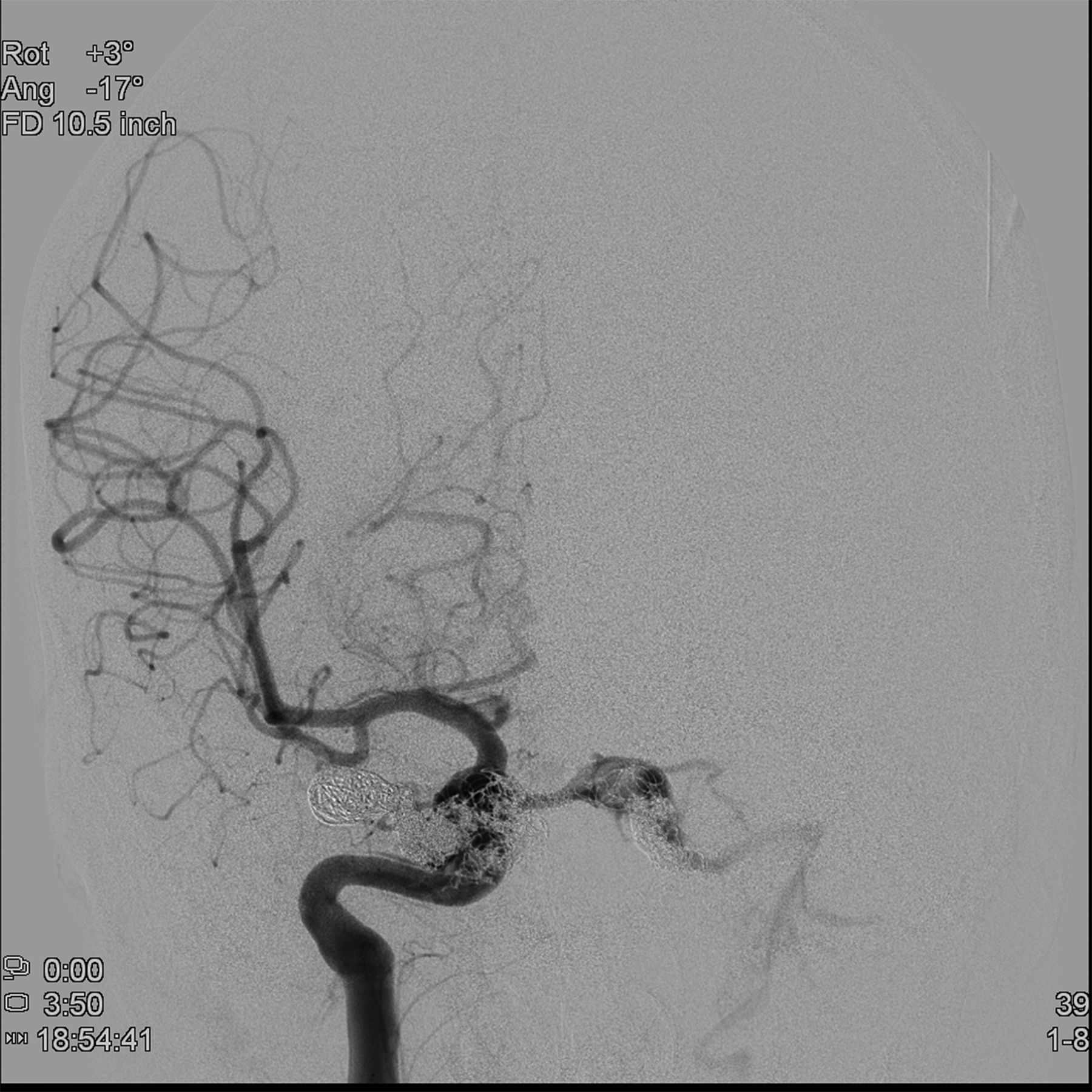
Follow-up angiography demonstrated significant reduction of the CCF with no evidence of early venous drainage through the right SOV. In addition, there was normal opacification of the distal right internal, middle and anterior cerebral arteries (figures 4 and 5). A small amount of very sluggish flow was, however, still visible from the right ICA into the contralateral sinus. At the end of the procedure the loud bruit over the right eye was no longer audible. The patient tolerated the procedure well and was admitted to the intensive care unit overnight. There was reduced conjunctival injection the following day and he was discharged home 2 days later. Clinically, he had complete resolution of the headaches after completing a 1-week course of a tapering dose of methylprednisolone. The patient went back to work full-time and, at the 1-month clinical follow-up evaluation, there was no evidence of right eye proptosis, injected conjunctiva or auditory bruits.The 3-month follow-up CTA did not show evidence of a CCF or of dilated periorbital veins. The patient has been back at work full-time since the procedure and remained asymptomatic at the last clinical evaluation performed 11 months after the procedure. Although it would have been optimal to document occlusion of the CCF by conventional catheter angiography, because of the risk of arterial dissections we did not perform this study on follow-up. The patient is also currently followed clinically with serial imaging to evaluate the eventual progression of the iliac and femoral pseudoaneurysms.
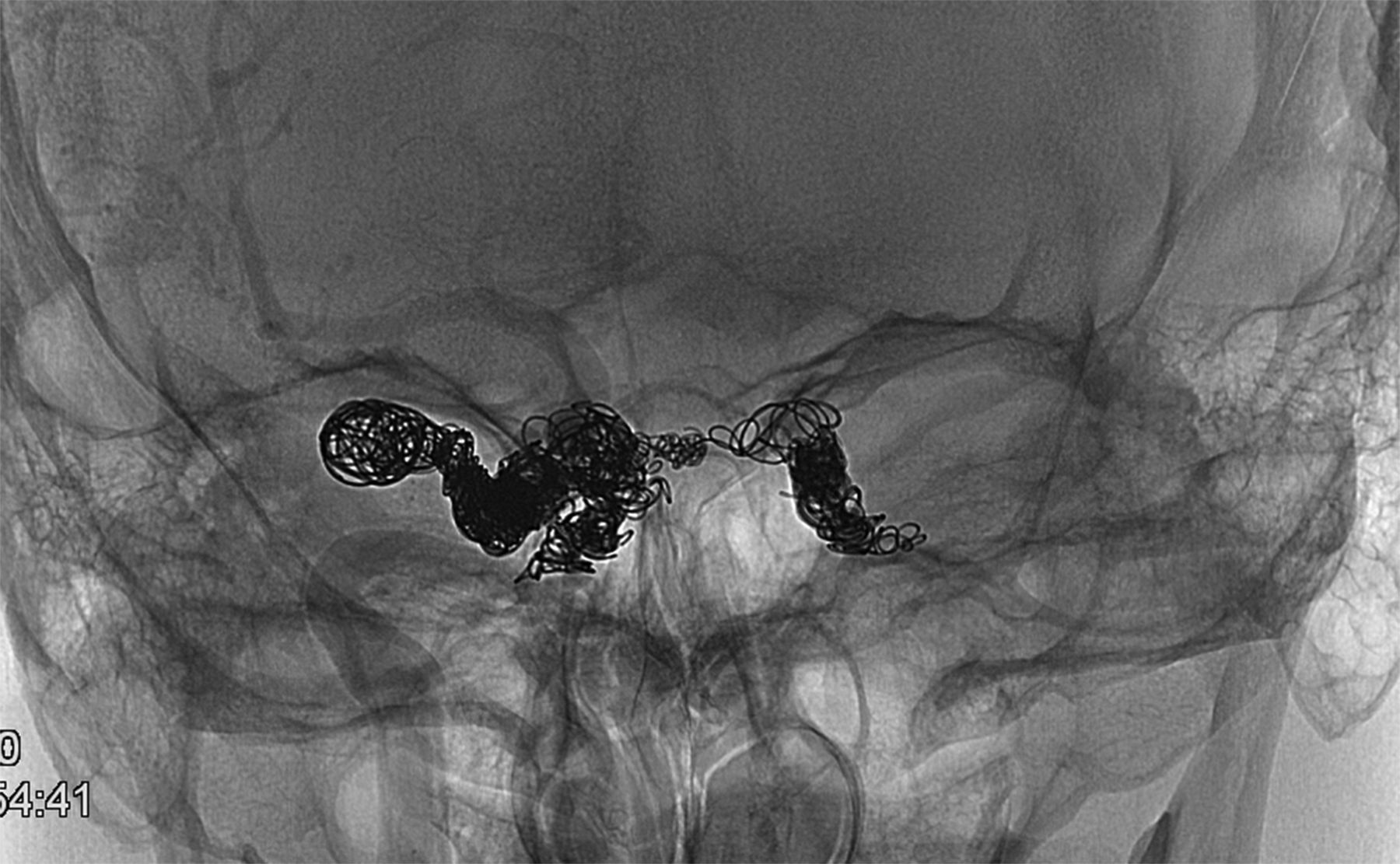
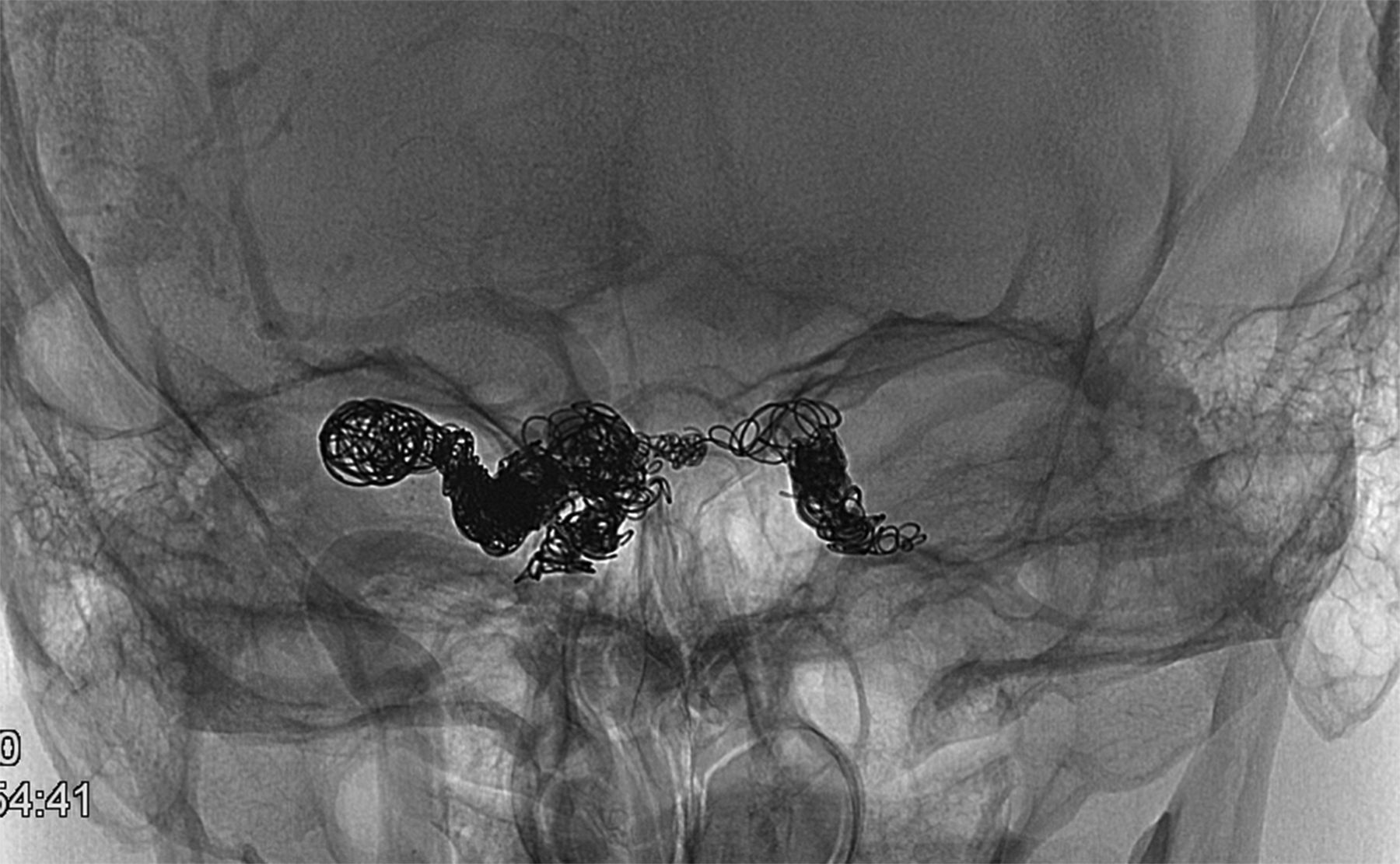
Final (unsubtracted) view of the right internal carotid artery angiogram showing the coil mass in both cavernous sinuses.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
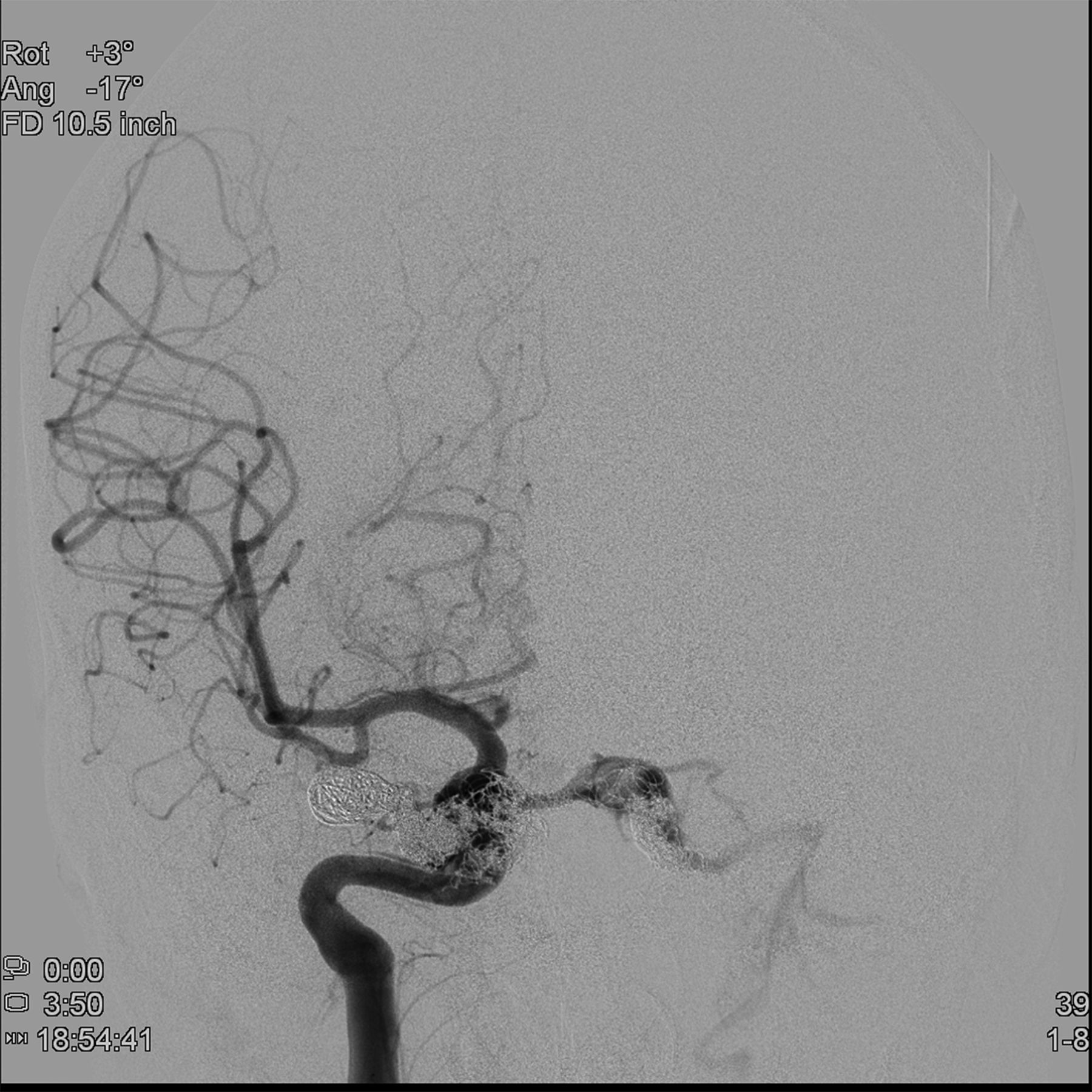
Final anteroposterior view of the right internal carotid artery angiogram. There was normal opacification of the supraclinoid internal carotid artery (ICA) and right middle cerebral artery but a small amount of very sluggish flow was still visible from the right ICA into the contralateral sinus.
Discussion
CCFs are arteriovenous shunts between the ICA or ECA system and the cavernous sinus. In a direct (type A) CCF, connections form between the ICA and the cavernous sinus while, in an indirect CCF (type B–D), the connections are more common between the cavernous sinus and branches of the ICA, ECA or both. These lesions were classified by Barrow et al in 1985.2 Patients with direct CCF often present dramatically with exophthalmos (proptosis), chemosis, pain, opthalmoplegia and bruits. Patients with indirect fistulae may present with mild symptoms.
Multiple etiologies are implicated in direct CCF, including basilar skull fracture or blunt force trauma.4 In contrast, spontaneous causes include rupture of an ICA cavernous aneurysm. In collagen tissue disorders such as EDS IV, fibromuscular dysplasia and pseudoxanthoma elasticum, the proposed mechanism is a spontaneous dissection of the ICA with pseudoaneurysm formation.5 While spontaneous direct CCFs usually have numerous microfistulae and multiple dural feeders, these features are associated with indirect lesions.6 Patients with EDS IV in particular have a unique clinical and genetic predisposition to the formation of arteriovenous fistulae. They may develop multiple aneurysms and arterial dissections in multiple arteries. When they develop spontaneous CCFs, they often present with exophthalmos, chemosis, pain, opthalmoplegia and bruits. These symptoms occur as a result of high flow CCFs which allow pressurized arterial blood to connect directly to the cavernous sinus resulting in venous hypertension and reversal of venous drainage of the superior petrosal sinus, SOV, sphenoparietal sinus and pterygoid plexus they often present with exophthalmos, chemosis, pain, opthalmoplegia and bruits. These symptoms occur as a result of high flow CCFs which allow pressurized arterial blood to connect directly to the cavernous sinus resulting in venous hypertension and reversal of venous drainage of the superior petrosal sinus, SOV, sphenoparietal sinus and pterygoid plexus.7
Diagnosis of CCF includes non-invasive imaging such as CTA and MRA. Common findings on CT and CTA include dilation and tortuosity of the SOV, proptosis of the affected eye and enlargement of the ipsilateral cavernous sinus. MRI can also provide additional details including abnormal flow voids in the cavernous sinus and orbital edema.6 However, conventional catheter angiography remains the gold standard for definitive diagnosis and planning of the treatment of CCFs. This allows determination of direct and indirect lesions, location, size, presence of steal phenomena and identification of high-risk features including cortical venous drainage. While low-flow CCF (mostly type B–D) can be managed conservatively, those with high-flow features should be considered for emergency treatment. These features result in an increased risk of morbidity and mortality and include retrograde venous drainage to the cortical veins, thrombosis of other venous outflow pathways and the presence of a pseudoaneurysm. These are associated with clinical signs and symptoms of rapidly increasing proptosis, change in visual acuity, intracranial hemorrhage and ischemia.
Endovascular approaches to treating CCFs include transarterial or transvenous obliteration of the ipsilateral cavernous sinus with embolic materials or coils, detachable balloon or sacrifice of the ICA. Owing to multiple complications from a transarterial approach, transvenous approaches were considered initially but were not successful. Improved tools and techniques later became available including liquid embolic agents (n-butyl cyanoacrylate (nBCA), ethylene-vinyl alcohol copolymer)7 and the introduction of detachable coils.
The increased use of detachable coils has made a transvenous approach more successful and preferred over surgical techniques such as trapping. The transvenous approach is the preferred treatment for indirect CCFs in all patients due to a higher single session curative rate, higher long-term success and simplicity compared with the transarterial method (multiple arterial feeders and small size).8 The various approaches to the CCF include a posterior route from the common femoral vein to the internal jugular vein, the inferior petrosal sinus with subsequent access to the cavernous sinus. An alternative anterior approach may be pursued via the facial vein to obtain access to the SOV into the cavernous sinus. Once access to the sinus is obtained, treatment modalities similar to those used in transarterial approaches may be used.
However, a review by Shievink et al of the management of spontaneous CCF in patients with EDS demonstrated 58% mortality with 23% attributed to treatment complications.1 Treatment at that time included surgical ligation of the ICA or common carotid artery, surgical trapping of the fistula and transarterial balloon embolization with detachable balloons1 ,9 and stereotactic radiosurgery.10 ,11
Despite the advances in endovascular techniques in patients with EDS IV, complications are frequently reported. Most of these can be attributed to the need for arterial access for mapping the procedure from the common carotid artery. The complications are severe and include retroperitoneal hematoma, colonic rupture and iliac artery perforations.1 Recently, Khan et al reported successful embolization of a CCF in a patient with EDS IV by direct puncture of the highest cervical segment of the ICA after failure of a transvenous approach.12 In addition, Hollands et al reported a case of initial surgical exposure of the ipsilateral carotid artery and internal jugular vein with placement of endovascular sheaths in lieu of a transfemoral access.13
Our patient had a direct CCF which, in addition to the typical symptoms, was causing significant cerebral venous hypertension. Treatment was pursued from a transvenous route to minimize the high risk of arterial dissection caused by an arterial approach. The femoral access was challenging because of the presence of a previous dissection of the iliac and femoral arteries. We found that both ultrasonographic and continuous fluoroscopic guidance allowed us safe access to the true lumen of the dissected right femoral artery. The risk of arterial dissection was further minimized by navigating a 4 F glide catheter within the ipsilateral carotid artery to provide a roadmap and to monitor the progress of the occlusion of the CCF by the venous route. Detachable coils were safely used to successfully achieve progressive occlusion of the SOV and the bilateral cavernous sinus. Balloon-assisted infusion of embolic agents such as Onyx and nBCA were not considered due to the high risk of dissection of the ICA during balloon inflation.
In conclusion, patients with EDS IV are at high risk of developing spontaneous arterial dissection with pseudoaneurysm formation. In particular, they seem to be at high risk of developing direct CCF. The treatment of direct CCF in patients with EDS IV is possible, but with a high risk of complications. We found that simultaneous fluoroscopic- and ultrasound-guided access via the femoral artery was useful for safely accessing the femoral artery, even in a case of previous dissection with pseudoaneurysm formation.
Key messages
-
Patients with EDS type IV are at high risk of developing spontaneous arterial dissection with pseudoaneurysm formation, in particular direct carotid cavernous fistula (CCF).
-
Treatment of direct CCF in patients with EDS type IV is possible, but the risk of complications is high.
-
Simultaneous fluoroscopic- and ultrasound-guided access via the femoral artery is a useful technique, even in a case of previous dissection with pseudoaneurysm formation.
-
The transvenous approach can result in successful treatment of patients with EDS IV compared with transarterial approaches.
References
Footnotes
-
Republished with permission from BMJ Case Reports Published 2 January 2013; doi:10.1136/bcr-2013-010990
-
Contributors Study concept and design and acquisition of date: IL. Analysis and interpretation of data: all authors. Drafting of the manuscript: IL and EL. Critical revision of the manuscript for important intellectual content: all authors.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.