Article Text

Abstract
Background Endovascular therapy seems to benefit a subset of patients with large vessel occlusion strokes. We aimed to develop a clinically useful tool to identify patients who are likely to benefit from endovascular therapy.
Methods In a derivation cohort of consecutively treated patients with anterior circulation large vessel occlusion (Grady Memorial Hospital, N=247), independent predictors (p<0.1) of good outcome (90-day modified Rankin scale score (mRS) 0–2) were determined using logistic regression to derive the Pittsburgh Response to Endovascular therapy (PRE) score as a predictor of good outcome. The PRE score was validated in two institutional cohorts (University of Pittsburgh Medical Center (UPMC): N=393; Unitat d’Ictus Vall d’Hebron: N=204) and its discriminative power for good outcome was compared with other validated tools. Benefit of successful recanalization was assessed in PRE score groups.
Results Independent predictors of good outcome in the derivation cohort (age, baseline National Institute of Health Stroke Scale (NIHSS) score and Alberta Stroke Program Early CT Score (ASPECTS)) were used in the model: PRE score=age (years)+2×NIHSS−10×ASPECTS. PRE score was highly predictive of good outcome in the derivation cohort (area under the curve (AUC)=0.79) and validation cohorts (UPMC: AUC=0.79; UIVH: AUC=0.72) with comparable rates of good outcome in all PRE risk quartiles. PRE was superior to Totaled Health Risks In Vascular Events (THRIVE) (p=0.03) and Stroke Prognostication using Age and NIHSS (SPAN) (p=0.007), with a trend towards superiority to Houston Intra-Arterial Therapy 2 (HIAT2) (p=0.06) and iSCORE (p=0.051) in predicting good outcomes. Better outcomes were associated with successful recanalization in patients with PRE scores −24 to +49 but not in patients with PRE scores <−24 or ≥50.
Conclusions The PRE score is a validated tool that predicts outcomes and may facilitate patient selection for endovascular therapy in anterior circulation large vessel occlusions.
- Stroke
- Thrombectomy
- CT
- Intervention
Statistics from Altmetric.com
Introduction
Results from clinical trials comparing endovascular revascularization therapy (ERT) with intravenous thrombolysis for anterior circulation large vessel occlusion stroke (LVOS) have yielded neutral results,1–3 but several lines of evidence suggest that patients with severe stroke symptoms (National Institute of Health Stroke Scale (NIHSS) score ≥14) and/or proximal LVOS (intracranial internal carotid terminus (ICA-T) and M1 middle cerebral artery (MCA)) may benefit from ERT.2 ,4 ,5 In addition to the level of occlusion and NIHSS at presentation, several other factors (successful recanalization, established infarct core, Alberta Stroke Program Early CT Score (ASPECTS), age, baseline functional status and collateral status) also influence stroke outcome and need to be considered during patient selection for ERT.6 As a result, several prediction tools have been developed to aid patient selection, both in clinical practice as well as in defining the target population for clinical trials,7–10 but a standardized approach to patient selection for ERT is lacking across institutions.11 Optimal patient selection for ERT can minimize futile recanalization procedures, thereby limiting healthcare costs associated with ERT.12
Using independent predictors of good outcome that are available to the clinician prior to ERT, we derived the Pittsburgh Response to Endovascular therapy (PRE) score that incorporates age, NIHSS at presentation and ASPECTS on initial head CT scan and validated the PRE score in two large endovascular cohorts. The PRE score was also compared with previously validated scores that predict outcomes in patients with stroke.7 ,9 ,13 ,14 PRE score thresholds were defined to distinguish patients likely to benefit from those who do not benefit from successful recanalization.
Methods
Data source and subjects
The derivation cohort from the Grady Memorial Hospital (GMH) endovascular database (2008–2013) comprised consecutively treated patients. Demographic data, clinical data and 90-day modified Rankin scale score (mRS) as measured by the treating physician were prospectively collected for each patient. Adult patients (age ≥18 years) with anterior circulation LVOS (ICA-T, M1 and M2 MCA) who received ERT within 8 h from time last-seen-well (TLSW) with documented 90-day mRS were included. The first validation cohort of consecutively treated patients (2009–2013) was derived from the University of Pittsburgh Medical Center (UPMC) endovascular stroke registry (Pittsburgh, Pennsylvania, USA). Patients in this cohort underwent endovascular therapy at one of three UPMC-affiliated hospitals, each a comprehensive stroke center with endovascular, neurointensive and rehabilitative services. The second validation cohort of consecutively treated patients (2009–2013) was derived from Unitat d’Ictus Vall d’Hebron Neurology Hospital Vall d’Hebron, Barcelona, Spain (UIVH). Each site had institutional review board approval for the maintenance of endovascular stroke databases. Permission from all three centers was sought prior to use of individual databases.
Measurements
Baseline NIHSS scores at each site were calculated by the treating physicians. ASPECTS on non-contrast head CT scan upon arrival at the comprehensive stroke center was determined by the treating neurologist or stroke physician prior to endovascular treatment. All patients underwent CT or MR angiography prior to endovascular treatment but level of occlusion was confirmed by catheter-based angiography. Revascularization status (Modified Thrombolysis In Cerebral Infarction (mTICI) grade) was determined by the operating physician after the procedure. Comparison of PRE score with Houston Intra-Arterial Therapy 2 (HIAT2), Totaled Health Risks In Vascular Events (THRIVE) and Stroke Prognostication using Age and NIHSS (SPAN) index was performed after pooling all three patient cohorts and excluding patients with missing data points. The HIAT2 score, THRIVE, iSCORE and SPAN index were calculated as previously described.7 ,9 ,10 ,14 Final infarct volume (mL) was determined by measuring the area of the infarct on each slice (diffusion-weighted MRI scan within the first 48 h following treatment or first available non-contrast head CT scan after 24 h of treatment) and then summating individual slice thicknesses of all outlined areas.15
Statistical analysis
Categorical variables were compared with the Fisher exact test. Continuous variables were compared using the unpaired t test (two-tailed) for means and independent samples median test for medians. Variables significantly predictive (p<0.05) of good outcome (90-day mRS 0–2) in univariate logistic regression analysis were entered in multivariate logistic regression analysis and only significant independent predictors of good outcome (p≤0.1) were considered in the final model. Variables were weighted based on B coefficients relative to age (lowest B coefficient value). Each weight was rounded to the nearest integer and used in developing a composite score. Model calibration was assessed in the derivation cohort with the Hosmer–Lemeshow test (p>0.05 considered good calibration). In univariate regression (derivation cohort) with PRE score as a predictor of good outcome, we determined the predicted rates of good outcome in different POST score groups and compared these with observed rates (Pearson correlation coefficient was determined). Receiver Operating Characteristic (ROC) area under the curve (AUC) was used to assess the discriminative power of PRE for good outcome (excellent ≥0.80, very good ≥0.75). Statistical analyses were performed using IBM SPSS Statistics V.20. The discriminative power (AUC) of PRE was compared with other scores using the Hanley and McNeil method.16
Results
Patient characteristics
In the derivation cohort, 309 patients met the inclusion criteria and 62 patients were excluded due to missing imaging data or 90-day mRS. In the UPMC validation cohort, 426 patients met the inclusion criteria and 33 patients were excluded due to missing data variables. In the UIVH validation cohort, 244 patients met the inclusion criteria and 40 patients were excluded due to missing data variables. Patient characteristics and outcomes in the derivation (GMH, N=247) and validation cohorts (UPMC, N=393; UIVH, N=204) are summarized in table 1. Significant differences in age, NIHSS, ASPECTS, sex distribution, risk factors (diabetes, hypertension and atrial fibrillation), proportion of ICA-T occlusions, intravenous thrombolysis rates and final infarct volumes were observed (table 1). In all three cohorts the overall rate of good outcome was 40.1% (339/844) regardless of recanalization status.
Patient characteristics in the derivation and validation cohorts
Derivation and validation of the PRE score
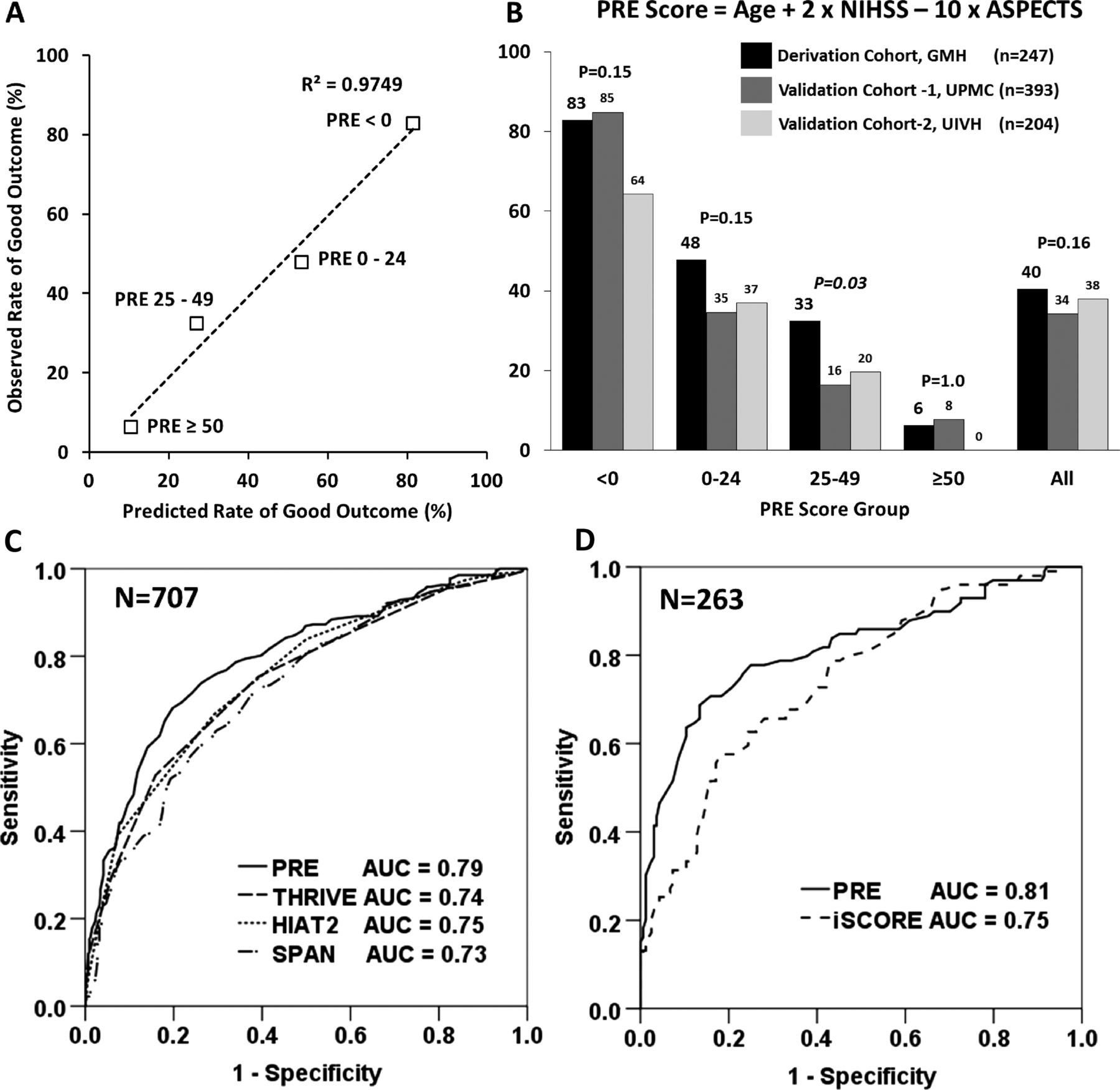
Univariate analysis in the derivation cohort identified age (p<0.001), NIHSS at admission (p<0.001), ASPECTS (p<0.001), female gender (p=0.016), hypertension (p=0.025), admission glucose level (p=0.02) and TLSW to groin puncture (p=0.048) as significant predictors of good outcome (p<0.05). Intravenous tissue plasminogen activator (tPA) (p=0.8), level of occlusion (p=0.26), hyperlipidemia (p=0.09) and atrial fibrillation (p=0.87) were not significant predictors in this analysis and were excluded from the multivariate analysis. In a multivariate analysis (table 2), only age (OR 0.96, 95% CI 0.94 to 0.99, p=0.002), NIHSS at presentation (OR 0.91, 95% CI 0.86 to 0.97, p=0.002) and ASPECTS (OR 1.36, 95% CI 1.21 to 1.51, p=0.001) on initial CT scan were independent predictors (p<0.10) of good outcome. Calibration of the regression model was satisfactory in the derivation cohort (Hosmer–Lemeshow test p=0.36). Individual factors were weighted based on B coefficients for each variable and a composite score was derived: PRE score=age+2×NIHSS−10×ASPECTS. A very strong positive correlation was observed between predicted and observed rates of good outcome in the derivation cohort (figure 1A). Discriminative power of the PRE score was assessed by calculating the AUC of a ROC curve to predict a good outcome and was compared across PRE score groups in the derivation and validation cohorts. Compared with the derivation cohort (AUC=0.79, p<0.001), PRE score predicted good outcomes in the UPMC (AUC 0.79, p<0.001) and UIVH (AUC 0.72, p=0.001) cohorts. Discriminative power of the PRE score was not affected by intravenous (IV) tPA use (AUC 0.794 (IV tPA) vs AUC 0.798 (non-IV tPA)). Patients were divided into PRE score quartiles (PRE <0, 0–24, 25–49, ≥50) and predicted rates of good outcome were compared with observed rates in the derivation cohort. Compared with the derivation cohort, the validation cohorts had similar rates of good outcomes in PRE <0 (p=0.15), 0–24 (p=0.15) and ≥50 (p=1.0) groups (figure 1B). The PRE 25–49 group in the validation cohorts had a lower rate of good outcome compared with the derivation cohort (p=0.03).
Results from multivariate analysis: Derivation of the PRE score

Pittsburgh Response to Endovascular (PRE) score validation and comparison with other validated clinical prediction scores. (A) Calibration of the PRE score in the derivation cohort: excellent degree of agreement between predicted and observed rates of good outcome across four PRE score groups (R2=0.98, p<0.001). (B) Comparison of the observed rates of good outcome in four PRE score groups in the derivation and validation cohorts showed no significant differences except for a slightly higher rate of good outcome in the PRE 25–49 group in the derivation cohort. (C, D) Comparison of discriminative power (area under the curve (AUC)) of PRE, THRIVE, HIAT2, iSCORE and SPAN for good outcomes (90-day modified Rankin scale score (mRS) 0–2). HIAT2, Houston Intra-Arterial Therapy 2; NIHSS, National Institute of Health Stroke Scale; SPAN, Stroke Prognostication using Age and NIHSS; THRIVE, Totaled Health Risks In Vascular Events.
Since octogenarians represent a significant proportion of LVOS, a uniform approach to treating these patients is also needed. Octogenarians accounted for 20.8% (175/843) of the entire cohort. Of the 175 octogenarians, only 24 had PRE ≥50 where ERT seems to be futile. In octogenarian patients with favorable PRE scores (PRE 0–49), successful recanalization (mTICI 2B/3) resulted in better outcomes compared with TICI 0–2A recanalization (35.2% vs 15%, p=0.008), and this difference was more pronounced in the PRE <25 group (52% vs 17%, p=0.004) (see online supplementary efigure 2).
Comparison of PRE score with other tools that predict outcomes in acute LVOS
In a combined analysis of the derivation and validation cohorts we compared the PRE score with previously published scores (THRIVE, HIAT2, SPAN and iSCORE) that predict outcomes in acute ischemic stroke. In 707 patients in the derivation and validation cohorts (figure 1C), PRE (AUC=0.79, 95% CI 0.74 to 0.85, p<0.001) was better than THRIVE (p=0.025) and SPAN (p=0.007). PRE score was not statistically superior to HIAT2 although a trend was observed (PRE AUC=0.79 vs HIAT2 AUC=0.75, p=0.06). In 263 patients in the UPMC database with parameters available to calculate the iSCORE (100 patients excluded due to missing data), PRE trended towards superiority over iSCORE in predicting good outcome (p=0.051, figure 1D).
PRE score can be used to identify patients likely to benefit from ERT
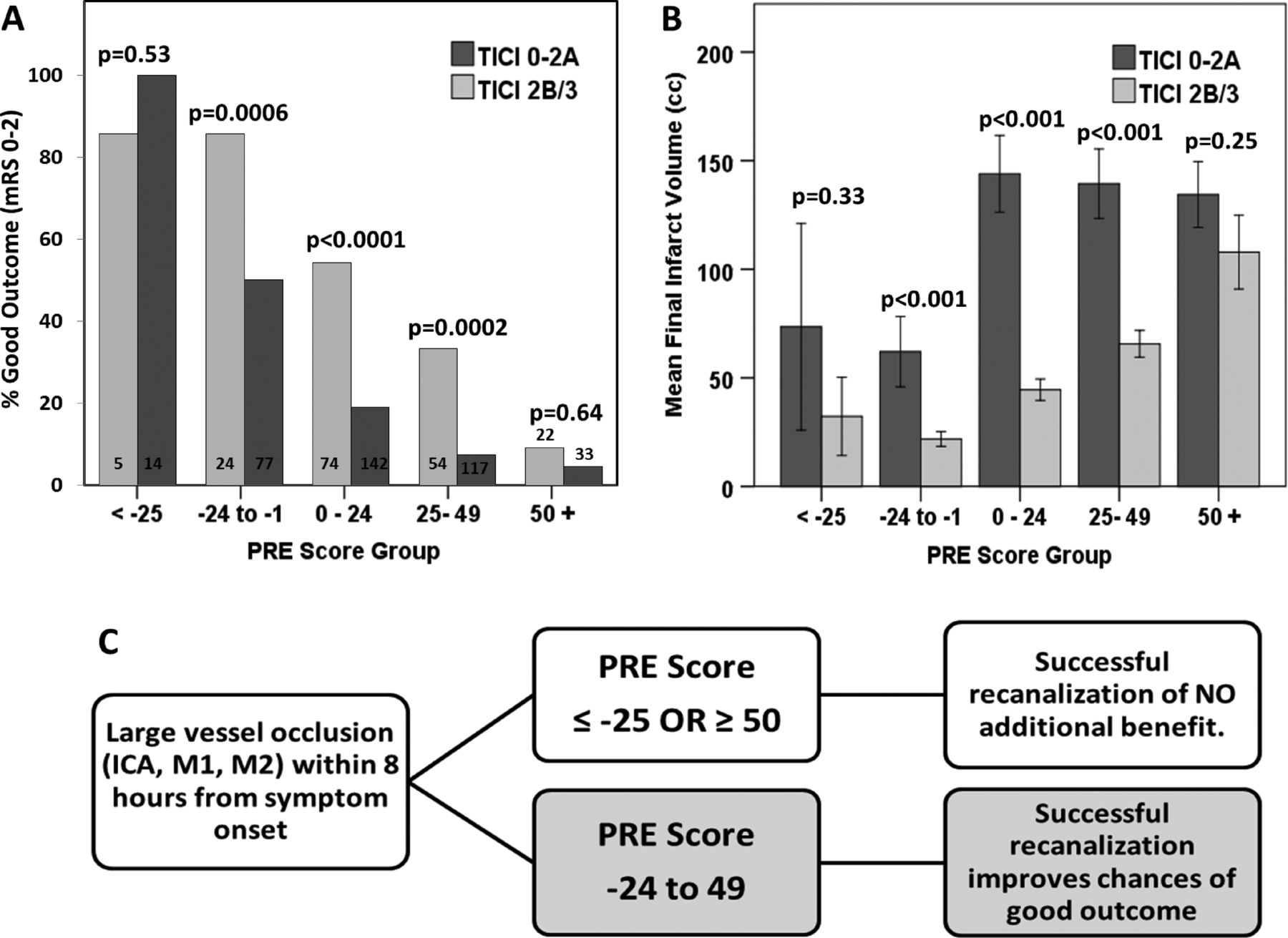
The benefit of ERT is mediated through recanalization of the occluded vessel, thereby limiting infarct volume growth. With new generation endovascular devices, successful recanalization after ERT is achieved in about 70% of cases. In a combined analysis of 562 patients in the three cohorts (282 patients excluded due to missing mTICI status or final infarct volume), successful recanalization (mTICI 2B/3) was achieved in 383 patients (68.2%). We have shown that a PRE score ≥50 is associated with a very low likelihood of good clinical outcomes following ERT. A true prediction of the benefit of ERT can be made if we compare outcomes in patients with and without successful recanalization (mTICI 2B/3) across various PRE score groups. In our database, successful recanalization resulted in higher rates of good clinical outcomes compared with mTICI 0–2A in PRE score groups −24 to −1 (p=0.002), 0–24 (p<0.001) and 25–49 (p=0.001) but not in PRE score groups ≤−25 (p=0.55) and ≥50 (p=1.0) (figure 2A). Rates of good outcome paralleled significantly smaller mean infarct volumes in the favorable PRE groups (PRE −24 to +49) but not in the PRE ≤−25 and PRE ≥50 groups (figure 2B). The PRE ≤−25 and PRE ≥50 groups together accounted for 13.2% (74/562) of patients in the combined database.
{kind=link}
{kind=link}
Identification of patients likely to benefit from recanalization with endovascular revascularization therapy (ERT). Comparison of (A) rates of good outcome (90-day modified Rankin scale score (mRS) 0–2) and (B) mean final infarct volumes in various Pittsburgh Response to Endovascular (PRE) score groups, dichotomized based on successful recanalization (Modified Thrombolysis In Cerebral Infarction (mTICI) 2B/3). (C) Suggested algorithm for using the PRE score in decision making for patient selection for ERT. ICA, internal carotid artery.
Discussion
Results from recent trials and other studies comparing ERT with intravenous thrombolysis for LVOS1 have shown that ERT is not the treatment of choice for all LVOS but seems most effective in proximal occlusions with higher NIHSS scores,2 that it is effective only if successful recanalization is achieved,3 and better patient selection is of key importance for future trials.4 ,17 ,18 It is imperative to ensure that ERT is offered only to patients who are likely to benefit, while avoiding unnecessary interventions in patients who are either ‘too good’ or ‘too bad’ to treat.19 Several scoring tools for outcome prediction and patient selection for ERT have been developed but very few of these are routinely used in clinical practice.20
We developed and validated the PRE score to serve as a simple tool that can be used at the bedside to help clinicians in selecting patients with acute LVOS for ERT. The PRE score incorporates age, NIHSS at presentation and ASPECTS on initial CT scan as independent predictors of good outcome following ERT. This score is easy to calculate, incorporates factors that are commonly used in the acute setting before an MRI scan is available to determine the exact infarct burden and is independent of time to treatment or IV tPA use. Prognostication of good outcome prior to implementation of a potentially effective intervention should dichotomize the predictions based on success or failure of the intervention. The PRE score, when used in the context of revascularization status (mTICI 2B/3), is able to identify subgroups of patients (PRE −24 to +49) who are likely to benefit from ERT (figure 2C). A PRE score ≥50 identifies patients where ERT is very likely to be futile in preventing disability. This ‘too bad to treat’ population probably represents older patients with lower ASPECTS scores and higher NIHSS scores (see online supplementary eFigure 1). These results are also consistent with previous studies that identified age >70 and NIHSS score ≥20 as independent predictors of futile recanalization in patients with LVOS.21 Patients with a PRE score ≤−25 seem to do well regardless of ERT, tend to be younger with lower NIHSS scores and higher ASPECTS (see online supplementary eFigure 1), but predictors of outcome in this population need to be defined. The ability to identify a ‘too good to treat’ population is a unique feature of the PRE score. In addition to being intuitive, the PRE score provides quantitative data to guide families or surrogate decision makers with regard to realistic expectations from endovascular interventions. A comparison of outcomes in successfully recanalized (mTICI 2B/3) versus non-recanalized (mTICI 0–2A) patients also yields a rough estimate of the number of patients needed to be recanalized (NNR) in order to achieve one additional good outcome in each favorable PRE score group (PRE score −24 to 1: NNR=2.8; 0–24: NNR=2.6; 25–49: NNR=3.85). While further validation of the PRE score in an endovascular trial database would be useful in confirming our findings, these preliminary estimations may guide sample size calculations for future trials comparing ERT with intravenous thrombolysis within the 4.5 h time window as well as in trials enrolling patients beyond 4.5 h where tPA is not effective.
Clinical scoring systems are not meant to supersede clinical judgment but assist and build confidence in a medical decision made emergently, frequently by surrogate decision makers with guidance from the treating physician. Prognostic scores should also balance predictive accuracy with simplicity in order to be clinically useful. The SPAN index, for example, is a highly simplistic two-variable score with the lowest predictive accuracy in our analysis. The iSCORE, on the other hand, is a highly complex tool that incorporates numerous variables and cannot be determined without an online calculator. The THRIVE score, which incorporates age, NIHSS and three risk factors (diabetes mellitus, hypertension, atrial fibrillation),7 and the HIAT2 score, which incorporates age, NIHSS, glucose and ASPECTS,14 have both been validated in endovascular cohorts. Compared with these, the PRE score incorporates only three variables and, despite its simplicity, seems to be superior to THRIVE, HIAT2 and iSCORE. This could be due to use of age, NIHSS score and ASPECTS as continuous variables in our model rather than categorical variables, which could overcome any loss of predictive power resulting from categorization of variables. Whether a scoring tool such as the PRE score is helpful in clinical practice and decision making needs to be prospectively validated.
Studies have suggested that octogenarians with LVOS are less likely than younger patients to achieve successful recanalization or good outcomes following ERT.22 While our analysis in octogenarians is limited by small sample size and selection biases, we did find that patients with a favorable PRE score had better outcomes with successful recanalization, suggesting that ERT in octogenarians with PRE score <50 is reasonable and should be evaluated prospectively.
Hospital costs related to endovascular therapy can also be prohibitive in limited resource settings and a cost-effective analysis of ERT in acute ischemic stroke has not been performed. In our study, 13% of patients were very unlikely to benefit from ERT (PRE ≤−25 or PRE ≥50). Excluding these patients from ERT may limit futile procedures and unnecessary hospital expenses at an aggressive endovascular center. Conversely, at a conservative center, procedure-related costs may increase due to a larger number of patients that can be considered for ERT, but this could be offset by lowered disability and nursing home or rehabilitation costs. Only results from ongoing clinical trials will confirm the benefit (or lack) of ERT in LVOS.
Certain limitations of our study need to be acknowledged. Our analysis is retrospective and is prone to selection bias due to varying endovascular practices at each institution. Significant differences in baseline demographics in our derivation and validation cohorts were also observed. Since patients without mRS at 90 days were excluded, selection bias due to patients lost to follow-up may explain the non-significant differences in median follow-up mRS in the derivation and validation cohorts. Nevertheless, the PRE score predicted clinical outcomes in a comparable manner, supporting its wide applicability to patients with anterior circulation LVOS regardless of epidemiologic disparities. Surprisingly, variables such as IV tPA use, level of occlusion and atrial fibrillation were not significant predictors of good outcome. This could be explained by the limited sample size of the derivation cohort and selection biases. It is also possible that, in the LVOS population, these variables have a smaller influence on outcome. Since all patients were treated with endovascular therapy, many patients may have been treated shortly after tPA administration, thereby possibly masking any potential recanalization-mediated benefit of IV tPA. Baseline disability was not included in our model due to the selection bias of not offering ERT to patients with significant baseline disabilities (mRS ≥3) at most centers. Only 1% (2/204) patients who were treated at UIVH had a baseline mRS ≥3. The PRE score must therefore be applied with caution to patients with major baseline disabilities. Although the PRE score was not validated in a tPA-ineligible population, we expect comparable results since the discriminative power of PRE was not affected by the utilization of IV tPA. The PRE score was not validated in patients treated beyond 8 h from TLSW, but we expect the PRE score to retain its predictive accuracy in these patients because time to treatment was not an independent predictor of outcome in our analysis, an observation explained by the close association between time to treatment and ASPECTS. Finally, since the majority of patients were >35 years of age, the PRE score has not been validated in very young patients. Further validation of the PRE score in an endovascular trial database may overcome many of these limitations.
In conclusion, we have derived and validated the PRE score as a simple tool to predict outcomes in patients with LVOS prior to ERT. Patients with a PRE score of −24 to +49 seem to benefit from ERT if successful recanalization is achieved. The PRE score also performs better than previously validated scoring tools and can be useful in clinical practice and in future endovascular trials.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
Contributors SR:study concept and design, acquisition of data, analysis and interpretation. AA, C-HS, MR, MM, AJ: acquisition of data, critical revision of manuscript for important intellectual content. CS, RN, RG, MF: critical revision of manuscript for important intellectual content. TGJ: study supervision, study concept and design, analysis and interpretation.
Competing interests RG: consultant to Stryker Neurovascular, Covidien, Rapid Medical, Royalties: UpToDate, Associate editor of Journal of Neuroimaging and Interventional Neurology. RN: Stryker Neurovascular (PI for TREVO-2 and DAWN Trials), Covidien (Steering Committee SWIFT trials; Core Lab-STAR trial), Penumbra (Executive Committee-3D Separator trial). TGJ: consulting and speaker fees from Co-Axia, ev3, Concentric Medical and Micrus.
Ethics approval Institutional Review Board (retrospective analysis).
Provenance and peer review Not commissioned; externally peer reviewed.