Article Text

Abstract
Introduction/purpose Developmental venous anomalies (DVAs) are variations of normal transmedullary veins that are necessary for the drainage of white and gray matter. DVAs are predominantly benign anatomic variations and are usually incidentally discovered. In exceedingly rare cases, DVAs can be symptomatic due to mechanical or flow-related pathophysiological mechanisms. Restriction of outflow can produce a variety of morphological and clinical presentations ranging from venous congestive edema to hemorrhage. We present a case of a 53-year-old female with an infratentorial thrombosed DVA that caused venous congestive edema.
Materials and methods A retrospective review of the patient’s electronic medical record including inpatient notes and all radiological exams was performed.
Results A 53 year-old female without past medical history presented to the emergency room with 3 days of headache, vertigo and ataxia. On physical examination, she demonstrated left upper extremity dysmetria and abnormal gait. MRI of the brain showed tortuous venous structures in the left cerebellar hemisphere and left side of the pons converging into a prominent structure with extensive susceptibility artifact. There was increased T2/FLAIR signal in the pons, left brachium pontis and dorsal medulla. These findings were consistent with a thrombosed developmental venous anomaly causing venous congestive edema. The patient was placed on steroids and diagnostic cerebral angiography confirmed the DVA. No other vascular malformation was identified. Demonstration of a thrombosed DVA in the absence of an associated cavernous malformation, arteriovenous malformation or dural fistula justified treatment with anticoagulation. Her symptoms improved on steroids and she was continued on anticoagulation.
Conclusion Although the vast majority of DVAs are benign lesions, understanding the pathophysiological mechanisms behind symptomatic DVAs is important for treatment. We present a case of thrombosed DVA in the absence of additional vascular abnormality, thus justifying anticoagulation therapy. Differentiating a thrombosed DVA from a partially thrombosed arteriovenous malformation or dural fistula is vital as these other conditions may warrant surgery, radiosurgery or endovascular embolization.

{kind=link}
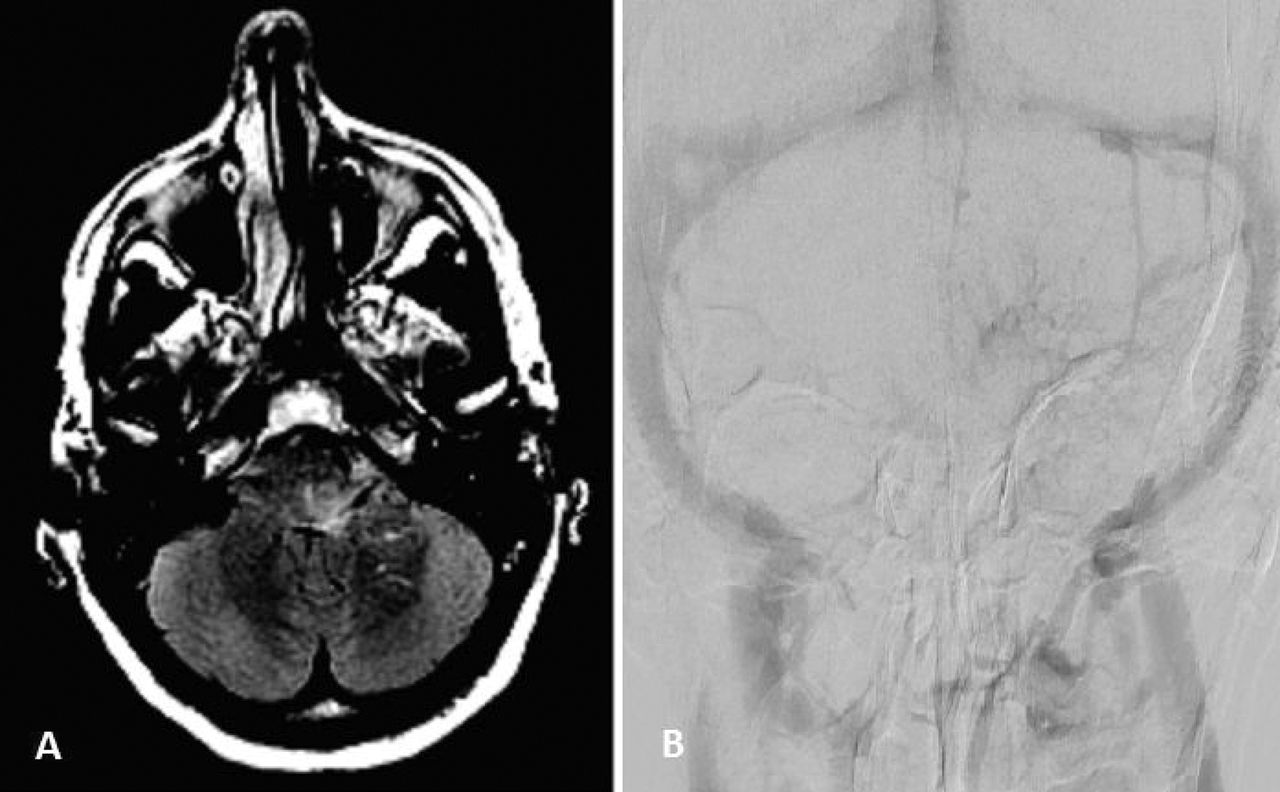
(A) Axial FIESTA image shows edema in left side of the pons and brachium pontis causing mass effect on the fourth ventricle. Several medullary veins converge onto a prominent venous structure extending towards the cerebellopontine angle cistern. (B) Venous phase of DSA shows a collection of dilated medullary veins in the left cerebellum converging to an enlarged collector vein. No arteriovenous malformation or dural fistula was seen
Disclosures K. Amuluru: None. Y. Alderazi: None. C. Gandhi: None.