Article Text

Abstract
Introduction/Purpose Malapposition has a negative correlation to aneurysm healing1. We examine the influence of malapposition communicating into the aneurysm, and the effect of malapposition incidence at any position along the parent artery on healing. We define communicating malapposition (CM) as any malapposition along the aneurysm neck (figure 1). We hypothesize that CM seen on optical coherence tomography (OCT) results in lower aneurysm occlusion rates after 30 days, and that malapposition at any other point along the parent artery has no effect.
Materials and Methods Fifty New Zealand White rabbits underwent elastase-induced aneurysm creation.2 After 21 days, animals were randomly implanted with: Pipeline Embolization Device (PED; n=20); Pipeline Embolization Device with Shield technology (SHIELD; n=20); or, Flow Reduction Endoluminal Device (FRED; n=10). Five days prior to implantation, 10 animals from each group began dual antiplatelet therapy (DAPT; aspirin/clopidogrel 10 mg/kg each) which was continued daily until the 30 day terminal endpoint. All animals were used for statistical analysis in this study since the influence of DAPT yielded no significant impact on rates of aneurysm occlusion. All animals underwent post-deployment OCT to assess device/vessel apposition. At 30 days, DSA and OCT were acquired to assess aneurysm healing. The incidence of CM was assessed on a binary scoring system: 0 CM present; 1 CM absent. Aneurysm healing on DSA was measured using a previously developed 5-point scale3 – a score of 3 or 4 (neck remnant or complete occlusion) was considered a positive outcome. Separately, the presence of malapposition distal to the aneurysm neck was measured on a similar binary scale: 0- malapposition seen distal to aneurysm; 1 – no malapposition observed. A Fisher’s exact test was used to show significance.
{kind=link}
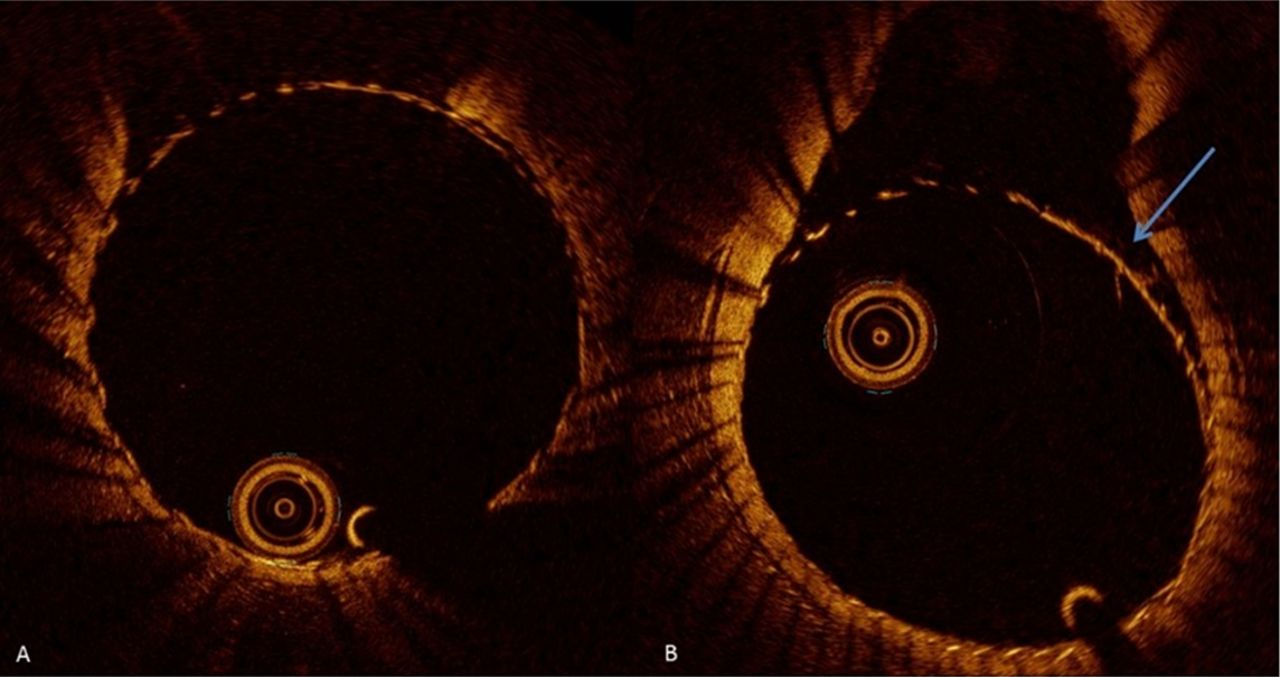
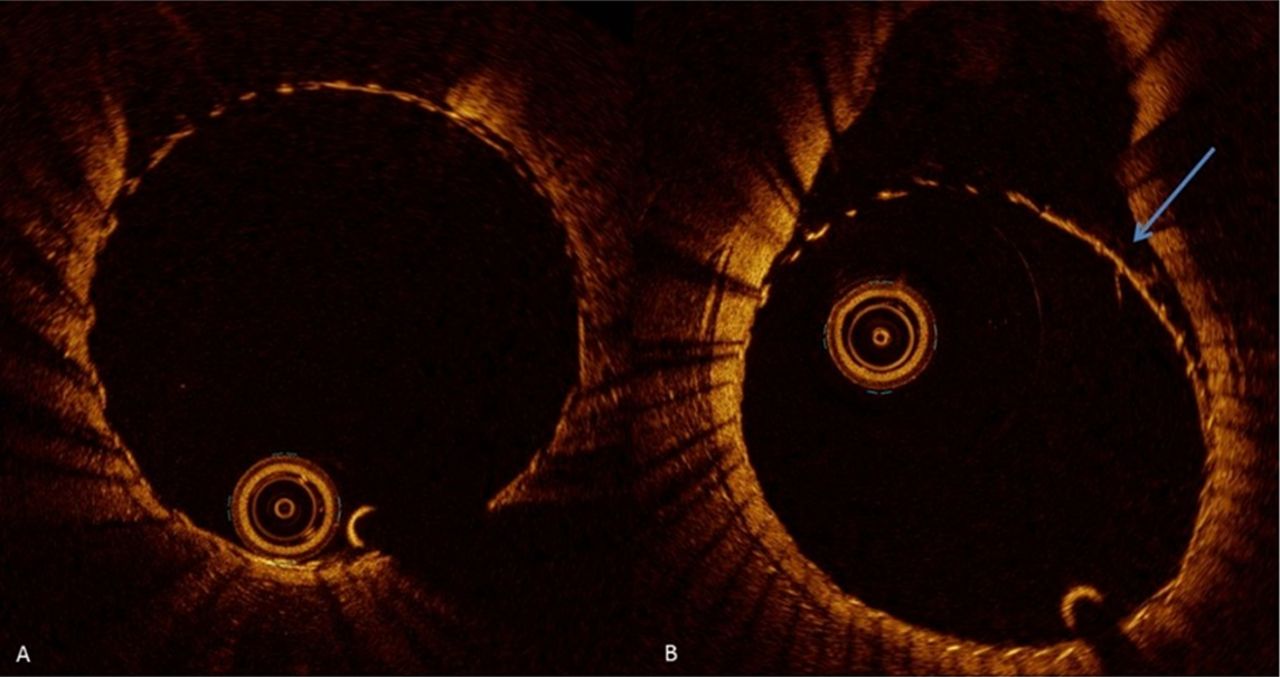
(A) OCT slice of aneurysm neck showing no communicating malapposition – final DSA occlusion score=4; (B) OCT slice of aneurysm neck showing communicating malapposition (arrow) – final occlusion score=1
Results Overall positive aneurysm outcome at 30 days was seen in 50% of cases (n=25), with no CM seen in 80% of those cases (n=20). Significant interaction between no CM and positive outcome was confirmed by a Fisher exact test, p=0.0014. When malapposition incidence along the parent artery distal to the aneurysm was compared to positive outcome, no significant interaction was found, p=0.776.
Conclusion OCT shows potential in serving as an indicator of poor outcome in the presence of CM during device implant. From these data, absence of communicating malapposition is strongly associated with early aneurysm occlusion, whereas malapposition distal to the aneurysm showed no effect on rates of aneurysm healing.
References
. AJNR 2016;37(11):2087–91.
2. AJR. 2000;174:349–354.
. AJNR 2012;33(10):2004–9.
Disclosures R. King: None. O. Brooks: None. E. Langan: None. M. Marosfoi: None. F. Clarençon: None. T. Tamaura: None. J. Wainwright: 5; C; Medtronic Neurovascular. M. Gounis: 1; C; Medtronic Neurovascular. A. Puri: 1; C; Medtronic Neurovascular.