Article Text

Abstract
We report a case of a 72-year-old man who had undergone elective stenting of an asymptomatic high grade stenosis of the proximal left internal carotid artery. The indication was progression of the stenosis over a 3 year period despite receiving maximal medical therapy, and patient preference for stenting over endarterectomy. He became profoundly hypotensive in the immediate post-stent period and required immediate and prolonged vasopressor support over the next week. The etiological hypothesis is baroreceptor hyperactivity related to procedure induced unilateral stretching of the carotid body.
- Blood Pressure
- Stent
- Vessel Wall
Statistics from Altmetric.com
Background
Carotid stenosis is a common and important risk factor for ischemic stroke, where treatment options include carotid endarterectomy (CEA) or carotid angioplasty and stenting (CAS). Recent (and controversial) trials have suggested that CEA should generally be preferred as the safer treatment1 ,2 although CAS is preferred in some high risk patients and patients with unfavorable anatomy, previous ipsilateral CEA or contralateral vocal cord palsy, open tracheostomy, previous radical neck dissection, or radiotherapy.3 Treatment of asymptomatic disease is more controversial due to the lower risks of stroke, particularly with advances in medical management, including the use of statins to lower cholesterol.
Commonly recognized CAS complications include thromboembolic events but hemodynamic depression (defined loosely as hypotension, bradycardia, or both) also occurs. Transient hypotension is common and is most often related to stretching of the vessel by the balloon and/or stent and stimulation of carotid baroreceptors and consequent fall in vascular tone. This effect generally lasts only minutes and sometimes several hours, but is rare beyond 48 h. If hypotension is prolonged, vasopressor support may be required. We present the first published case report of persistent hypotension requiring vasopressor support lasting beyond 1 week.
Case presentation
A 72-year-old man was referred for management of a high grade carotid stenosis which was initially detected on a carotid artery duplex in 2009 because a bruit was detected during a routine health check. The stenosis was characterized in the 50–69% range. A progress carotid duplex ultrasound performed several months prior to presentation demonstrated progression of the plaque to >80% on the left side. The plaque was calcific, heterogeneous, and ulcerated along its proximal 3 cm. The right internal carotid artery (ICA) had a similar morphology but was stenosed at 40–60%. He was asymptomatic.
He was an ex-smoker with mild dyslipidemia (total cholesterol 4.1, triglycerides 1.3, high density lipoprotein cholesterol 0.9, and low density lipoprotein cholesterol 2.6) and impaired fasting glucose (6.3 mmol/L). He had taken aspirin and simvastatin for several years. A cardiologist had recently added an angiotensin II receptor blocker to improve his vascular risk factor profile, but he had a normal range of blood pressure levels.
Other past history included spinal canal stenosis that had required L4/5 decompression, erosive gastritis, and benign prostatic hypertrophy. His medications were aspirin, telmisartan 20 mg daily, simvastatin, and temazepam.
The clinical examination was unremarkable except for neck bruits, prominent on the left and mild on the right side.
Considering the potential risk of stroke in the medium–long term in the absence of serious comorbidities, and otherwise good health, intervention was advised and agreed. Due to social circumstances, the patient opted for CAS over CEA because of the convenience of being minimally invasive and requiring a shorter hospital stay. The patient was informed of the risks/complications of the procedure and consent was obtained.
There was no history of autonomic dysfunction, with his blood pressure recordings (n=14) from his general practitioner averaging 117/68 mm Hg and heart rate 74 beats/min over the prior 2 years. He had longstanding ECG changes showing right bundle branch block, and an exercise stress echocardiography had shown no signs of myocardial dysfunction and normal physiological adaptations to exercise.
He was admitted to hospital electively for the procedure.
Treatment
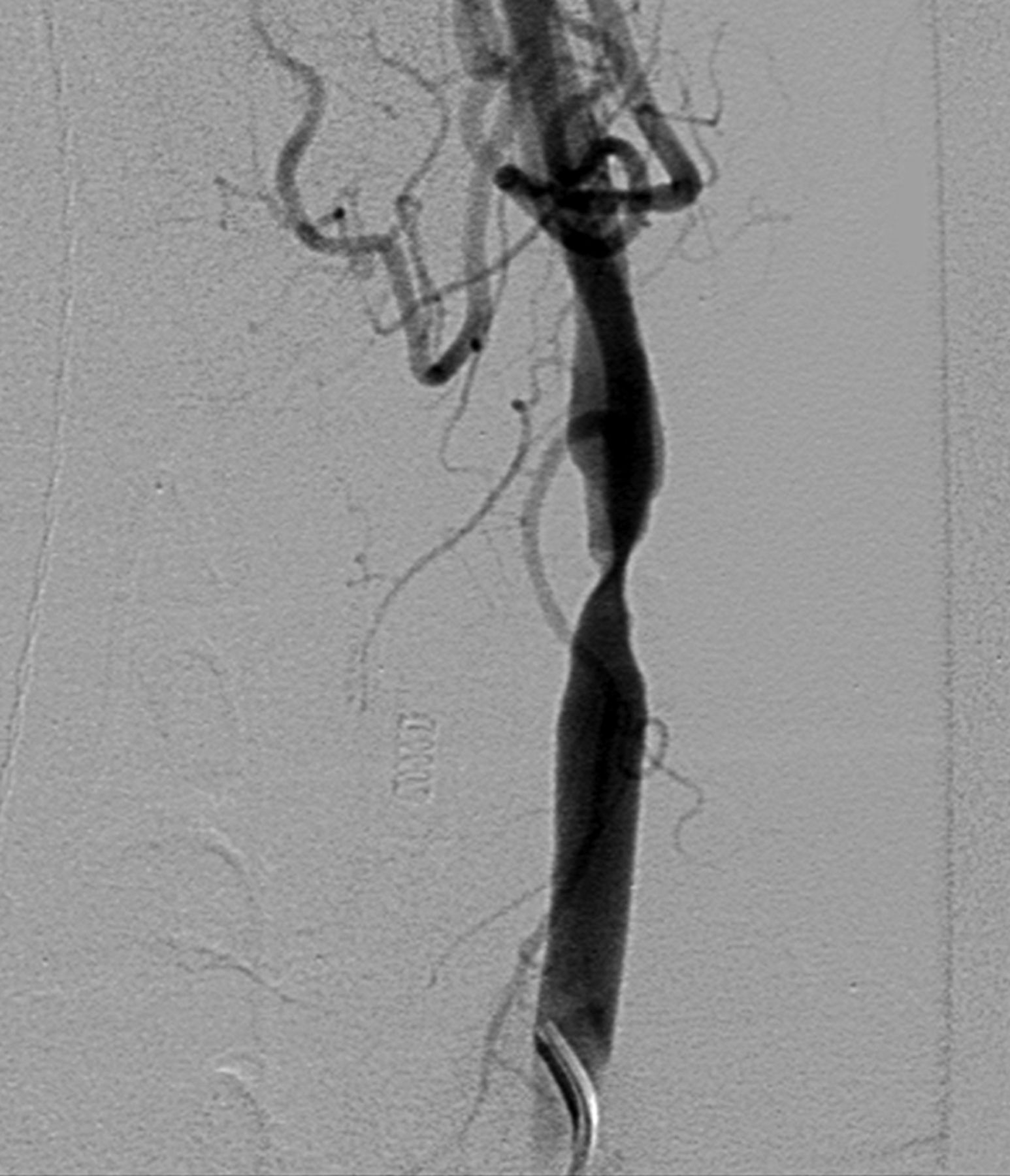
Injection of the left common carotid artery showed the stenosis at the origin at the left ICA with adjacent calcified plaque. The stenosis was measured as 50% using the NASCET (North American Symptomatic Carotid Endarterectomy Trial) criteria in the lateral projection but in the frontal projection appeared much more severe as the left ICA origin was slit-like. The left ICA more distally appeared normal.
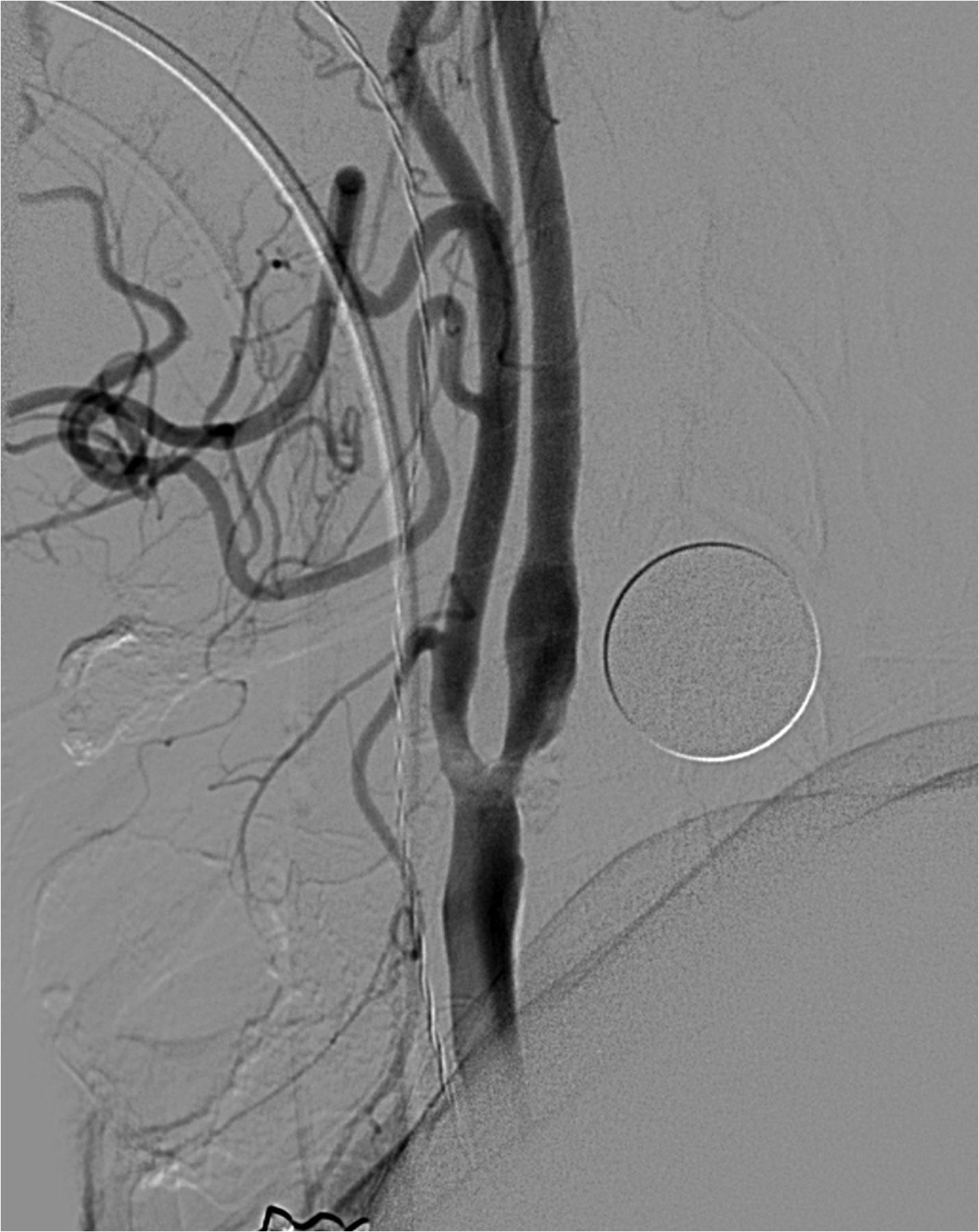
After discussion with the treating neurologist, a filter wire was placed across the left ICA origin using a 6 F shuttle sheath, and a 7 mm×40 mm carotid Wallstent was then deployed across the stenosis in a satisfactory position. Post-dilatation was performed with a 6 mm balloon to 8 atm, producing a substantial improvement in caliber at the origin of the left ICA with this improvement present both in the anteroposterior and lateral planes. There were no immediate complications observed (figures 1⇓⇓–4).
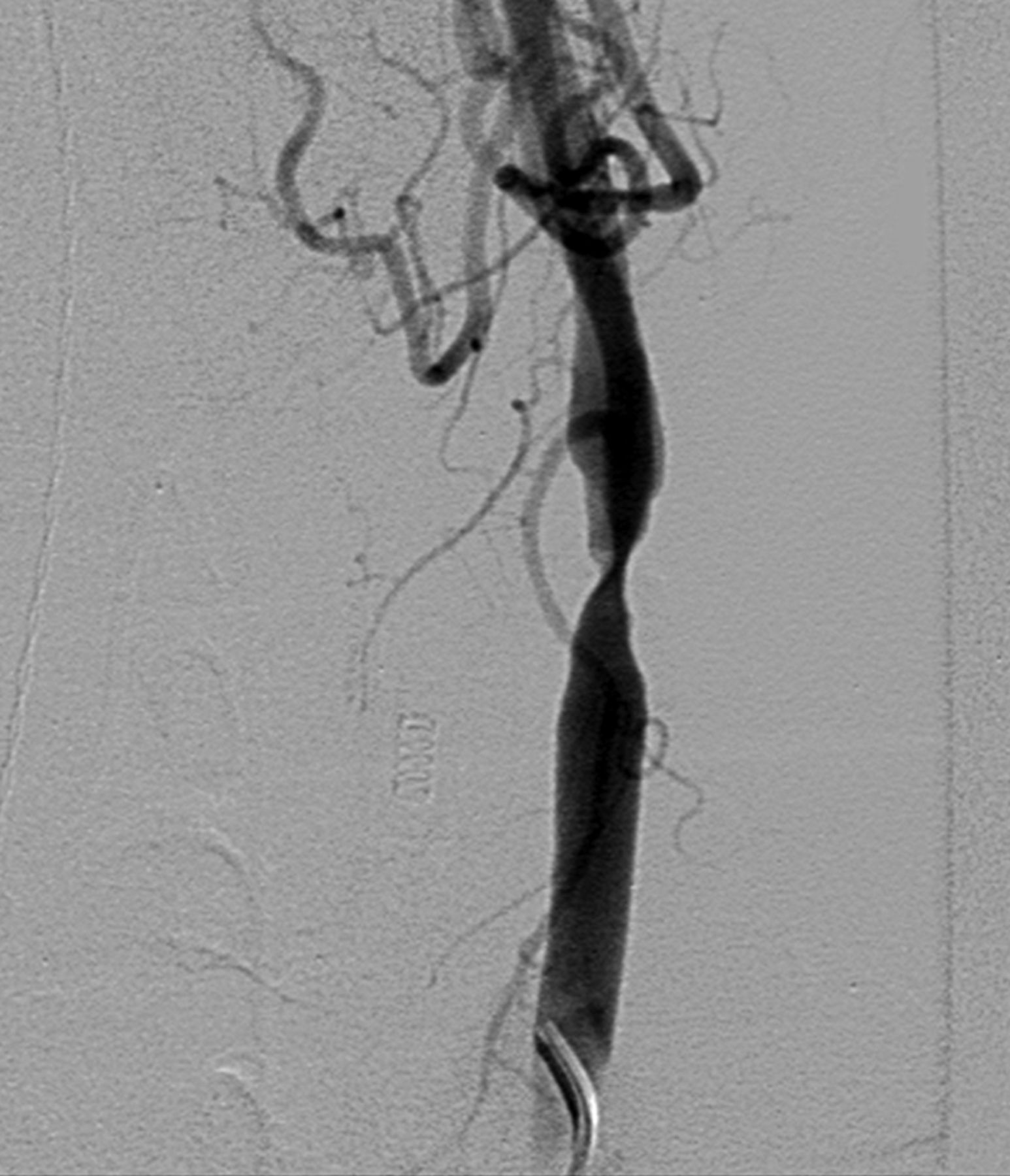
Selective injection of the left common carotid artery, demonstrating >90% stenosis of the left internal carotid artery in the anteroposterior projection.

Post-stenting in the anteroposterior projection.
Selective injection of the left common carotid artery, demonstrating >50% stenosis of the left internal carotid artery in the lateral projection (North American Symptomatic Carotid Endarterectomy Trial (NASCET) criteria).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Post-stenting in the lateral projection.
Outcome and follow-up
He received a standard general anesthetic protocol and required boluses of metaraminol shortly after the general anesthetic agents were administered and a further bolus 30 min after the stent was deployed. He received a total of 14.5 mg of metaraminol for the whole procedure. He did not suffer bradycardia or hypotension immediately following angioplasty and stenting but did require intermittent vasopressor support once under anesthesia. Once in recovery and extubated, the patient's blood pressure remained stable over a period of 90 min without further vasopressor support. On arrival in the high dependency unit, his blood pressure had dropped to a systolic pressure of 63 mm Hg via an arterial line measurement. Intravenous fluids and metaraminol infusion were commenced to stabilize his blood pressure.
Over the next few days, he required continued support hemodynamically. While his blood pressure remained fairly low (systolic <100 mm Hg) and sinus bradycardia was encountered frequently, his renal function and urine output remained within normal limits. He complained of orthostatic symptoms on sitting up bed, which was avoided.
There was no evidence of a cardiac injury, as evident by regular cardiac enzymes, ECGs, and transthoracic echocardiography being normal. He denied any puncture site or abdominal pain, and his hemoglobin remained stable.
On day 4 post-procedure, midodrine was commenced and increased to 15 mg four times a day. While there was no major improvement in blood pressure, this allowed the metaraminol infusion dose to be reduced. At this stage, consideration was given to removing the carotid stent due to concerns that it had irreversibly altered his hemodynamic physiology. Fortunately, the patient's symptoms and blood pressure improved within the next 24 h, and he was then discharged with midodrine which was then discontinued 1 week later.
Discussion
Hemodynamic depression is a common but usually transient and temporary occurrence in carotid stenting. In this case, hemodynamic depression persisted for over 1 week but ultimately resolved spontaneously. This is the first published case of hemodynamic depression persisting for over 1 week.
Key messages
-
Risk factors for prolonged hemodynamic depression include severely calcified plaque or high grade stenosis (>70%), proximity to the carotid bulb, balloon angioplasty including multiple dilatations and balloon angioplasty with balloon pressure >8 atm, bilateral stenting,4 increased age or poor ejection fraction,5 and β-blocker use.6
-
It is probable that the need for high pressure post-stenting dilatation due to the resistant nature of carotid stenosis caused unusually prolonged hemodynamic depression in this case.
-
Furthermore, this case highlights the appropriate use of inotropes and eventual resolution with hemodynamic support.
Footnotes
-
Republished with permission from BMJ Case Reports Published 9 January 2014; doi:10.1136/bcr-2013-011016
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Not commissioned; externally peer reviewed.