Article Text

Abstract
Introduction While the use of intraoperative angiography (IA) has been shown to be a useful adjunct in aneurysm surgery, its routine use remains controversial.
Objective We wished to determine if IA is required in all patients undergoing aneurysm surgery (ie, routine IA) or if intraoperative assessment can reliably predict the need for IA (ie, select IA).
Methods We prospectively evaluated all patients undergoing craniotomy for aneurysm clipping. In these patients, the treating surgeons were asked to record whether they felt IA was required at two time points: (1) prior to surgery and (2) immediately after clip application but before IA. All patients underwent IA as per the institutional protocol. IA results and the need for post-IA clip adjustments were recorded.
Results Of the 200 patients enrolled, 197 were included for analysis. IA was deemed necessary on preoperative assessment in 144 cases (73%) and on post-clip assessment in 116 cases (59%). Post-clip IA demonstrated 47 (24%) positive findings and post-IA clip adjustments were made in 19 of 198 cases (10%). On preoperative assessment, there were four cases where IA was deemed unnecessary, yet post-IA clip adjustment was required, resulting in a sensitivity of 79% and false negative rate of 8%. Regarding post-clip assessment, there were five cases where IA was thought to be unnecessary and clip adjustment was required, resulting in a sensitivity of 73% and false negative rate of 6%.
Conclusions The accuracy of a strategy of select IA was not improved by assessing the need for IA immediately after aneurysm clipping versus prior to surgery onset. This suggests that intraoperative assessment regarding the adequacy of aneurysm clip application should be viewed with caution.
- Aneurysm
- Angiography
- Subarachnoid
Statistics from Altmetric.com
Introduction
Surgery for aneurysmal subarachnoid hemorrhage is based on two overriding principles. The first is that the aneurysmal sac should be completely obliterated and isolated from the cerebrovasculature. Secondly, cerebral blood flow should otherwise remain unobstructed.1 A surgeon's ability to optimize the balance between these two factors has a great impact on the success of the surgery.2
It has long been known that obtaining this balance can be a difficult matter, which goes beyond technical skill and experience alone.1 ,3–6 One of the earliest to acknowledge this fact were Allcock and Drake1 when they reported their experience showing that 19% (13 of 70) of patients who had undergone craniotomy for aneurysm clipping were found to have an unexpected remnant on postoperative angiography and 9% (6 of 70 patients) to have vessel occlusions. In a subsequent study, Drake and Vanderlinden3 reported the long term follow-up of these patients, where the aneurysmal remnants were found to be significant, as 44% (11 of 25 patients) presented with recurrent subarachnoid hemorrhage. This group later presented a second larger study4 where 13% (43 of 329) of patients who underwent postoperative angiography were found to have a aneurysmal remnant, and from these 28% (12 of 43) suffered a re-hemorrhage. Similarly, Le Roux et al2 found an aneurysmal remnant rate of 5.7% and an inadvertent vessel occlusion in 5.7% of 637 treated aneurysms. In addition, they showed that vessel occlusion was a significant predictor of postoperative neurological deficit. The risk of re-hemorrhage was calculated by Feuerbertg et al5 in a retrospective analysis of 28 aneurysmal ‘rests’, which was estimated to be 0.38–0.79% per year.
From these results, it is clear that the ability to immediately evaluate and correct imperfect clip placement is highly desirable. To provide this function, the use of intraoperative angiography (IA) was developed.7–9 IA has since become a useful adjunct to aneurysm surgery, as it allows the surgeon to assess the clip placement and patency of associated cerebral vessels while still in the operating room. In the event that a problem is discovered, the surgeon can make near immediate adjustments. Many centers utilize and recommend routine IA, and have found that clip adjustments are required in approximately 7–17% of cases.6 ,10–12 IA, however, is not without risk, as complication rates are reported to range from 0.4% to 2.6%.6 ,10 ,12 ,13 Moreover, angiographic studies add to the expense and time of each case.14
The logistical difficulty, risk of complication, added expense, and development of newer technologies, such as micro Doppler, Charbel flow probe, and indocyanine green angiography (ICGA), have led some to suggest that IA should be used on a selective basis only.14–16 However, it continues to be shown that the sensitivities of these tools are less than that of IA and can lead to unexpected findings.17 ,18 Yet, because only a minority of patients undergoing aneurysm surgery ultimately have clip adjustments based on IA results, clearly it would be beneficial if angiography could be utilized in a more selective manner; however, very few data comparing selective versus routine IA for aneurysm surgery are available.
The purpose of this study was to determine if routine IA is required. It is clear from previous studies that preoperative assessment can be misleading, resulting in missed vessel occlusions and aneurysm remnants.6 We propose that the treating neurosurgeon can reliably predict which patients will need IA based on assessments made immediately after aneurysm clip placement. From this hypothesis we wished to qualify the surgeon's ability to assess clip placement prior to IA, evaluate what factors prompt surgeons to make these decisions, and determine characteristics that would allow for the classification of patients as requiring routine versus selective IA.
Methods
This study was approved by the institutional review board within the Human Research Protection Office at Washington University in St Louis.
Study design
The study design was a prospective evaluation of all patients undergoing craniotomy for aneurysm clipping during the 4 year recruitment period. Each patient underwent preoperative digital subtraction angiography, which was reviewed by the treating neurosurgeon and attending neurointerventional radiologist (figure 1). After the preoperative angiogram and prior to surgery, the treating neurosurgeon, via questionnaire, documented whether an IA would be required (figure 2). The neurosurgeon and neurointerventional radiologist also noted factors that led to this determination: aneurysm size, location, neck morphology, calcification, thrombus, and parent/branch vessel involvement with the aneurysm. The patient then underwent aneurysm clipping. The operative approach, clipping technique, use of Doppler ultrasound, use of Charbel flow probe, and use of ICGA were determined by the treating neurosurgeon. Prior to IA the treating neurosurgeon returned to the questionnaire and documented whether they felt an IA was indicated. Again, the factors used in determining this decision were recorded: aneurysm size, location, neck morphology, concern for aneurysmal remnant, and/or parent/branch vessel encroachment. The findings of the IA were recorded: residual aneurysm, vessel encroachment, and if IA led to clip adjustment. Other characteristics of the patients and their aneurysms were recorded such as rupture status, Hunt and Hess grade, Fisher grade, location, size, neck size, and presence of thrombus and/or calcification. Surgical details logged were the number of clips used, use of temporary clipping, intraoperative rupture, use of Charbel flow probe, and use of micro Doppler probe.
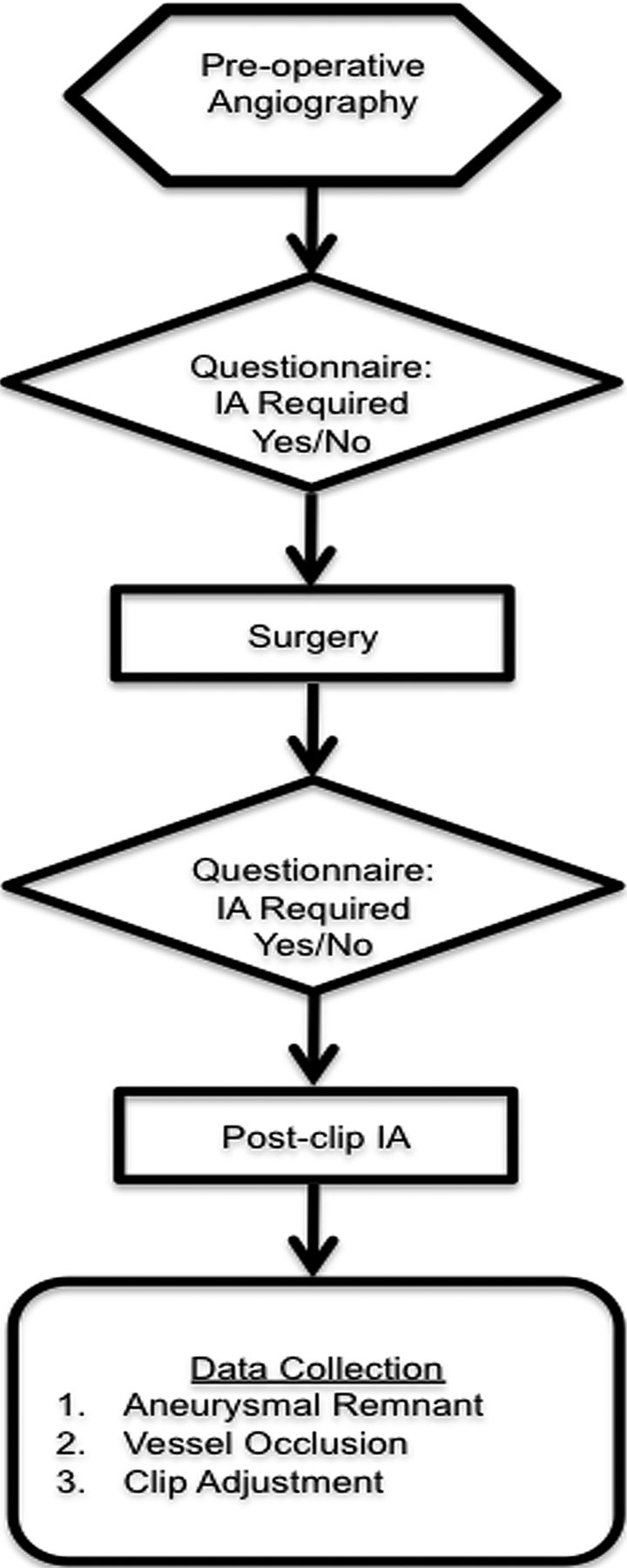
Flowchart demonstrating the study design. IA, intraoperative angiography.

{kind=link}
{kind=link}
Image of the questionnaire completed by the surgeon prior to surgery and immediately following clip placement but prior to intraoperative angiography.
Intraoperative angiography
We briefly describe the technique used for IA. For a more complete description, see Derdeyn et al.13 Typically, a 5 F sheath was placed in the right femoral artery either preoperatively or intraoperatively. The patient was then positioned on a radiolucent operating table (Skytron, Grand Rapids, Michigan, USA) using a radiolucent head holder (Mayfield Skull Clamp; Ohio Medical, Cincinnati, Ohio, USA) to fix the head. When the neurosurgeon felt the clip application was adequate, the neuroradiology team was called to the operating room to perform IA. A portable digital subtraction unit (OEC Diasonics, Salt Lake City, Utah, USA) was used for all studies. Views were obtained in at least three planes (anteroposterior, lateral, and oblique). Each set of images was obtained following arterial injections of contrast agent given by hand. Following image acquisition, the attending neuroradiologist interpreted the findings and compared them with the preoperative angiogram in consultation with the operating neurosurgeon.
Statistical analysis
Data from the questionnaires were collected and entered into a computer database. Analysis was completed using the statistical software package SAS V.9.1 (SAS Institute, Cary, North Carolina, USA). Outcomes assessed were: (1) rate of aneurysmal remnant, (2) rate of parent/branch vessel encroachment, (3) rate of post-IA clip adjustment, (4) rate of ‘missed’ positive IA findings based on the surgeon's preoperative evaluation, and (5) rate of ‘missed’ positive IA findings based on the surgeon's intraoperative appraisal.
Statistical analysis of these results included sensitivity, negative predictive values, and false negative rates of the neurosurgeon's preoperative and post-clip assessments regarding the need for IA. Preoperative and intraoperative factors were evaluated in an effort to determine which predicted the need for post-IA clip adjustment. Categorical variables were analyzed using the Fisher exact t test and continuous variables with logistical regression. Factors found to be significant in univariate analysis were inputted into a multivariate logistical regression model. The strength of association is reported using OR with 95% CI and associated p values, where p<0.05 is considered significant.
Results
During the enrollment period, 200 patients were entered into the study. A full complement of data was available for analysis from 197 patients. General characteristics describing the aneurysms and clinical presentation are shown in table 1. A total of 143 (72.6%) aneurysms were ruptured. Average size was 7.3 mm±5.6. Location breakdown was as follows: 64 (32.5%) pre-bifurcation internal carotid, 60 (30.5%) middle cerebral, 47 (23.9%) anterior communicating, and 26 (13.2%) other (ie, basilar, ophthalmic, internal carotid bifurcation).
Patient characteristics (n=197)
Preoperative assessment (table 2) deemed IA necessary in 144 (73.1%) cases. The most common reason was branch vessel involvement (45.2%), followed by location (37.6%), and size (22.3%). In 116 (58.9%) cases it was felt that post-clip IA was indicated (table 3). The most significant factors affecting this decision were a question of remnant (37.1%), branch vessel encroachment (25.9%), and parent vessel encroachment (21.3%).
Preoperative assessment (n=197)
Post-clip assessment (n=197)
Post-clip IA (table 4) demonstrated 47 (23.9%) positive findings, 29 (14.7%) residual aneurysms, and 18 (9.1%) occasions when a parent/branch vessel was compromised. These findings resulted in 19 (9.6%) cases where the permanent clip was adjusted.
Intraoperative angiography results (n=197)
In assessing the predictive capabilities of preoperative assessment, there were four cases where IA was deemed unnecessary, yet post-IA clip adjustment was required. For preoperative assessment, this results in a sensitivity 78.9%, negative predictive value of 92.5%, and false negative rate of 7.5% (table 5).
Comparison of preoperative versus post-clip assessments (n=197)
Regarding post-clip assessment, there were five cases where IA was thought to be unnecessary and clip adjustment was required (three residual aneurysms and two vessel occlusions). Sensitivity was 73% and the negative predictive value was 93.8% for post-clip assessment, with a false negative rate of 6.2% (table 5).
Univariate analysis found that neither preoperative patient characteristics nor surgeon opinion was significant in predicting the need for post-IA clip adjustment. Those factors found to be significant were presence of aneurysm calcification, use of >1 permanent clip, use of temporary clips, intraoperative aneurysmal rupture, and flow verification via Doppler probe (table 6). Entering these variables into the multivariate model, the only factor found to be an independent predictor of post-IA clip adjustment was use of >1 permanent clip, with an OR for clip adjustment of 4.8.
Factors predicting post-intraoperative angiography clip adjustment
Discussion
Any discussion regarding the benefits of a technique used in treating cerebral aneurysms must be prefaced with the goals of therapy. For surgery, the ultimate objective is to prevent future subarachnoid hemorrhage. This is more accurately described as reconstruction of the cerebral vasculature in such a way that blood flow in the aneurysm is stopped while maintaining flow through associated parent and branch vessels. In an effort to improve outcomes from this process, a number of tools have been developed.17 Of these, IA is considered by many as the ‘gold standard’ for post-clip assessment. Yet, given the relative infrequency in which IA leads to changes in surgical management, additional cost, and associated morbidity, it has been suggested that IA should be used on a selective basis.14 The purpose of this study was to prospectively evaluate the impact that a selective IA protocol would have on final clip placement by comparing results between preoperative and post-clip intraoperative assessments.
Selective versus routine IA
The issue of selective versus routine IA has been a persistent issue within cerebrovascular surgery. Klopfenstein et al6 attempted to resolve the question when they reported an intriguing prospective study examining the use of selective versus routine IA. In their study prior to surgery, the treating neurosurgeon preoperatively recorded whether IA would be necessary. All patients then underwent surgical aneurysm clipping followed by routine cerebral angiography. Changes in surgical treatment resulting from IA were compared with the surgeons’ preoperative predictions for the need for IA. In cases where angiography was felt to be necessary, clip adjustments were required in 17% of cases while in cases where angiography was thought to be unnecessary, clip adjustments were required in only 4%. The complication rate from IA was 0.5%. These authors concluded that their results support the routine use of IA, based on the low risk of angiography and the significant number of cases (even when angiography was predicted to be unnecessary) where surgical modifications were required. Similarly, Tang et al12 in a prospective evaluation of 517 aneurysms found that IA prompted change in 12.4% of cases with a complication rate of 0.4%. Popadic et al19 in their prospective evaluation of 126 patients found IA led to clip adjustment in 10.3% of cases and a complication rate of 0.8%. Again, they recommend routine use is warranted, based on the benefits of IA relative to the low risk.
Our study is the first of its kind to prospectively compare a surgeon's ability to assess the adequacy of clip placement with the ‘gold standard’ IA during surgery for cerebral aneurysms. The results demonstrate (as has been established in previous studies6 ,11–13 ,19) that IA provides useful information which allows for immediate changes in surgical management (9.6% in this series). These are similar to the findings from this institution by Derdeyn et al13 who found a 7.6% rate of clip adjustment following IA. However, surprisingly and somewhat disappointingly, the data also provide evidence that post-clip assessment provides no significant improvement in determining the need for IA compared with preoperative assessment (post-clip false negative rates of 7.5% compared with 6.2% in preoperative assessment). These facts, along with evidence from the literature, continue to support the use of routine IA.
Factors predicting the need for IA
The rationale for the surgeons’ preoperative and post-clip assessments are shown in tables 2 and 3. The preoperative decisions were driven primarily by branch vessel involvement (45.2%) and aneurysm location (37.6%). These factors persisted in the post-clip decision; however, the greatest concern was the possibility of an aneurysmal remnant (37.1%). It is interesting that none of these factors proved to be significant in predicting the need for IA. Yet it is clear that the surgeon's overall impression of aneurysm complexity was used in the decision process.
Previous studies have found aneurysm size to be a significant factor in predicting post-IA clip adjustment.2 ,12 ,14 ,20–23 Others have found location to be an important consideration when deciding on the need for IA. 11 ,12 ,14 ,19 ,20 ,22 ,23 This has consistently been shown for location such as middle cerebral artery trifurcation, anterior communicating complex, and basilar bifurcation. Beyond aneurysm characteristics, Nanda et al24 demonstrated that intraoperative rupture predicted the need for IA. Perhaps one of the largest and most comprehensive studies assessing this issue was presented by Le Roux et al.2 In their analysis of 543 diagnostic angiograms following aneurysm surgery on 494 patients, they found a 5.7% rate of both aneurysmal remnant and vessel occlusion. Predictors of remnant were atherosclerosis and multiple clip applications. Factors significant for vessel occlusion were atherosclerosis, temporary clips, multiple clips, and multiple clip applications.
Our findings add to these results by again demonstrating that intraoperative factors play a role in determining the need for IA (table 6). The results suggest that the decision is not simply a judgment based on aneurysm characteristics, but rather must be combined with the degree of surgical complexity (ie, multiple clips, temporary clips, and intraoperative rupture). Interestingly, the use of a microvascular Doppler probe was a significant predictor of post-IA clip adjustment. While others have found microvascular Doppler assessment to be useful in aneurysm surgeryv,17 ,25 our results are not consistent with these previous studies. Our hypothesis is that microvascular Doppler is insensitive to posterior wall remnants outside of the operative field of view and vessels receiving collateral or retrograde flow.
We acknowledge that the routine use of IA can be both technically and logistically challenging for many institutions. It adds to the operative time and, with complication rates reported as high as 3.5%,21 subjects patients to additional risks. However, we and other experienced centers have shown that IA can be accomplished with low complication rates, ranging from 0.99% to 1.5%.13 ,26 Based on the fact that IA demonstrated positive findings in 24% of cases and the need for clip adjustment in 10% of cases, it is our opinion that the additional costs and risks related to IA are justified. We believe that this is particularly true in today's environment where experience in open cerebrovascular surgery is declining while the complexity of clipped aneurysms is increasing.
There are limitations to the study. The most significant of these is the lack of routine ICGA, which has been shown to be useful in post-clip assessment during cerebral aneurysm surgery. 15 ,16 The study was initiated prior to our institution obtaining operating microscopes compatible with ICGA. However, from a subset of the current population, we have previously published (Washington et al18) our results comparing ICGA with IA and found a relatively high discordance rate of 14%. While it has since become routine in our aneurysm surgeries, we and others17 ,18 have found ICGA to have weaknesses and recommend against solely relying upon it. Additionally, our IA procedures were completed with a portable digital subtraction unit with acquisition of images in the anteroposterior, lateral, and oblique projections. We have previously shown that the false negative rate using this technique is 7%.11 This does not detract from our findings, but rather further emphasizes the need for a multimodality assessment. Also, as the prevalence of ‘hybrid’ operating rooms increases, with access to more accurate imaging including three-dimensional angiography, the benefit of IA will likely be even further increased.
Conclusions
This use of IA is, and will continue to be, a useful adjunct in the assessment of aneurysm surgery. Based on previous studies and those presented here, selective use of IA based on preoperative assessment results in an unacceptable number of unexpected findings. Furthermore, we have demonstrated that determining the need for IA post-clip does not improve accuracy sufficiently. From this, a rationale for selective IA use is not justified. We realize, however, that due to logistical issues, not all facilities are capable of routine IA for all aneurysm cases. Therefore, we strongly suggest that in cases with complex aneurysmal configurations, requirement of multiple clips, temporary clip usage, and intraoperative rupture, IA should be considered.
References
Footnotes
Contributors All authors participated in the following ways: substantial contributions to the conception or design of the work, or the acquisition, analysis, or interpretation of the data for the work; drafting the work or revising it critically for important intellectual content; final approval of the version to be published; agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None.
Ethics approval The study was approved by the institutional review board within the Human Research Protection Office at Washington University in St Louis.
Provenance and peer review Not commissioned; externally peer reviewed.