Article Text

Abstract
Background An accurate understanding of the morbidity and mortality associated with brain arteriovenous malformation (AVM) hemorrhage is important in determining the management of unruptured AVMs. Recent studies suggest this morbidity to be lower than assumed. We sought to perform a detailed critical assessment of the morbidity associated with ruptured brain AVMs.
Methods A retrospective chart review from a single-center tertiary care medical center was performed. Inclusion criteria were patients admitted with intracranial hemorrhage caused by a previously untreated AVM. Forty variables were analyzed including patient demographics, imaging findings, clinical course, and clinical examinations.
Results From 2008 to 2013, of the 51 patients who fit our inclusion criteria, we found admission National Institutes of Health Stroke Scale (NIHSS) scores of 0, 1–9, and ≥10 in 22%, 24%, and 55%, respectively. Hematoma location was parenchymal in 33%, intraventricular in 10%, subarachnoid in 4%, and combined in 53%. Deep venous drainage was present in 35% of cases and associated aneurysms were present in 37%. 43% underwent emergency hematoma evacuation while four patients died during their admission. Of those who survived, 74% had neurologic deficits upon discharge (NIHSS ≥1), with 25.5% of patients having a severe deficit (NIHSS ≥10). On follow-up, 55% were independent in their daily activities of living.
Conclusions Our assessment of morbidity associated with brain AVM rupture is higher than previously assumed and reported. These results should be further validated in a larger, more representative sample. An accurate understanding of the morbidity associated with AVM rupture is important as more patients with unruptured brain AVMs seek consultation.
- Arteriovenous Malformation
- Hemorrhage
- Vascular Malformation
Statistics from Altmetric.com
Introduction
Increasing availability and use of non-invasive brain vascular imaging has led to greater detection and more frequent consultations for unruptured brain arteriovenous malformations (AVMs). The optimal management of AVMs is becoming an increasingly important topic and an area of great controversy. The recently published and widely cited ARUBA study1 suggested that patients with unruptured brain AVMs should be treated conservatively with medical management. This conclusion was largely based on the higher than expected peri-procedural complication rate from the intervention group during the 33-month follow-up period. However, since its publication there has been controversy regarding its generalizability, short follow-up period, indiscrimination among different treatment modalities, low percentage of patients receiving microsurgical treatment, as well as a primary endpoint that overestimates actual clinically significant complication rates.2 ,3 An essential and often overlooked variable in managing the patient with an unruptured AVM is a detailed understanding of the morbidity associated with hemorrhage. Although much has been published on estimating the rate of AVM hemorrhage, fewer studies have looked specifically at the morbidity. Of the few studies focused specifically on this topic, the morbidity of AVM rupture has been suggested to be lower than previously assumed, with the large majority regaining functional independence.4 ,5 If this were the case, there would be even less justification for preventive interventional treatment for unruptured brain AVMs.
Our anecdotal perception of the morbidity of AVM rupture has been different. As a result, the aim of this study was to characterize in greater detail the morbidity and mortality of patients with ruptured brain AVMs and to compare our results with previously published series.
Methods
We performed a retrospective chart review from a single-center tertiary care urban referral academic center. Patients admitted with intracranial hemorrhage caused by a previously untreated AVM were included in the study.
Study subjects were identified using the international classification of diseases (ICD-9) code 747.81. All charts were manually reviewed via the electronic medical record system. Study subjects were selected if they had an intracranial hemorrhage secondary to AVM rupture. All AVM diagnoses were made on MRI and/or catheter cerebral angiography. A brain AVM was specifically defined as early opacification of a cerebral vein originating from a brain pial artery. Patients were excluded from the study if the etiology of their intracranial hemorrhage was not clearly related to the brain AVM or if there had been a prior attempt at endovascular or open surgical management of their AVM. Patients with vascular malformation types other than AVMs, such as dural arteriovenous fistulas or cavernous malformations, were excluded.
Forty variables encompassing imaging, clinical, and treatment data were analyzed. All imaging was independently reviewed by each of the authors. Admission non-contrast head CT was reviewed to determine the anatomic location(s) and maximal diameter of the hematoma. The location of the intracranial hemorrhage was recorded as parenchymal, intraventricular, subarachnoid or parenchymal+ (parenchymal hemorrhage with an intraventricular, subarachnoid, and/or subdural component). The presence of midline shift was recorded and defined from this scan as any distance between an imaginary reference line joining the frontal crest and the protuberantia occipitalis interna and the most shifted point of the septum lucidum. AVM angioarchitecture was determined by either catheter angiography if available or CT angiography. Deep venous drainage was defined as the existence of any nidal drainage into the deep venous system of the brain. Associated aneurysms included prenidal, intranidal, draining, and remote aneurysms.
Clinical measures included hematoma evacuation, which was defined as emergency hematoma decompression within 24 h of admission. Neurologic impairment and disability at admission and discharge was assessed by physical examination by a neurosurgeon or neurologist, usually with documentation of a National Institutes of Health Stroke Scale (NIHSS) score by the managing neurologist or neurointensive care unit nurse. Follow-up visits with a neurosurgeon or neurologist were used to determine a modified Rankin Scale (mRS) score.
Statistical analysis
ANOVA F-test, Student t test, and χ2 tests were used for all intergroup comparisons. Statistical significance was defined as a p<0.05. All analysis was done using Stata V.13 (Stata Corp, Texas, USA).
Results
Between 1 October 2008 and 1 May 2013 a total of 339 patients were admitted to our hospital with an ICD-9 code of 747.81. Of these, 51 patients (15%) presented with an intracranial AVM hemorrhage that fit our inclusion criteria (figure 1). Baseline demographic characteristics and past medical history are shown in table 1.
Patient demographics (N=51)

Selection criteria and process for study sample. AVM, arteriovenous malformation.
Hematoma features
The most common location of bleeding was parenchymal, which was present in 84% of patients. More than half of the patients (53%) presented with more than one hemorrhage type (table 2). The most common combination was intraparenchymal hemorrhage with intraventricular involvement. The average maximum hematoma diameter was 4 cm.
Anatomic location of intracranial hemorrhage (N=51)
Midline shift was seen in 21 patients (41%) while 22 (43%) underwent emergency hematoma evacuation. As expected, and seen in table 3, the proportions of patients with midline shift, more than one hemorrhage location, and those requiring surgical evacuation of their hematoma was significantly higher in the group presenting with an NIHSS score of ≥10 (p<0.05).
Demographic, AVM and outcome characteristics by level of presenting neurologic deficit
Presenting neurologic deficit
We found admission NIHSS scores of 0, 1–9, and ≥10 in 22%, 24%, and 55%, respectively. Table 3 shows demographic, hematoma, and angioarchitectural characteristics grouped by presenting deficit.
Angioarchitectural features
Angioarchitectural features were determined by catheter cerebral angiography in 47 cases and CT angiography in 4 cases. The mean (SD) maximum diameter of the AVM nidus was 2.5 (1.7) cm (range 0.5–8). In a quarter of our cases the AVM nidus was located in the posterior fossa; 35% of AVMs had deep draining veins. Among those 17 patients with deep venous drainage, 47% had both superficial and deep drainage. There were 19 patients with an associated aneurysm, 11 of which had either pre- or intra-nidal aneurysms and 8 of which had remote aneurysms. The percentage of those patients with an associated aneurysm was greatest in the group presenting with severe stroke (46%), although this difference was not statistically significant.
AVM interventions
During their admission 58% underwent AVM embolization, 43% underwent surgical resection, and 29% underwent both endovascular and surgical intervention.
Discharge outcomes
Four patients died during the admission and two (4%) went to a skilled nursing facility. The majority of patients (n=24, 47%) were discharged to a rehabilitation facility. Twenty-one patients (41%) were discharged home. Mortality and discharge to a skilled nursing facility or rehabilitation center was highest among the group that presented with a severe stroke at admission (table 3). According to the NIHSS score, there was an overall improvement in distribution from admission to discharge (table 4).
Comparison of admission and discharge National Institutes of Health Stroke Scale (NIHSS) profile
Follow-up outcomes
The mRS score at follow-up was determined for all 47 surviving patients with a mean (SD) elapsed time to follow-up of 5.6 (9.7) months (range 0.25–48). Twenty-one patients (45%) had a mRS score of ≥3. Multiple sites of intracranial hemorrhage were significantly higher in the group with a mRS score of ≥3 than in the group with a mRS score of ≤2 (80% vs 32%; p<0.01).
Discussion
This study of 51 consecutive patients admitted to our hospital with first time ruptured brain AVMs shows that the level of morbidity by clinical grading scales, imaging, and emergency procedures is higher than previously published. The majority of our patients presented with a NIHSS score of at least 10. We demonstrated a relationship between hematoma size, the presence of midline shift, and hematoma evacuation with clinical grade. There was an inverse relationship between the presence of deep venous drainage and clinical morbidity. No association was found between AVM nidus size, aneurysms, and clinical morbidity.
The majority of large series published over the past 30 years describing AVM rupture have focused on evaluating the risk of bleeding rather than the morbidity associated with bleeding.6–9 Of those that did study the morbidity, variable definitions of morbidity were used both in terms of definition and point in time ranging from ‘a fixed neurological deficit’ in the earlier studies to a mRS score of >2 in later studies. In the 1980s Ondra et al10 reported that 23% of 166 patients with untreated AVM developed major morbidity or death from hemorrhage. Also in the 1980s, Fults et al11 found a 40% mortality rate among 51 patients with ruptured AVM. In 1988 another report found that 23% of 168 patients with AVM developed severe disability and 29% died.12 More recently in 2002, 24.5% of 240 patients with AVM died from AVM hemorrhage and 27% had a mRS score of >2.13 It is difficult to determine the role any surgeries and/or interventions may have had in addition to the original pathology in contributing to the clinical outcomes.
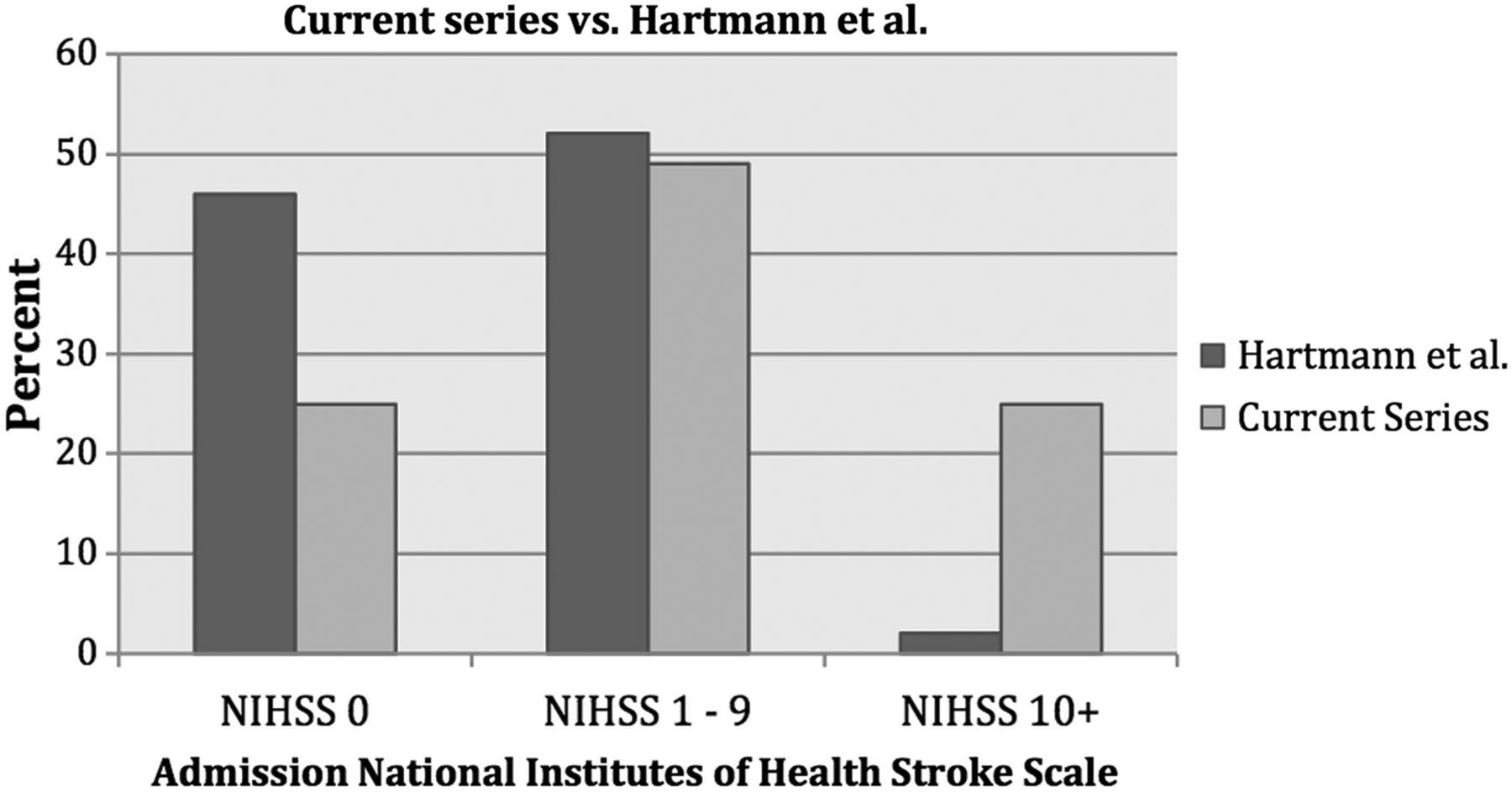
Only two serial studies from the same database at Columbia-New York Presbyterian have focused in more detail on characterizing the morbidity of patients with ruptured brain AVMs. They evaluated admission clinical grades prior to any interventions, as well as clinical grades at discharge and follow-up. However, their reports suggested a remarkably lower than previously reported level of morbidity. Hartmann et al5 evaluated a prospective consecutive cohort of 115 patients with incident ruptured brain AVMs and found that 47% of patients in their cohort presented without neurologic deficits and 84% of patients were independent in their daily activities of living on follow-up. As seen in figure 2, Hartmann et al's overall distribution of AVM rupture morbidity according to admission NIHSS score was 47%, 52%, and 2% for patients with NIHSS scores of 0, 1–9 and ≥10, which is very different from our results. A second study by Choi et al, using the same database as Hartmann et al, published 8 years later included more than double the number of subjects with incident AVM hemorrhages (n=241) and demonstrated a similar overall morbidity.4 Their overall distribution for NIHSS on admission was 61%, 31%, and 8% for patients with scores of 0–1, 2–9, and ≥10. Similar to the study by Hartmann et al, the majority of patients had a favorable NIHSS score on admission, with 61% having a NIHSS score of 0 or 1.

{kind=link}
{kind=link}
Comparison of admission National Institutes of Health Stroke Scale (NIHSS) profile with previous comparable published series.
As shown in table 5, our overall distribution of admission NIHSS scores reflected a higher level of morbidity associated with AVM rupture. There may be several reasons for the significant differences we saw in admission NIHSS scores and overall morbidity. First, the average age of our patients was 45 years compared with 37 years in the two Columbia studies. Our hemorrhage patterns also differed, which may explain some of the differences we saw in the NIHSS profiles. The rates of intraparenchymal, intraventricular, subarachnoid, and combined hemorrhage patterns in the study by Hartmann et al were 23%, 16%, 30%, and 31%, respectively, while ours were 33%, 10%, 4%, and 53%. In the study by Choi et al the hemorrhage location distribution was 71%, 14%, and 15%, respectively, for intraparenchymal, intraventricular and subarachnoid hemorrhage. For some reason they did not use a combined category. Nevertheless, they found parenchymal hemorrhage to be associated with an OR of 2.9 in predicting an unfavorable clinical outcome.4 Our cohort, which underwent independent head CT adjudication, had far more parenchymal hemorrhage patterns (86% in total) and much fewer exclusively subarachnoid hemorrhage patterns. Our results are consistent with this relationship between parenchymal hemorrhage and increased neurologic morbidity. A final possible explanation for the differences in our findings is that 17% of the 241 ruptured AVM niduses reported by Choi et al were located in the posterior fossa compared with 25% of our cases, and this is thought to be associated with greater morbidity and mortality. However, when stratified according to severity of neurologic deficits, we did not see a positive correlation.
Comparison of demographic, hematoma, angioarchitectural, and neurologic morbidity characteristics with previous comparable published series
What was more similar between our series was the finding of associated aneurysms. In the series reported by Hartmann et al and Choi et al, AVM-associated aneurysms were found in 26% and 31% of cases, respectively, compared with 36% in ours. Aneurysms in this context are generally regarded as sources of more severe hemorrhage and may therefore contribute to increased morbidity. Nevertheless, the overall numbers seem comparable between all series.
What has not been previously reported are hematoma sizes, rates of midline shift, and emergency hematoma evacuation. These adjunctive markers generally reflect the degree of initial neurologic injury. As such, nearly half of our patients had midline shift and underwent emergency hematoma evacuation, which further reflects the morbidity suggested by our admission NIHSS profile.
The average maximum hematoma diameter was significantly higher in those patients who were discharged with a severe stroke (NIHSS ≥10) than in the groups with mild to moderate stroke symptoms (NIHSS 1–9) or no stroke symptoms at discharge (p<0.05). Thus, hematoma size, midline shift and hematoma evacuation did demonstrate a linear relationship with worsening clinical NIHSS grade. In total, the combination of these clinical and imaging variables may capture the true morbidity associated with AVM rupture more accurately than previously published series.
Probably the most important and meaningful outcome measure is the level of disability after hospitalization. The majority of patients (51%) required further care with discharge to a rehabilitation or skilled nursing facility. At 30-day follow-up, favorable mRS scores of 95% and 72% were reported by Hartmann et al and Choi et al, respectively, while only 55% of our cohort were functionally independent at follow-up (table 5).
Another reason for the difference in our findings may be more historical. Previous series, albeit prospective, began enrolling patients as far back as 1987,5 which raises the question of the accuracy in using clinical scales such as the NIHSS. The NIHSS, designed primarily for ischemic stroke, only became widely used after FDA approval of intravenous thrombolysis in 1996. Furthermore, certification for the use of the NIHSS only began in the early 2000s. The majority of the NIHSS scores determined in the series by both Hartmann et al and Choi et al were probably pieced together using the physician's notes. Obtaining scores in this way may bias the data towards lower scores if there is not sufficient documentation. However, previously published studies have suggested that retrospective determination of NIHSS scores from physician charting is valid, including for those with severe stroke.14 ,15
The limitations of this study include our small sample size, particularly when compared with previously published studies. Additionally, as a tertiary care referral center that receives the majority of our admissions through hospital transfers as opposed to the emergency room, our patient population and therefore our overall results may be biased. We may simply have taken care of more severely affected patients because patients with slight symptoms may have remained at the original hospital. However, one might think that this particular bias would be comparable to series reported by most centers that care for many patients with AVM providing tertiary level care. At the same time, patients with truly devastating hemorrhages may not have been sufficiently stable for transfer in the first place. The degree to which these two biases potentially cancel each other out is unclear. Collaboration with several different centers from around the country would provide us with data and conclusions of greater validity.
Conclusion
Our detailed results indicate morbidity related to AVM rupture that is higher than previously published, with the majority of patients in this cohort presenting with severe neurologic impairment. Our NIHSS profile at admission and discharge, hematoma location and size, the rates of hematoma evacuation and midline shift as well as follow-up mRS score all suggest that AVM rupture may not be as benign as previously assumed and reported. An accurate understanding of the severity of the morbidity of AVM rupture should be considered alongside rupture risk and procedural risk16 when asked to consult on a patient with an unruptured brain AVM.
Acknowledgments
The authors acknowledge Shannon Sims MD and Lorenzo Munoz MD.
References
Footnotes
Contributors MM and MC contributed to the design, data collection, analysis and drafting of the manuscript. LAT contributed to the data analysis.
Competing interests None.
Ethics approval Ethical approval was obtained from Rush University Medical Center (IRB# 14042805-IRB01).
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The authors agree to share any data on request.