Article Text

Abstract
Background Experience with the endovascular treatment of cerebral aneurysms using the p64 Flow Modulation Device is still limited. This study discusses the results and complications of this new flow diverter device.
Methods 40 patients (30 women, 10 men) with 50 cerebral aneurysms treated in six Italian neurointerventional centers with the p64 Flow Modulation Device between April 2013 and September 2015 were retrospectively reviewed.
Results Complete occlusion was obtained in 44/50 aneurysms (88%) and partial occlusion in 3 (6%). In the other three aneurysms (6%), two cases of asymptomatic in-stent thrombosis and one intraprocedural occlusion of the parent vessel occurred. Technical complications were observed in eight procedures (16%). Permanent morbidity due to acute in-stent thrombosis and consequent ischemic stroke occurred in one patient (2.5%). No delayed aneurysm rupture, subarachnoid or intraparenchymal hemorrhage, or ischemic complications occurred and there were no deaths.
Conclusions Endovascular treatment with the p64 Flow Modulation Device is a safe treatment for unruptured cerebral aneurysms, resulting in a high rate of occlusion. As with other flow diverter devices, we recommend this treatment mainly for large-necked aneurysms of the internal carotid artery siphon. However, endovascular treatment with the p64 device should also be encouraged in difficult cases such as aneurysms of the posterior circulation and beyond the circle of Willis.
- Aneurysm
- Angiography
- Flow Diverter
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Introduction
Flow diverter devices (FDDs) are important tools in the treatment of intracranial aneurysms, with high rates of aneurysm occlusion and low rates of morbidity and mortality.1–4 They are becoming a suitable and, in selected cases, preferred alternative to traditional endosaccular treatment with coils. These new devices consist of a high attenuation braided mesh stent placed in the parent artery at the level of neck to disrupt the intra-aneurysmal flow and subsequently create intra-aneurysmal thrombosis; the exposed surface of the FDD also provides good support for the development of the neointima.5
FDDs have shown huge advantages in occluding difficult to treat aneurysms such as wide-necked, fusiform, or giant aneurysms, or those with complex morphology.6–17
Although the introduction of these devices is relatively recent, experience with their use is rapidly increasing. However, the choice of the best endovascular procedure and the indications for the use of FDDs are still a matter of debate.
Since the approval of the Pipeline Embolization Device (PED; Covidien, Mansfield, Massachusetts, USA) and the Silk device (Balt Extrusion, Montmorency, France), second-generation devices with different structures and delivery systems have been introduced. The recent literature mainly reports experience with the Silk6–11 and PED,12–17 while evidence for new devices such as the Flow Re-Direction Endoluminal Device (FRED; Microvention, Tustin, California, USA),18 ,19 Pipeline Flex (Covidien),20 Surpass (Stryker, Freemont, California, USA),21 and p64 (Phenox, Bochum, Germany)22 ,23 is limited and for newer devices such as Derivo (Acandis, Pforzheim, Germany) the experience is still preclinical.24
Understanding the safety and efficacy profiles associated with new FDDs in the treatment of intracranial aneurysms should therefore be considered.
We report a series of 40 patients with 50 aneurysms treated with the p64 Flow Modulation Device. This study discusses the results and complications of this new FDD.
Materials and methods
Study design
This study was designed to define the role of the p64 Flow Modulation Device in the endovascular treatment of cerebral aneurysms.
We retrospectively reviewed all cases of cerebral aneurysms that were admitted to six Italian neurointerventional centers between April 2013 and September 2015. Forty patients with 50 cerebral aneurysms treated with the p64 FDD were enrolled in the study.
Inclusion criteria were patient consent to the endovascular procedure and aneurysms that were difficult to treat with other standard endovascular techniques such as coiling because of the anatomical configuration.
All patients had complete pre- and post-procedural clinical and radiological data.
The radiological definition was obtained in 30 patients (75%) by CT angiography and in 10 (25%) by contrast-enhanced MR angiography (CE-MRA) using native images, two-dimensional multiplanar reconstructions, and three-dimensional volume rendering; digital subtraction angiography (DSA) was performed in all patients. The aneurysm location and size, aneurysm neck, and neck to diameter ratio were recorded. The aneurysm size was classified as small (<15 mm), large (16–25 mm), and giant (>25 mm).
The endpoints were angiographic evidence of complete aneurysm occlusion, recanalization rate, occlusion of the parent artery, and clinical and radiological evidence of brain ischemia.
The occlusion rate was evaluated according to the O'Kelly-Marotta (OKM) scale for flow diversion based on the degree of filling (A, total filling; B, subtotal filling; C, entry remnant; D, no filling).25
Patient characteristics
The 40 patients comprised 30 women and 10 men of median age 57 years (range 40–79 years). Thirty-five patients (87.5%) had unruptured aneurysms and five (12.5%) had ruptured aneurysms with previous subarachnoid hemorrhage (SAH). In the five patients with ruptured aneurysms the hemorrhagic episode occurred between 15 and 30 days before the FDD treatment. According to the Hunt-Hess classification, three patients were grade 1 and two were grade 1A (with third and sixth cranial nerve palsy, respectively).
Among the 35 patients with no previous hemorrhage, 15 (37.5%) complained of headache, 6 (15%) had cranial nerve palsies due to aneurysm compression, and 1 (3%) presented with pons ischemia due to a large basilar artery fenestration aneurysm and brainstem compression. Other unrelated symptoms were present in 13 patients (32%) (table 1).
Clinical and radiological characteristics in 40 patients with 50 aneurysms
Aneurysm characteristics
Among the 50 aneurysms, 43 (86%) were in the anterior circulation and 7 (14%) in the posterior circulation. The most common location (table 1) was the paraophthalmic internal carotid artery (ICA) (22, 44%) followed by the posterior communicating artery (PcomA) (10, 20%) and the cavernous ICA (7, 14%), with single cases of other locations.
Forty-six aneurysms were saccular and four were fusiform. Aneurysm size ranged from 2 to 26 mm (median diameter 9 mm). Forty-three (86%) were small, five (10%) were large, and two (4%) were giant.
The neck size ranged from 1.5 to 12 mm (average 5 mm). The neck to sac ratio ranged from 0.3 to 1 (average 0.8) (table 1).
Endovascular treatment and medication
The p64 FDD was the first and only treatment for 32 aneurysms (64%); in 9 (18%) the device was implanted in association with coils due to complex aneurysm morphology and size. Nine aneurysms (18%) previously treated by endovascular coiling (6, 12%), stenting with another FDD (1, 2%), or neurosurgical clipping (2, 4%) were retreated with the p64 FDD because of recanalization.
All patients with unruptured aneurysms were pretreated with 75 mg clopidogrel daily for 5 days together with 150 mg aspirin. Patients treated in the subacute phase of SAH received a loading dose of clopidogrel (600 mg) 4 hours before the procedure.
The thrombocyte inhibition test VerifyNow was performed in only 12 patients (25%) according to the single-center experience; no resistance to clopidogrel or aspirin was found. All patients had a continuous intravenous infusion of heparin during the procedure and a bolus of 1000 IU every hour during the procedure to maintain an activated clotting time of >250–300 s.
Clopidogrel (75 mg) and aspirin (100 mg) were administered daily for up to 6 months for anterior circulation aneurysms and up to 12 months for posterior circulation aneurysms, after which only aspirin was continued indefinitely.
All endovascular treatments were performed by six interventional neuroradiologists with more than 20 years’ experience in the management of cerebral aneurysms.
The procedure was performed under general anesthesia through catheterization of the right common femoral artery using an 8 F vascular sheath and a triaxial system. The p64 size was chosen according to the proximal parent vessel diameter, as is usual for other FDDs. The p64 was then placed at the level of the aneurysm and the correct apposition to the vessel wall was assessed by DSA and non-subtracted angiographic images. The procedure was considered successful if the p64 completely covered the aneurysm.
In 29 patients (72.5%) one device was deployed to treat a single aneurysm, and only in one case (2.5%) were two p64 devices used for the treatment of the same aneurysm (figure 1). The device was used to treat two contiguous aneurysms in 10 patients (25%).
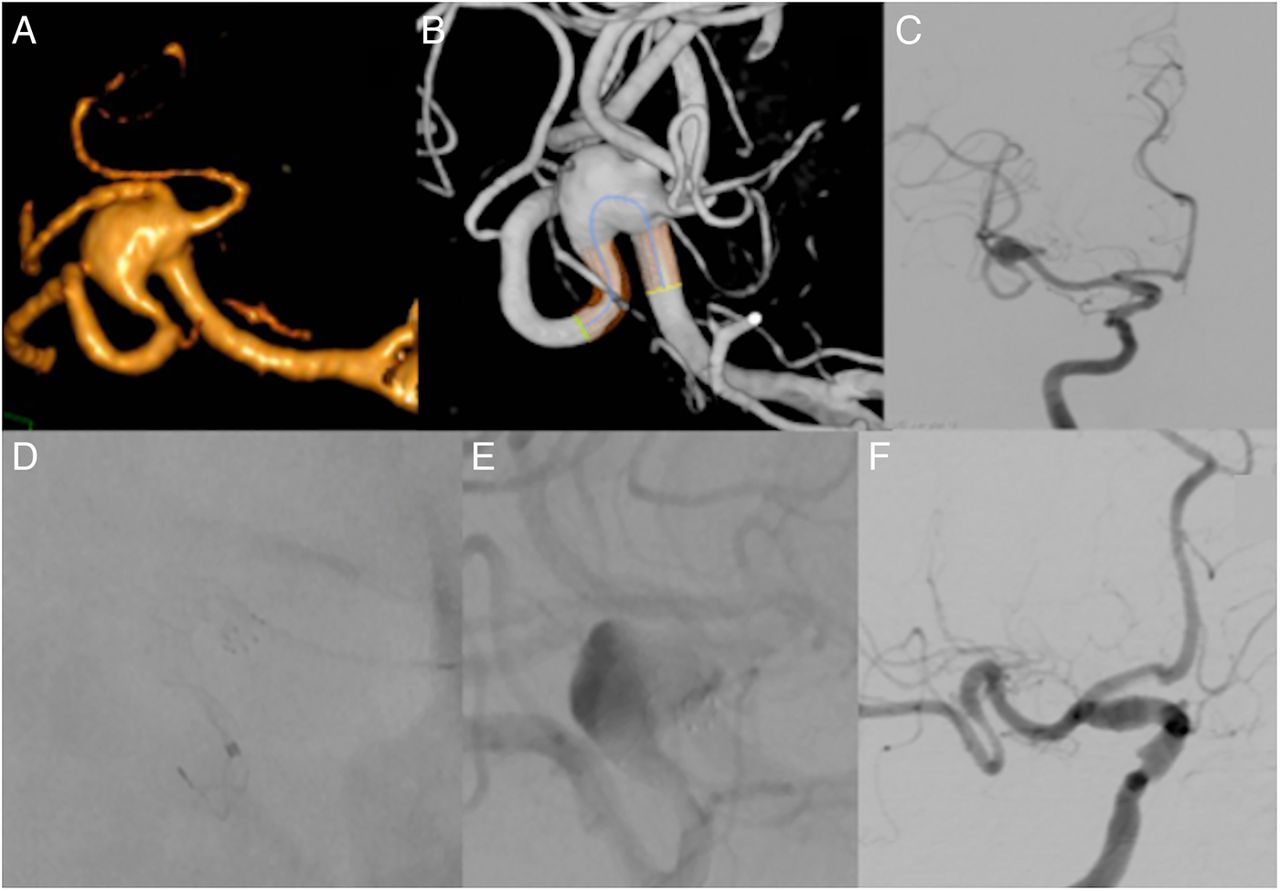
A 70-year-old man with a fusiform right middle cerebral artery aneurysm. (A) Pretreatment time-of-flight MR angiogram. (B, C) Pretreatment three-dimensional digital subtraction angiogram with flow diverter device length and size evaluation. (D) Deployment of two p64 flow diverter devices. (E) Angiogram at the end of the procedure shows immediate contrast stasis (F) Three-month follow-up angiogram after p64 placement shows complete exclusion of the aneurysm.
Retrieving and repositioning before detachment occurred in four procedures (10%).
Intra-aneurysmal contrast stasis was observed in all patients immediately at the end of the procedure.
Follow-up
The clinical neurological evaluation was performed immediately after the procedure, at discharge, and at 1, 3, 6, and 12 months.
Radiological examination by MRA was performed at 3–6 months and 12 months and until aneurysm occlusion was obtained; in all cases complete aneurysm occlusion was then confirmed by DSA. For patients with documented occlusion, follow-up with CE-MRA was performed every 12 months.
Actual follow-up ranged between 6 and 24 months (median 16 months).
Results
Peri-procedural technical complications
Technical complications occurred in eight procedures (16%); these included detachment failure in two cases, difficulty in deployment in two, cervical ICA dissection in one, and in-stent aggregation in three.
Detachment failure occurred in two patients. The first had a small PcomA aneurysm where the length of the device was underestimated; the initial device (3.5×12 mm p64) was therefore replaced with a longer one (3.5×18 mm) with a good final angiographic result. The second occurred in a patient with a large cavernous aneurysm. Owing to the tortuosity of the cavernous segment, the aneurysm was perforated by the microwire when attempting catheterization of the supraclinoid ICA with a consequent high-flow carotid–cavernous fistula (CCF). The patient was treated with parent artery occlusion due to good collateral circulation without clinical consequences.
In two patients with difficulty in deployment the microcatheter was pushed inside the p64 device to enable full opening of the device and to obtain better wall apposition.
One patient with dissection of the cervical ICA due to guiding catheter traumatism was successfully treated with a Carotid Wallstent (Boston Scientific).
In-stent aggregation occurred immediately after the procedure in two patients with a small A1/A2 anterior cerebral artery (ACA) aneurysm and in one with a previously ruptured fusiform PcomA aneurysm. An immediate bolus of tirofiban (Aggrastat) (25 μg/kg intravenously infused within 5 min) and a post-loading dose infusion (0.15 μg/kg/min intravenously for 18 hours) were administered which resulted in clinical and angiographic resolution in two cases and a permanent neurological deficit due to acute in-stent thrombosis and consequent ischemic stroke in another (2.5%).
No delayed aneurysm rupture, SAH, or intracerebral hemorrhage occurred and there were no deaths.
Neuroradiological outcome
All patients were followed up at 3–6 months; 34 (85%) were also studied at 12 months and 18 (45%) at 24 months (table 2).
Aneurysm occlusion data (50 aneurysms)
Complete occlusion (OKM D) was obtained in 44 out of 50 aneurysms (88%) and partial occlusion (OKM C) in three (6%); three others (6%) had occlusion of the parent artery. Among the three cases of partial occlusion (OKM C), one had an aneurysm of the A1/A2 segment of the ACA and a contralateral hypoplasic A1 which was considered as a functional side branch responsible for the partial occlusion; the two others were large aneurysms of the posterior circulation. Among the three cases of parent artery occlusion, two were intraprocedural (iatrogenic parent vessel rupture in one case and acute in-stent thrombosis in another) and one occurred at 3-month follow-up because of interruption of dual antiplatelet therapy (figure 2).
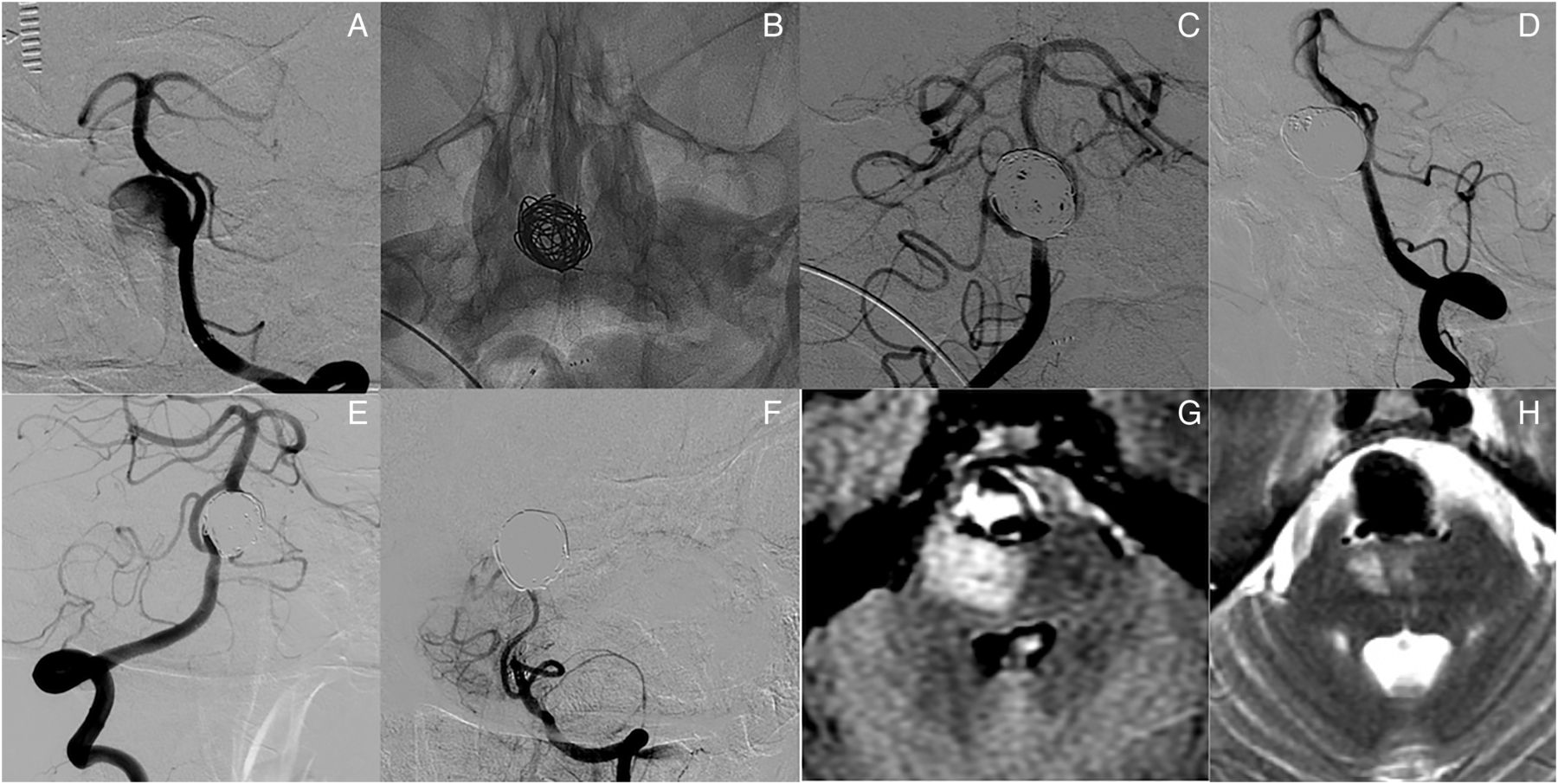
A 58-year-old woman with a large fenestration basilar artery aneurysm with compression on the brainstem. (A) Left vertebral artery angiogram. (B) Non-subtracted image shows fully opened p64 and coiling of the sac. (C, D) Early angiogram after deployment of p64 flow diverter device. (E, F) Three-month follow-up shows persistent occlusion of the aneurysm (E) but also in-stent thrombosis (F). (G, H) MRI before (G) and 3 months after (H) the procedure shows reduced compression on the brainstem.
Complete occlusion in 44 aneurysms (88%) occurred at 3 months in 30 cases (60%), at 6 months in 11 cases (22%), and at 12 months in 3 cases (6%) (figure 3).

{kind=link}
{kind=link}
{kind=link}
A 66-old-man with a large partially thrombosed aneurysm of the P2 tract of the right posterior cerebral artery. (A, B) Non-subtracted image (anteroposterior and oblique views). (C) Non-subtracted image showing deployment of the p64 device. (D) Three-month follow-up angiogram after p64 placement shows complete occlusion of the aneurysm.
Thirty-eight (96%) of the 40 implanted p64 FDDs were patent at the last follow-up.
Correlation of occlusion time with the aneurysm characteristics (table 3) showed a high prevalence of occlusion of small aneurysms at 3 months (68%), and no difference in occlusion time according to aneurysm size, neck, and neck to sac ratio.
Correlation of occlusion time with aneurysm size and neck (50 aneurysms)
Clinical outcome
One patient had permanent post-procedural morbidity (modified Rankin Scale (mRS) score 4) and another had an unchanged mRS score of 3.
The clinical conditions were stable with mRS score 0 in the other patients.
Discussion
The aim of treatment with FDDs is to disrupt the intra-aneurysmal flow and favor intra-aneurysmal thrombosis while preserving the patency of the adjacent vessels. The FDD mesh porosity and the pressure gradient between the parent artery and the aneurysm sac play a significant role in the aneurysm occlusion time; in the same way, it ensures the patency of the side branches covered by the FDD.
Flow diversion may provide a valid alternative to these more traditional endovascular techniques by preserving the parent artery while achieving high complete occlusion rates, as reported in large series and meta-analyses.1–4
Since the approval of the PED and Silk devices, new FDDs have been introduced in Europe. New devices such as the Pipeline Flex, FRED, and p64 have met the needs of second-generation devices. In particular, they have been structured to avoid mispositioning of the device and to reduce the associated complications, as reported in the first large multicenter study.12 The main characteristics of these new devices are an improved delivery system with easier and more precise deployment, mesh porosity for maintaining flow in branching vessels, good radio-opacity to confirm apposition to the vessel wall and avoid unwanted thrombus formation.
From a technical point of view, the p64 Flow Modulation Device is a braided mesh tube composed of 64 nickel-titanium alloy (nitinol) with radiopaque markers along the length of the device and eight proximal bundle markers. The device is compatible with a 0.027 inch internal diameter microcatheter. It is available in sizes of 2.5–5 mm diameter and 12–36 mm length (depending on diameter size). The ability to retrieve the device after complete deployment is a clear advantage; in fact, due to controlled mechanical detachment, the p64 can be retrieved into the microcatheter and removed or repositioned until 100% of its length has been extruded. Once a satisfactory position is obtained, the device is detached.22 ,23
The use of a device with 64 braiding wires instead of 48 with major metal coverage (defined as the ratio of the metal surface area to the total surface) and high pore density (defined as the number of pores per unit surface area) may lead to a higher rate of aneurysm occlusion. In our experience, among 88% completely occluded aneurysms, the higher percentage (82%) occurred until 6 months.
Experience with new FDDs such as the p64 is very limited, particularly regarding mid- and long-term follow-up. The only reported clinical series by Fischer et al analyzed the results of 121 patients with 130 aneurysms.23 As in our series, the main location was the ICA siphon (103/130, 79%), whereas aneurysm locations beyond the circle of Willis (14/130, 11%) and in the posterior circulation (10/130, 13%) were less common. At the final follow-up, 1.7% morbidity, 0.8% mortality, and 85.7% occlusion rates were reported.
In our series, complete occlusion occurred overall in aneurysms of the ICA siphon (37/ 39, 95%) and particularly in all the cases (100%) located at the paraophthalmic segment.
The results from aneurysms located at the cavernous segment are particularly encouraging with a high occlusion rate at the last follow-up (6/7, 85%) and no morbidity. Aneurysms at this location often present with cranial nerve palsies and are difficult to treat with other endovascular techniques. One multicenter study using PED and Silk devices reported a high mortality rate (4%) and recommended treatment of extradural cavernous aneurysms only if symptomatic and in expert hands.12 Comparing the occlusion rate of our study (85%) with the only series of cavernous aneurysms treated with the PED device (71%),26 p64 achieved a higher occlusion rate and no mortality or permanent morbidity. Furthermore, complete resolution or a significant improvement of symptoms occurred in all symptomatic patients. Aneurysms at other locations such as the posterior circulation and beyond the circle of Willis had a lower rate of complete occlusion (57% and 75%, respectively), which is similar to other recent series.27 ,28
With regard to aneurysm size, small aneurysms had a significantly higher occlusion rate at 3 months while giant ones, as expected, required a longer time (12 months).
With regard to previous treatments, all recanalized aneurysms after previous treatment such as coiling (12%), clipping (4%), or stenting with other FDDs (2%) were completely occluded at the 12-month follow-up. In fact, occlusion was achieved in almost all patients at 3 months (78%). The occlusion rate of recanalized aneurysms in our series is higher than in those treated with Silk and PED devices29 (100% vs 82.1%) and the permanent morbidity is lower (0% vs 6.9%). Thus, treatment with the p64 device should be recommended for recanalized aneurysms.
Complete aneurysm occlusion or reduction in size was achieved in 3/4 (75%) fusiform aneurysms, as in other large reported series.30
In-stent aggregations occurred in 2/3 A1–A2 aneurysms (66%), all of which resolved with intravenous tirofiban administration. The possible reasons for this need to be discussed. A major limitation of all FDDs is that they must be delivered through large profile 0.027 inch microcatheters. These represent a technical drawback due to the probable injury of the intima, especially for the treatment of aneurysms in distal locations such as beyond the circle of Willis. Moreover, in all cases the smaller available p64 (2.5 mm) was deployed in vessels of 2 mm, with consequent lengthening and major metal coverage of the vessel. These aspects probably led to turbulent blood flow within the device and subsequent platelet aggregation. The introduction of a new FDD with a smaller length and size and a smaller delivery microcatheter could reduce this complication.
Occlusion of the parent vessel was observed in 3/50 aneurysms (6%), a rate that is not negligible. These included a case of a previously ruptured fusiform PcomA aneurysm with homolateral posterior cerebral artery origin, a case of a large aneurysm at the fenestrated basilar artery treated by p64 and coiling in which the dual antiplatelet therapy was interrupted, and an ICA cavernous aneurysm where treatment with the p64 device was complicated by vessel perforation and CCF.
The occlusion rate, morbidity, and mortality have been reported in several recent studies of FDDs.
The experience with the p64 device shows a similar or even better profile with a high occlusion rate (88%), no mortality, and low permanent morbidity (2.5%).
Limitations of our study are its retrospective nature, the small number of included cases, the low rate of patients with 24-month follow-up (45%), the large prevalence of aneurysms of the ICA siphon (78%), and small aneurysms (86%). On the other hand, all patients were treated in centers with a large experience of endovascular treatment of brain aneurysms and were carefully followed up with adequate clinical and neuroradiological studies.
Conclusion
Endovascular treatment with the p64 FDD is a safe and effective treatment option for intracranial aneurysms and is associated with a high occlusion rate and low risk of complications.
As for other FDDs, we recommend this treatment mainly for large-necked aneurysms of the ICA siphon. However, the treatment of aneurysms of the posterior circulation and beyond the circle of Willis should also be encouraged.
The advantages of the p64 device over the other known FDDs include the 64 braided wires, 100% retrievability, mechanical detachment, and the absence of risk of mispositioning.
Further series with a larger patient population and longer follow-up will define the role of this device in the treatment of intracranial aneurysms.
References
Footnotes
Contributors FB designed data collection tools, monitored data collection, cleaned and analyzed the data, and drafted and revised the paper. He is the guarantor of the study. GL analyzed the data and drafted and revised the paper. LU monitored data collection, analyzed the data and drafted and revised the paper. MM, AM, LD, MR, NB and ID monitored data collection for the whole study and revised the draft paper. AM, MR NPN and MM designed data collection tools, monitored data collection, and revised the draft paper. FM, MM, PC, DS and FC analyzed the data and drafted and revised the paper.
Competing interests FB serves as proctor for Covidien. NPN serves as proctor for Sequent Medical, Covidien and as consultant for Covidien, MicroVention, Sequent Medical.
Patient consent Obtained.
Ethics approval All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or National Research Committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Participants gave informed consent for data sharing.