Article Text

Abstract
Background and purpose Intra-arterial therapy (IAT) is most effective when performed rapidly after ischemic stroke onset. However, there are limited performance benchmarks in IAT and there is a scarcity of information on how to structure an effective IAT protocol and its impact on time to treatment. The objective of our study was to detail a standardized IAT protocol, and to assess its influence on time to treatment in ischemic stroke.
Methods This was a retrospective observational study over 4 years at a comprehensive stroke center. A standardized IAT protocol was implemented in June 2013 that included pre-notifying the stroke team before hospital arrival, defining clinician roles, processing tasks in parallel, and standardizing IAT procedures. Three time metrics were examined and reported as median (IQR) minutes: arrival to CT imaging, CT to groin puncture, and puncture to recanalization. We compared these metrics in patients admitted before implementation (January 2012–May 2013) to patients admitted after (June 2013–December 2015) using Wilcoxon Mann–Whitney tests.
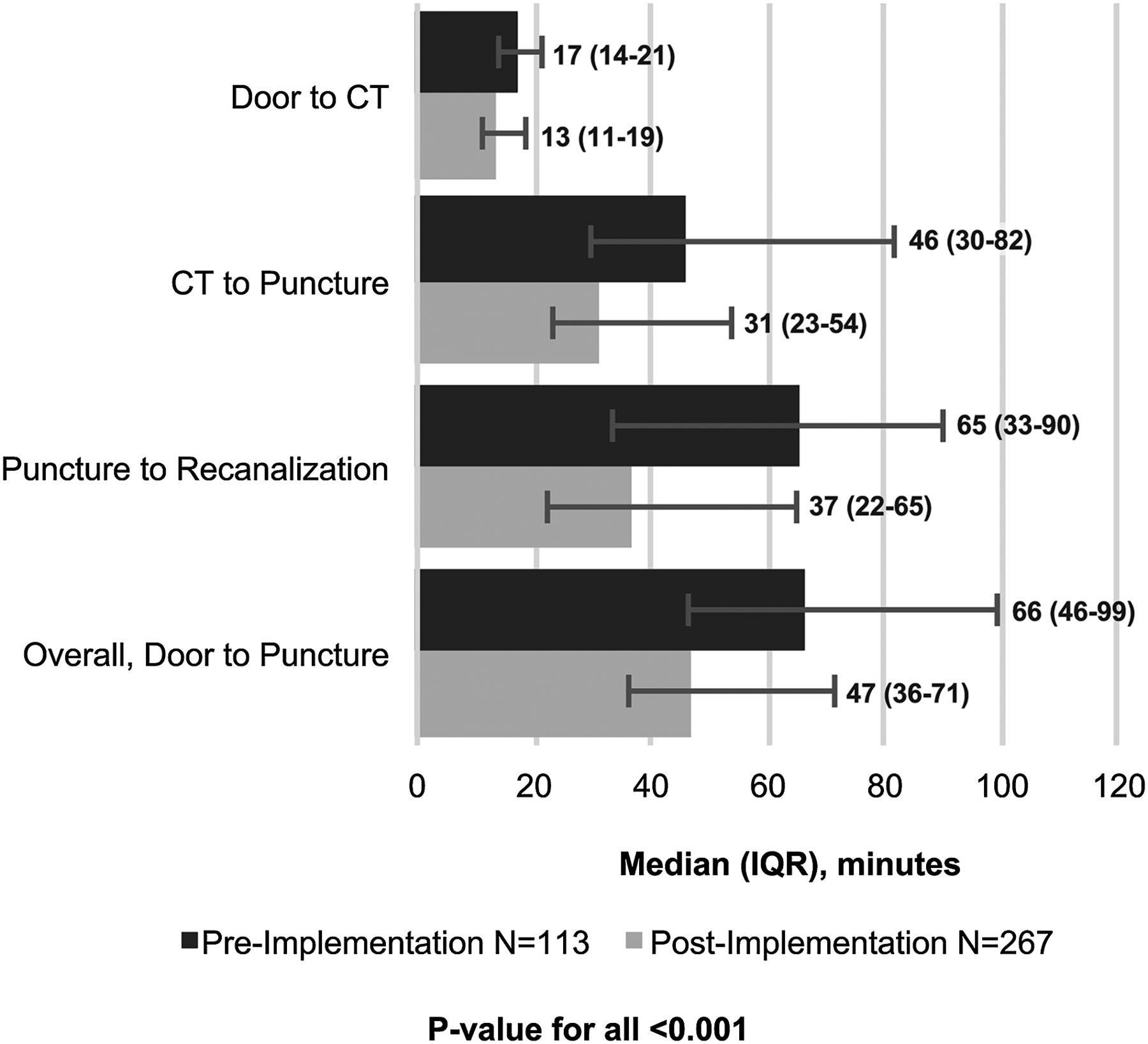
Results 380 patients were included. After the protocol was implemented, there were significant reductions in time from arrival to CT (17 (14–21) vs 13 (11–19) min, p<0.001), CT to puncture (46 (30–82) vs 31 (23–54) min, p<0.001), and puncture to recanalization (65 (33–90) vs 37 (22–65) min, p<0.001). 60% of time was saved during puncture to recanalization. Significant reductions in time were observed during both normal working hours and off-hours.
Conclusions Implementation of a standardized protocol resulted in a significant reduction in time to recanalization for patients with an ischemic stroke. A standardized IAT protocol decreases time to recanalization when team roles are clearly defined, tasks are processed in parallel, and procedures are standardized.
- Stroke
- Thrombectomy
- Intervention
Statistics from Altmetric.com
Introduction
Recent trials have established the clinical benefit of endovascular treatment for acute ischemic stroke (AIS) patients presenting with emergent large vessel occlusion (ELVO); every 30 min delay in recanalization reduces the average absolute rate of a good outcome by 11%.1–5 Additionally, these trials have confirmed the importance of rapid treatment, workflow, and efficient team based care for intra-arterial therapy (IAT) in AIS.1–5 The emphasis on workflow is driving stroke centers to explore methods for reducing the time from symptom onset to treatment.6–9 In 2011, the Brain Attack Coalition recommended door to treatment times of 2 hours as a benchmark for patients undergoing IAT.9 ,10 Using these guidelines, the Rapid Reperfusion Registry was developed to include patients at seven stroke centers who met this time window.11 Unfortunately, according to the registry, only 52% of all patients achieved an arrival to puncture time of 2 hours in 2012.11
Stroke centers must focus their efforts on the factors affecting treatment times. In 2015, the Society of Neurointerventional Surgery (SNIS) suggested several stroke process time metrics for implementation at comprehensive stroke centers (CSC).12 SNIS recommends time from door to interpretation of CT angiography (CTA) in <20 min, door to first groin puncture initiated in <60 min, and arrival to recanalization in <90 min.12 According to several studies, complying with these metrics requires optimization of triage strategies, including parallel processing, standardization of procedures, teamwork, and training.7 ,8 ,13 Evaluating and describing current procedures may help shed light on potential inefficiencies, improve workflow, and help minimize delays.7 The objective of this study was to detail a standardized IAT protocol, and compare treatment times and inhospital patient outcomes before and after its implementation.
Methods
This was a retrospective observational study including all consecutively admitted adult (≥18 years old) patients presenting with signs of an ischemic stroke to a CSC over a 4 year time frame (2012–2015). The inclusion criterion for this study was having a radiographically confirmed ischemic stroke followed by IAT. There were no exclusion criteria. The local institutional review board approved the study. The study was divided into two time periods: one prior to implementation of the standardized IAT protocol (January 3, 2012 to May 26, 2013), and the other after its implementation (June 1, 2013 to December 30, 2015).
On June 1, 2013, we underwent a series of three time saving process improvements (figure 1). First, when there was pre-notification of the arrival of a suspected ELVO ischemic stroke patient, the entire neurointerventional (NI) and stroke team (neurology, radiology, emergency medicine, and laboratory staff) received the estimated time of arrival (ETA) of the patient from the NI physician and were prepared and awaiting patient arrival 30 min beforehand. On arrival, the patient was brought to the stroke launch pad, an area located directly between the emergency medical service entrance and CT where, in parallel: (1) admissions’ personnel register the patient; (2) the emergency department (ED) physician obtains a National Institutes of Health Stroke Scale (NIHSS) score, brief history, and physical assessment; (3) the ED physician and neurologist determine the diagnostic imaging needed and imaging orders are entered by the ED physician; (4) the neurologist educates the family on diagnosis and procedures; (5) the ED technologist sends blood to the laboratory or draws blood on route to CT; and (6) the ED charge nurse and primary nurse document the NIHSS score, obtain vitals, and communicate with the CT technologist for expedited transport to the CT scan.
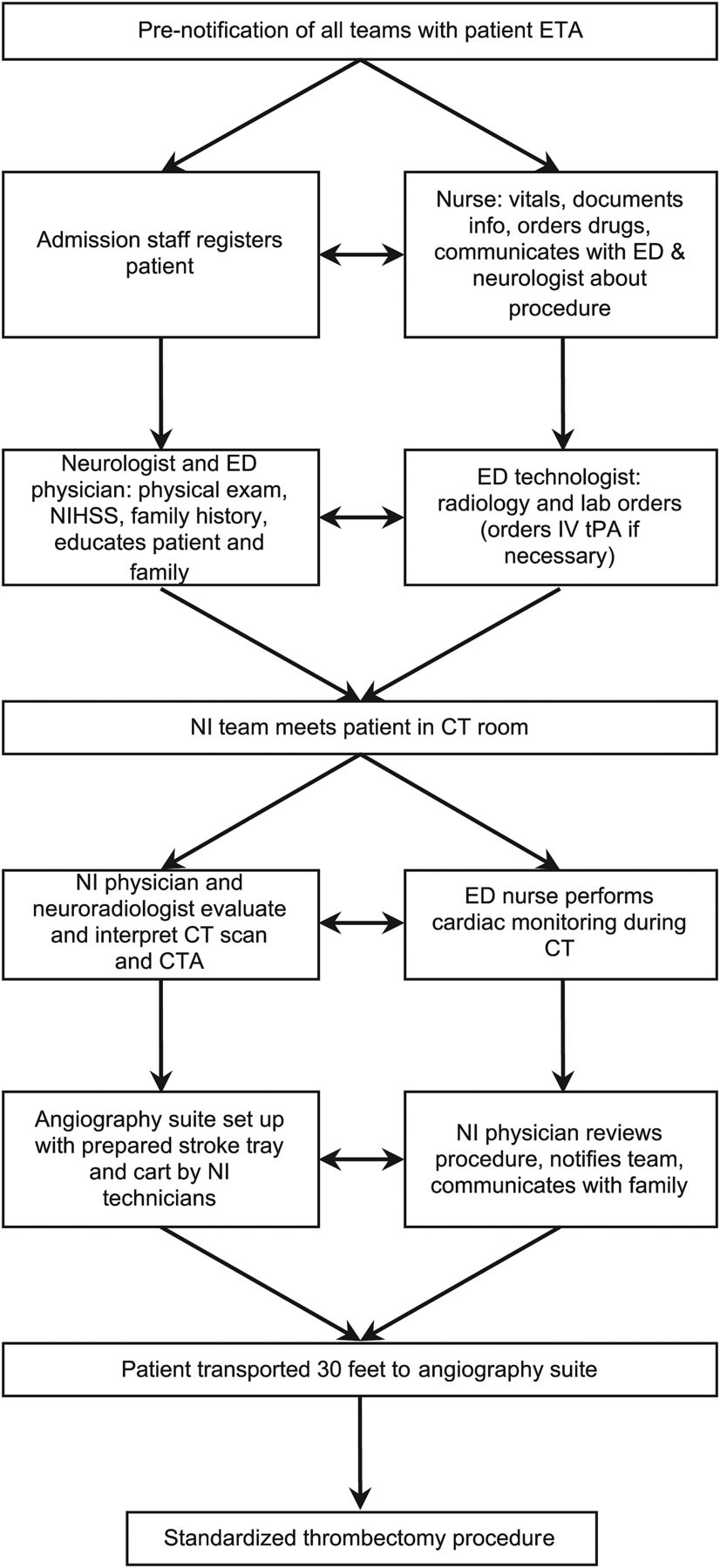
Flowchart of the standardized stroke protocol. Throughout the protocol, emphasis is on parallel processing, in which each team performs their task simultaneously with each other. CTA, CT angiography; ED, emergency department; NI, neurointerventional; NIHSS, National Institutes of Health Stroke Scale; tPA, tissue plasminogen activator.
The second process improvement was that the NI team, made up of the NI physician, anesthesiologist, nurse, and two technologists, was required to meet all arriving patients in the CT scanner room. This is always possible during weekday working hours and when patients are transferred to our CSC. In this circumstance, the stroke neurologist has already evaluated the patient and the non-contrast head CT (NCCT) via telemedicine, determined that the patient is likely to have a large vessel occlusion, and has notified the NI physician. The NI physician then meets the stroke team and the patient in the CT scanner room; this is approximately 120 feet from where patients first arrive in the ED at the stroke launch pad and 55 feet from the helipad elevator. In parallel, the anesthesiologist, the NI nurse, and the two technologists prepare the angiography suite for the potential thrombectomy procedure.
During CT imaging: (1) the ED nurse stays with the patient during the CT scan for cardiac monitoring; (2) the NI physician evaluates the CT scan and CTA of the neck and head contemporaneously from the CT scan monitor. If the NCCT shows a favorable Alberta Stroke Program Early CT (ASPECT) score and CTA shows a large vessel occlusion, the NI physician and the stroke neurologist decide whether to proceed with thrombectomy; (3) the diagnostic neuroradiologist calls the treating neurologist in the CT control room with a contemporaneous read of the NCCT so there is no delay in administering intravenous tissue plasminogen activator, if appropriate; (4) the NI physician notifies anesthesiology, the NI nurse, and technologists of the IAT case, and discusses the procedure with the patient and family; (5) a wheeled stroke cart, with all of the devices needed for the thrombectomy, has already been brought into the angiography suite and includes femoral artery access sheath, guide sheath, aspiration catheters, and stent retrievers (figure 2). A standardized stroke kit, BRISK (brisk recanalization ischemic stroke kit) is always ready in the angiography suite, which contains all of the other necessary items to perform the procedure. BRISK includes a micropuncture access kit, syringes, flush lines, sterile gauze, arterial line, and monitoring lines (figure 3).

Prepared stroke cart, with femoral artery access sheath, guide sheath, aspiration catheters, and stent retrievers.

BRISK with micropuncture access kit, syringes, flush lines, sterile gauze, arterial line and monitoring lines. BRISK, brisk recanalization ischemic stroke kit.
The third process improvement was standardizing the thrombectomy procedure as follows: (1) groins are not shaved prior to the procedure; (2) Foley catheters are not placed prior to the procedure; (3) conscious sedation (CS) rather than general anesthesia (GA) is used for all stroke patients, unless there is a concern regarding airway protection; (4) systolic blood pressure is maintained at approximately 185 mm Hg; the anesthesiologist uses Neosynephrine intravenously to maintain systolic blood pressure at 185 mm Hg before recanalization and Nicardipine intravenously to lower blood pressure to 140 mm Hg immediately after successful recanalization; (5) a 9 F femoral artery sheath (3 mm) is used for femoral artery access and allows for continuous arterial blood pressure monitoring, and a 6 F guide sheath (2.2 mm) is used for direct access proximal to the target artery; (8) a large inner diameter aspiration catheter that matches the occluded target vessel diameter as closely as possible (usually an ACE 64 catheter; Penumbra Inc) is advanced over an inner coaxial catheter (3 MAX; Penumbra Inc) and an 0.016 inch guidewire (Fathom; Boston Scientific) to the occlusion; (9) the inner coaxial catheter and guidewire are removed and the aspiration catheter is connected to an aspiration pump; and (10) continuous aspiration is performed for 2 min unless the clot is ingested. If there is no free flow in the aspiration tubing after 2 min, the catheter is slowly withdrawn and removed under continuous aspiration. When the aspiration catheter is near the guide sheath, suction is applied to the side port of the guide sheath with a 60 mL syringe. If Thrombolysis in Cerebral Infarction perfusion scale 2B/3 recanalization is not achieved after three aspirations, a stent retriever and local aspiration are implemented.
Outcomes
The primary outcome variables were times from door to CT (time from ED arrival to interpretation of the CT), CT to puncture (time from CT interpretation to puncturing of the femoral artery), and puncture to recanalization (time from puncturing of the femoral artery to recanalization or procedure termination). During imaging, CTs are interpreted contemporaneously. We also examined door to puncture time (time from ED arrival to puncturing of the femoral artery). Secondary outcome variables were in-hospital mortality and symptomatic intracranial hemorrhage rate (sICH), defined as any hemorrhage with neurological deterioration (change in NIHSS score ≥4).
Statistical analyses
Due to non-normal distribution of time intervals, data are presented as median (IQR). The Wilcoxon rank-sum and χ2 tests measured differences in categorical and ordinal variables. After protocol implementation, primary and secondary outcomes were compared between normal working hours (07:00–17:00, Monday–Friday) and off-hours (17:00–07:00 Monday–Friday and all hours Saturday–Sunday), as well as between transfer patients and direct admission patients using the Wilcoxon rank-sum and χ2 tests.
Stepwise multivariate logistic regression modeling was used to understand the impact of the protocol on inhospital mortality and sICH rates. The following covariates were available to the multivariate logistic regression model with an entry criterion of 0.20 and an exit criterion of 0.05: admission NIHSS, age, sex, race, inter-hospital transfer, and off-hours. SAS V.9.3 (SAS Institute Inc, Cary, North Carolina, USA) was used for all analyses. Two tailed tests with an α of 0.05 were used for all analyses.
Results
A total of 402 patients received IAT during the study period; 22 patients were excluded due to missing data. After exclusions, 113 patients were admitted before protocol implementation and 267 were admitted after its implementation. The baseline demographic characteristics of the patients before and after implementation were similar, showing no significant differences between the groups. There were also no significant differences between groups in symptom onset to arrival times or admission stroke severity (table 1).
Baseline characteristics among patients receiving intra-arterial therapy, pre-implementation versus post-implementation
There were significant decreases in median time in all treatment time intervals between the pre- and post-implementation groups (figure 4). These differences persisted during off-hours (table 2). There were no significant differences between normal working hours and off-hours, before versus after implementation.
Comparison of time intervals for normal working hours versus off-hours
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Impact of protocol implementation on each time interval, pre-implementation versus post-implementation. Median times are shown above the bars. The post-implementation period had a significantly lower median time in all treatment time windows (p<0.001 for all).
Each treatment time interval showed significant decreases for transfer patients between the pre- and post-implementation groups. Directly admitted patients showed no significant decreases in time intervals except for the CT to puncture time window (table 3).
Comparison of time intervals for transfer versus direct admission patients
After implementation of the IAT protocol, a significantly larger proportion of patients were recanalized within 30 min of femoral artery puncture. Before implementation, 21 (25%) patients were recanalized within 30 min of femoral artery puncture while after implementation, 83 (37%) patients were recanalized within 30 min (p=0.04) (table 4).
Proportion of puncture to recanalization time saved across pre- and post-implementation
A total of 69 (18%) patients died while in hospital but there were no significant univariate differences in the proportion of inhospital mortality between the pre- or post-implementation groups (21% vs 17%, p=0.33). After adjustment for admission NIHSS and age, there were no significant differences between the study groups in the odds of dying in hospital (AOR 0.63, 95% CI 0.32 to 1.12, p=0.15).
Overall, there were 18 (5%) patients who experienced sICH after IAT. There were no significant differences between the pre- and post-implementation groups in the rate of patients with sICH (7% vs 4%, p=0.16).
Discussion
Our data demonstrated that a standardized IAT protocol can significantly improve the treatment times for patients with ischemic strokes secondary to ELVO, while maintaining safety. In the United States, the average time from symptom onset to groin puncture is 6 hours, with an additional hour required for revascularization.14 According to the SNIS, CSCs should strive to start IAT within 60 min of arrival.12 Annual median data from our institution indicate that door to puncture times have been below the 60 min benchmark since 2012. The largest decrease in door to puncture times occurred after implementation of our revised IAT protocol in 2013, and showed an overall median (IQR) door to puncture time of 42 min (33.5–52) during normal working hours and 53 min (38–87.5) during off-hours.
Many factors in our study protocol aided in the prompt delivery of IAT; standardizing the thrombectomy procedure and parallel processing of tasks were the most important changes. Parallel processing and consistent support and participation from all team members have been described in numerous studies as important components of success in achieving rapid tissue plasminogen activator treatment times, and can also increase the rapidity with which IAT is delivered.7–12 ,15–20 According to the American Heart Association's Best Practice Strategies, the team based approach was associated with successful increases in the number of patients treated and reduction in the time to stroke treatment.10 Successful quality improvement protocols have also shown that processes must be performed simultaneously, not sequentially.16–20 Thus every process in our protocol was arranged so that each team had its resources in parallel with patient evaluation and treatment.
Furthermore, the use of CS versus GA during IAT may have helped reduce our time from puncture to recanalization. Several studies have suggested the use of CS in place of GA in order to reduce time to treatment, and also because of the potential risks associated with GA.21 ,22 Menon et al 22 reported that time from groin puncture to recanalization was 13 min longer in patients with GA versus CS. Abou-Chebl et al 21 showed that time to groin puncture was 10 min longer in patients with GA versus CS. Some of the arguments against CS for IAT patients is that patient movement during the procedure can lead to complications, resulting in longer procedure times and delayed time to recanalization.22 However, implementation of CS in our standardized thrombectomy procedure did not result in additional risk while puncture to recanalization times decreased significantly.
Our stroke center also participated in two studies that incorporated newer technology and endovascular techniques for AIS patients to improve time metrics, outcomes, and recanalization rates.23 ,24 The first study by Humphries et al 23 (August 2012–April 2013) demonstrated the efficacy and safety of using newer manual aspiration and stent retrievers for endovascular recanalization among six different stroke centers. Humphries et al used the Solitaire (EV3 Neurovascular, Irvine, California, USA) and Trevo (Stryker Neurovascular, Freemont, California, USA) stent retriever devices, followed by the Penumbra system distal access catheter, and observed a puncture to recanalization time of 57.3 (11–240) min (median (IQR)).23 The second study, ADAPT Fast (2012), used a new thrombectomy technique in which patients underwent a direct aspiration first pass technique with a large inner diameter aspiration catheter, usually a 5MAX or 3MAX (Penumbra), with a 0.016 inch microwire (Fathom, Boston).24 ADAPT showed an average time from puncture to revascularization of 31.6 (23.3) min from the same six stroke centers when the aspiration complement of ADAPT was successful as a standalone technique.24 Participating in the previous studies allowed us to incorporate more efficient techniques and technology, which we utilized in our thrombectomy procedure. These changes may have helped contribute to our post-implementation puncture to recanalization time of 37 (22–65) min (median (IQR)), while maintaining a low rate of sICH.
While recent studies have suggested the use of newer imaging technology such as cone beam CT perfusion or multiparametric CTA in order to improve time from stroke onset to endovascular revascularization, or to rapidly improve hemorrhage visualization,25–30 our study used CTA and NCCT. We believe that cone beam CT imaging does not accurately represent gray white matter differentiation. Additionally, studies exploring the use of these imaging techniques have reported inconsistent outcomes and warrant further study.25–30 Our protocol used standard CT imaging and we found significant time saving, without sacrificing patient safety.
Several studies have demonstrated that rapid IAT protocols decrease treatment times for patients with ischemic strokes.16–20 However, these studies did not achieve time savings similar to those reported in our current study.16 ,18–20 Mehta et al 16 reported a median (IQR) door to puncture time of 107 (87–124) min post quality improvement protocol. In addition, Rai et al 20 demonstrated a mean (SD) door to puncture time of 75 (18) min post quality improvement protocol. Our pre-implementation median door to puncture time was 66 min and decreased to 47 min post-implementation. Both of these previously mentioned studies applied lean methodology in order to eliminate wasteful steps, create an action plan to implement a new protocol, and continuously evaluate changes made. Lean methodology helped to establish an early NI activation system, including preparing the angiography suite in advance and clearly defining clinician roles.16 ,20 Early activation allowed them to reduce time from CT to angiography suite or door to puncture through parallel work of various team members.16 ,20 Additionally, the previously mentioned studies used GA (which also included placement of a Foley catheter) and did not discuss how their process improvements affected the puncture to recanalization time window.16 ,20 Our data demonstrate that 60% of all the time saved in our study was attributable to standardization of our thrombectomy procedure.
Many rapid stroke protocols compare normal working hours versus off-hours as a way to evaluate imbalances in delivery of care.16 ,18 ,20 ,21 In comparison with other studies, our off-hours arrival to treatment times were shorter.16 ,18 ,20 ,21 Rai et al 20 reported a post-quality improvement mean (SD) arrival to puncture time of 108 (42) min during off-hours. Mehta et al 16 identified patient presentation during normal working hours as an independent predictor of decreased arrival to puncture times because of delays from on-call staff during off-hours. Although our center benefited from an inhouse neurologist 24/7, as well as a 24/7 inhouse anesthesiologist, the technologists and nursing staff were on-call for a majority of off-hours. All time intervals were improved during all hours of work because delays were rare from on-call staff, and the rapid IAT protocol ensured every patient was treated consistently. Because a majority of our patients were transferred in from other hospitals, we had the benefit of knowing the ETA of the incoming patient and could insure the on-call team arrived before the patient arrived.
Despite significant decreases in treatment times, our study found no significant differences between treatment periods for inhospital mortality at discharge. Moreover, standardization of our protocol allowed us to meet aggressive CSC time benchmarks while reporting a low rate of sICH. Thus our protocol was associated with significantly decreased treatment times during all hours, while maintaining patient safety and low mortality rates.
There were several limitations to our study. These data come from a single comprehensive stroke center and are not generalizable to all stroke centers. It may be challenging for smaller scale stroke centers to implement a rapid IAT protocol that requires the entire stroke team to be brought in for each possible stroke case. Additionally, because of the small sample size of our direct admission patient group, we did not have the power to detect significant time savings. A power analysis revealed these statistical tests had an average of 30% power to detect a difference between times in direct admission patients. Finally, we did not have a randomized control group and thus we cannot establish causality between our intervention and the decreased treatment times observed.
Conclusions
Our results emphasize the importance of time saving protocols and their application to IAT. After standardizing our IAT treatment protocol, we observed significant reductions in treatment times during normal working hours and off-hours. If a stroke center is not able to implement the entirety of our rapid IAT protocol, at a minimum they will be able to understand how each element in our protocol contributed to decreasing treatment times. Focusing on these time metrics may help stroke centers improve IAT treatment time metrics and reduce delays during all hours.
References
Footnotes
Contributors All authors gave final approval of the published version and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Specifically, DF contributed to conception and acquisition of the data and critical revision. CM contributed to data acquisition, conception, and design, analysis and interpretation of the data, and drafting the manuscript. KM contributed to acquisition of the data and critical revision. MW contributed to acquisition of the data and critical revision. RJB contributed to critical revision. DL contributed to critical revision. JW contributed to critical revision. AO contributed to acquisition and interpretation of the data, drafting the manuscript, and critical revision. DB-O contributed to interpretation of the data and critical revision.
Competing interests DF is a consultant for Penumbra, Covidien, Microvention, Siemens, and Stryker. JW is a speaker for Genentech. MW was on the Activase Speakers Bureau in 2015; was a consultant for Clinical Data Management in 2015; and was a consultant for Lombardi Hill 2015-current. RJB was a speaker for Penumbra.
Ethics approval The study was approved by the local institutional review board.
Provenance and peer review Not commissioned; internally peer reviewed.
Data sharing statement Anonymized data and statistical code are available from the corresponding author.