
Abstract
Background
Sacral insufficiency fractures (SIFs) are often overlooked in elderly patients presenting with low back and pelvic pain following no or minimal trauma.
Objective
The aim of this review is to raise awareness and outline the clinical presentation, methods of diagnosis and treatment of SIFs.
Discussion
Insufficiency fractures represent a special category of stress fractures that occur in bones with reduced mineral content and elastic resistance. SIFs, a well-defined subgroup of the latter group, are not uncommon, but lack of clinical suspicion results in many being undiagnosed. SIFs are set to become an important clinical entity of both social and economic significance as the Western population ages. Subtle clinical presentations and signs coupled with radiographic findings that can mimic other unrelated or overlapping conditions, such as sacroiliac joint infection, spinal stenosis and metastatic bone disease, often make SIF diagnosis a challenge. The aim of this review is to increase awareness among clinicians, highlighting SIFs as an important differential diagnosis to be considered when patients present with low back and pelvic pain and subsequently allow prompt management. The paper provides an overview of epidemiology, anatomical considerations, relevant pathophysiology and risk factors, presenting symptoms and signs, investigations and imaging techniques, differential diagnoses and current treatment methods available for the management of SIFs.
Similar content being viewed by others


Epidemiology and cost of care
Osteoporotic fractures of the pelvic ring are not uncommon; however, they have been largely unrecognised, as until recently there was only scarce information in the literature. Data presented from the Finish computer-based population register have shown that the incidence of osteoporotic pelvic fractures requiring admission to hospital in Finnish women 60 years of age and older rose significantly between 1970 and 1997—from 20 to 95 per 100,000 people, respectively [1]. Furthermore, in a follow-up study by the same group of investigators, the number of pelvic fractures occurring following a minor trauma in the highest risk group among women aged 80 years or older also increased—from 35,421 in 1970 to 134,727 in 2002 [2]. A gross calculation estimated that the numbers will tripple by the year 2030 [2]. The latter conclusion, however, may be attributed to the current raised awareness of osteoporotic pelvic fractures and advanced radiological methods for their investigation and also to the fact that the mean age of patients increased from 74 years in 1970 to 80 years in 1997.
Sacral insufficiency fractures (SIFs) are a well-defined subgroup of insufficiency fractures. Since their original description by Lourie [3] in1982, several case reports and short case series have been published [3–54] stressing the subtle clinical and radiological features associated with these fractures (Table 1). The incidence of SIFs remains unknown; however, it is apparent that SIFs are more common than widely appreciated and remained largely overlooked as a cause of pain and disability within elderly and other at-risk populations. The potential prevalence of SIFs within the general population was, however, highlighted by Weber et al. in 1993 [26] following a 2-year prospective study. They found the frequency of SIFs in women aged over 55 years who presented to hospital with low back pain to be 1.8%.
Financial costs associated with SIFs remain unknown. Data related to potential costs involved comes from a 5-year retrospective study in the UK by Dasgupta et al. [55] who reported seven out of ten patients with SIFs required on average 20 days inpatient care at a cost comparable to that of a femoral-neck fracture. Total cost associated with the patient’s hospital admission and subsequent care will, however, depend on the country of residence, the mean length of stay and the intensity of rehabilitation.
Sacral anatomy and fracture classification
The sacrum is a triangular bone formed by the fusion of five separate vertebrae that articulate superiorly with the fifth lumbar vertebra and inferiorly with the coccyx. The sacrum is comprised of the body, the sacral ala with the two lateral masses and the sacral foramina. The lateral ear-shaped surface of the upper part of the lateral masses, called the auricular surface, articulates with the ilium to form the pelvic ring.
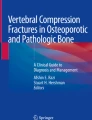
Currently, there is no classification system to describe SIFs; however, Denis et al. [56] classified traumatic sacral fractures according to their location into three discrete zones (Fig. 1). The Denis classification system, although not directly related to SIFs, remains a useful tool for their description since it presents fracture location in relation to potential complications. According to the Denis classification, zone 1 fractures involve the sacral ala, which is lateral to the sacral foramina and the central sacral canal. Fractures here are rarely associated with neurological deficits, but damage to the lumbosacral nerve roots may occasionally occur [57]. Zone 2 fractures involve one or several sacral foramina but do not enter the central sacral canal. These fractures are associated with unilateral lumbosacral radiculopathies. Zone 3 fractures occur through the body of the sacrum and involve the vertical and transverse central canal. Significant bilateral neurological deficit frequently associated with saddle anaesthesia and loss of sphincter tone is common in zone 3 fractures. Injuries in this region have the highest incidence of cauda equina.

Denis classification of sacral fractures [56]
The vast majority of SIFs occur in zone 1 [57]. The fractures run vertically, parallel to the sacroiliac (SI) joint, approximately in line with the lateral margins of the lumbar vertebrae and the vertical loading axis. Severe stresses maybe associated with an additional transverse fracture extending to the sacral body [57].
Pathophysiology and risk factors
SIFs are frequently bilateral and arise predominantly in the sacral ala parallel to the SI joints. Most SIFs are related to simultaneous further fractures of the pelvic ring. Biomechanical failure of the pelvic ring leads to increased instability and induces stresses at the SI joints, subsequently resulting in failure of the osteoporotic sacrum [6].
The majority of SIFs (over 90%) occur in elderly women [24, 35, 45]. SIFs often arise insidiously, resulting from axial stresses transmitted from the spine to a sacral ala with deficient elastic resistance [30, 58]. It is common for a patient to present without prior history of trauma, detracting clinicians from the diagnosis of fracture. Finiels et al. (1997) [59] conducted a meta-analysis of 493 SIFs from the literature along with an analysis of 15 SIFs from their own unit and stated that the majority of SIFs affected women over 60 years of age and that a history of trauma was often not identified in two thirds of the patients.
Several conditions may compromise bone density and strength, predisposing patients to SIFs—postmenopausal osteoporosis being the main cause among them. Corticosteroid-induced osteopenia and radiation therapy are also implicated as common risk factors for SIFs (Table 1). Secondary osteoporosis, however, is equally an important predisposing risk factor and should alarm the clinicians. Several pathological entities superimposing or being the underlying cause of osteoporosis may be involved, including hyperparathyroidism [60], osteomalacia, renal osteodystrophy [40, 61], lumbosacral fusion [51], Paget’s disease [16, 33], reconstructive surgery of the lower limb [7, 35] and transplantation of lung, heart-lung [39], kidney [45] and liver [62, 63]. Moreover, rheumatoid arthritis increases the risk of SIFs due to generalised osteopenia attributed to the corticosteroid therapy and the reduced mobility secondary to the disease as well as joint deformities [31]. Although osteomalacia is rarely seen in the developed world given that diet is usually fortified, the less-sever vitamin D insufficiency is, however, quite common within elderly population and predisposes to insufficiency fractures. Poor dietary intake and reduced gut absorption contributes to the development of vitamin D deficiency, but a combination of reduced functional capacity of the skin to synthesise vitamin D and inadequate sunlight exposure are the predominant reasons [64]. Vitamin D insufficiency causes secondary hyperparathyroidism, high bone turnover, bone loss and mineralisation defects, thereby contributing to the pathogenesis of fractures [65].
SIFs have also been reported to result from transient osteoporosis associated with pregnancy and lactation [38, 39, 66–68]. These fractures were, however, not accurately classified as insufficiency fractures but rather as stress fractures attributed to abnormal loading of transiently abnormal bone. Four types of pregnancy-related primary osteoporosis have been described: idiopathic osteoporosis of pregnancy, transient osteoporosis of the hip, postpregnancy vertebral osteoporosis and lactation-associated osteoporosis [69]. Hyperparathyroidism also associated with pregnancy could be a cause of secondary osteoporosis [60]. It has been shown that bone mineral density (BMD) reduces during pregnancy by a average of 3.5% [70]. This fall in BMD, attributed primarily to prolactin-related osteopenia [71], coupled with biomechanical alterations in sacral axial loading due to hyperlordosis [72], relaxin-related loosening of pelvic ligaments [73] and the gaining of body weight as well as insufficient maternal calcium intake [74], may contribute to the pathogenesis of SIFs in pregnant women.
Clinicians should maintain a high index of suspicion for patients presenting with sudden onset of low back and pelvic pain without trauma who are at risk of osteopenia attributed to all causes presented above.
Clinical presentation and physical examination
The clinical presentation is often variable, which often detracts from the diagnosis. Prominent features include sudden insidious, intractable, low back or pelvic pain coupled with a significant reduction in mobility and independence. Symptoms are exacerbated by weight-bearing activity and generally improve with rest. Patients are often most comfortable in a supine position. An initial history should ascertain previous activity levels (intensity, duration, recent changes) and any relevant risk factors for insufficiency fractures (osteoporosis, previous osteoporotic fractures, pelvic irradiation, prolonged corticosteroid treatment, cancer and other comorbidities such as rheumatoid arthritis). The predominant presenting symptom is pain, which may be severe and radiate to the groin, low back, buttocks, and thighs. SIFs are often associated with pubic rami fractures and present with tenderness over the parasymphysial area. The patient in such cases may recall a low impact trauma that subsequently resulted in major mobility restriction or even confinement to bed.
Physical examination may reveal sacral tenderness on lateral compression. SI joint tests, although not specific for SIFs, are often positive. Hip flexion-abduction-external rotation (FABER) test, Gaenslen’s test and squish test are all described in Table 2. Gait is usually slow and antalgic [57]. Trendelenburg test and sciatic nerve tension tests (Lasegue test and straight leg raise [75]) are usually normal [18, 61]. Neurological examination is often unremarkable. Nerve root compromise is uncommon but may present with sphincter dysfunction and lower-limb paraesthesia [18, 76]. The clinician should be aware of SIFs and vertebral osteoporotic fractures as a cause of neurological impairment in elderly patients with other comorbidities.
Laboratory investigations
Bone alkaline phosphatase (ALP), a marker of bone formation, can be a useful adjunct in directing the clinician towards a diagnosis of SIFs, particularly when early radiographs are inconclusive. Serum levels of ALP are often slightly raised.
Osteoporosis in the elderly is usually primary; however, reversible causes of secondary osteoporosis such as hyperthyroidism, hyperparathyroidism, osteomalacia or hypogonadism must be investigated, especially in men and younger patients who are not expected to present with primary osteoporosis. Levels of thyroid-stimulating hormone (TSH), parathyroid hormone (PTH), calcium, phosphorus, albumin, 25-hydroxyvitamine D, urinary calcium, creatinine, full blood count, liver function tests, C-reactive protein (CRP), erythrocyte sedimentation rate (ESR) and, if indicated, serum and urine protein electrophoresis can facilitate differential diagnosis of secondary osteoporosis. Osteocalcin, a bone matrix protein, is a useful biochemical indicator of high bone turnover. Markers of bone reabsorption, such as pyridinoline cross links, cross-linked N-telopeptide and C-telopeptide of type I collagen, can be detected in urine and may be of significant help for establishing a diagnosis of osteoporosis.
Associated stress fractures
The most frequently associated stress fracture is that of the ipsilateral, contralateral or both pubic rami. Aretxabala et al. [45] reported that 78% of patients with SIF had concomitant pubic rami and SIFs. De Smed and Neff [6] also reported a high association of concomitant pubic rami fractures. The authors concluded that SIFs may have preceded pubic fractures by 3–4 months and that the latter had a protracted course of healing compared with the former. Similarly, other authors have reported high frequencies of concomitant pubic fractures in variable proportions [26, 35, 77, 78].
Pelvis biomechanics dictate that disruption of the bony skeleton at one site may lead to increased stresses in other parts of the pelvic ring, resulting in fracture. Although it remains unclear which fracture (sacral or pubic rami) occurs first, De Smed and Neff [6] suggested that the initial disruption is likely to occur in the sacrum, and the subsequent instability this creates results in mechanical failure of the pubic rami. Therefore, detection of pubic rami fractures should raise clinical suspicion of coexistent SIFs in high-risk patients.
Radiographic investigation
Plain radiographs
Plain anterior posterior (AP) and lateral radiographs of the pelvis, sacrum and lower lumbar spine are generally requested as an initial screening tool. Inlet and outlet views of the pelvis are helpful to further demonstrate an underlying fracture and the overall integrity of the pelvic ring. Radiographs are, however, usually inadequate to demonstrate SIFs, especially in the acute setting and before the development of healing calcification that usually allows easier visualisation of fracture site. The curved anatomy of the sacrum, demineralisation of surrounding bone, distraction from concurrent SI joint arthritis and overlying bowel gas make SIF radiological diagnosis difficult [58]. Sclerotic bands and cortical disruptions along with fresh fracture lines may be seen in the sacral alae, indicating variable degrees of fracture healing [79]. Concomitant ipsilateral and contralateral pubic ramie fractures should raise the index of suspicion that posterior pelvic structures are also jeopardised [45]. Differential diagnostic dilemma arises when other pelvic insufficiency fractures coexist, mimicking malignant or metastatic disease due to their aggressive osteoblastic or osteolytic appearance depending on the stage of healing process [79].
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is by far the most sensitive screening investigation. It can pick up signal from bone marrow oedema that results from fracture inflammatory and reparation processes. T1-weighted images demonstrate a low signal intensity while T2-weighted images demonstrate high signal intensity. T2-weighted short tau inversion recovery (STIR) images and T2-weighted images with fat suppression are particularly sensitive to demonstrate a fracture line. Further enhancement can be achieved with intravenous gadolinium, but this is rarely necessary [80]. Coronal imaging of the sacrum is additionally helpful in revealing a horizontal component to the fracture. Blake and Connors [81] suggested that planning lateral MRIs of the sagittal sequences are sometimes useful in SIF diagnosis if the patient has had routine lumbar spine MRI for other suspected spinal pathology.
Bone scintigraphy
Bone scintigraphy with technetium-99 m medronate methylene diphosphonate (MDP) remains a sensitive technique for SIFs, particularly after a minimum time lapse of 48–72 h from symptom onset. A classic “H” pattern [30] may be apparent, and coupled with a corresponding clinical picture, this can be considered diagnostic [24, 79]. Formation of the “H” pattern, however, requires bilateral involvement and a horizontal fracture component to the sacral body that is not always present. In Finiels et al. [59] meta-analysis, complete bilateral involvement of the “H” sign was documented in only 43% of all cases where bone scintigraphy was performed. Clinicians should, however, be aware that bone scintigraphy can miss a bilateral sacral fracture since the SI joint often has a higher MDP uptake normally. Both MRI and bone scan, however, may provide inconclusive images often misinterpreted as metastatic bone disease, especially in the presence of a relevant past medical history.
Computed tomography
Computed tomography (CT) is a useful alternative to MRI and bone scintigraphy, as it provides reliable and valid results [80] highlighting sclerotic healing lines or fresh interdigitating fracture lines. These findings, however, can be subtle, and unless displaced or long-standing, fractures may be missed on the first reading. CT can be used as an adjunct to MRI and bone scintigraphy in excluding malignancy or osteomyelitis. Intact bony trabeculation and architecture could effectively provide the diagnosis of exclusion for malignant disease or osteomyelitis [79, 82].
Bone mineral density
Osteoporosis is the commonest denominator of SIFs and can better be assessed by measuring BMD. The gold standard for measuring BMD is the DEXA scan, which involves scanning of the lumbar spine, hip and sometimes the distal radius. T and Z scores are densitometric values that represent the number of standard deviations (SDs) above and below the mean for healthy controls at their peak BMD and age-matched controls, respectively. The World Health Organisation (WHO) has defined osteoporosis as a T score of <2.5 SD, and a Z score <1.5 SD should raise the suspicion of secondary osteoporosis [57].
Differential diagnosis
Malignancy and osteomyelitis are the most common pathologies involved in this region. Differential diagnosis is sometimes challenging since the osteoporotic appearance of the bone may mislead the clinician, appearing as distractive space occupying metastatic disease. Furthermore, the osteoblastic activity of fracture healing may also be misinterpreted as neoplastic or inflammatory processes. Significant past medical history for malignant disease along with bone, tumour and inflammatory markers may facilitate differential diagnosis [81]. In the case of diagnostic dilemma, CT can potentially demonstrate the intact or not architecture of bone trabeculation and set the differential diagnosis. Other conditions that produce pain in the SI joint or referred pain to that region include spinal stenosis, discogenic pain, osteoporotic vertebral fractures, facet-joint arthritis, trochanteric bursitis, sacroiliitis, gluteal and hamstring muscle strain, ischial tuberosity bursitis, intrapelvic, intraabdominal or retroperitoneal inflammation, infection or space-occupying processes and degenerative spondylolisthesis [57].
Treatment
The majority of SIFs are treated conservatively with bed rest and analgesia, followed by gradual mobilisation with walking aids as pain allows [57]. This results in the recovery of the vast majority of patients. Following initial management of SIFs, anabolic or antiresorptive medication is often prescribed to reduce the risk of further insufficiency fractures.
Medication
It should be assumed that patients with SIFs are osteopenic and would therefore benefit from supplements or treatment for secondary prevention of osteoporotic fragility fractures or both.
Calcium and vitamin D supplementation
Vitamin D deficiency is not uncommon in the elderly living alone and can be prevented by taking oral supplements. Ergocalciferol (calcium and vitamin D) is usually prescribed, and recommended daily doses include 1,200–1,500 mg Calcium with 20 µg vitamin D daily [64].
Antiresorptive agents
Bisphosphonates are potent inhibitors of bone reabsorption and widely prescribed in the management of osteoporosis. They are effective in increasing BMD of spine and hip, reducing the incidence of new fractures in patients with established osteoporosis [83, 84]; however, concerns have been raised about the potential oversuppression of bone turnover with long-term use [85]. Physiologically, osteoblastic bone formation follows bone resorption. Therefore, inhibition of bone resorption paradoxically may result in inhibition of bone formation. This has been demonstrated in animal studies where high doses of bisphosphonate resulted in noncompensated physiological microdamage. Microdamage “accumulation” is believed to be a direct result secondary to reduced osteoblastic activity [86]. In addition to microdamage accumulation, chronic suppression of bone turnover induced by bisphosponates may allow secondary hypermineralisation to continue, producing more brittle bone and thus predisposing to fractures [85]. The long-term effects of bisphosphonate therapy remain unknown. Randomised clinical trials support bisphosphonate therapy to be beneficial to bones during the first 5 years [87]. Based on the above-mentioned observations, clinicians may consider discontinuation of chronic bisphosphonate therapy in patients who develop insufficiency fractures. Calcitonin is licensed for the prevention and treatment of postmenopausal osteoporosis. In addition to increasing bone mass by reducing bone turnover, it is also an effective analgesic for bone pain. It can be given subcutaneously (100 U daily) or as a nasal spray (200 U daily).
Anabolic agents
Teriparatide (recombinant human PTH) and selective oestrogen receptor modulators (SERMS) [88] are approved for treatment of postmenopausal osteoporosis. Teriparatide is effective in increasing BMD [89], trabecular [90] and cortical thickness [91] and preventing osteocyte apoptosis [92].
Chemical pain control
A variety of analgesics, acting centrally (paracetamol, opioids) or peripherally [nonsteroidal anti-inflammatories (NSAIDs)] are widely available in clinical practise. The use of NSAIDs for pain in patients with fractures remains a source of controversy. There is reasonable experimental evidence indicating NSAIDs inhibit osteoblastic function [93] and fracture healing in animals [94]. No level 1 studies have been performed investigating potential negative effects of NSAIDs on fracture healing in humans although retrospective studies have reported an increased rate of nonunion [95].
Rehabilitation
Nonchemical pain control
Other therapeutic modalities that can provide symptomatic benefit during early rehabilitation include transcutaneous electrical stimulation (TENS), ultrasound and gentle physiotherapy.
Physiotherapy
A period of bed rest was traditionally recommended for the treatment of SIFs. More recently, early rehabilitation and moderate weight-bearing exercises, within the confines of pain tolerance, has been suggested. Evidence supporting earlier rehabilitation is provided from studies demonstrating a stimulant effect of weight bearing and muscle tension on osteoblast-mediated bone formation [96]. Periods of immobility have additionally been shown to result in unrestrained osteoclast-mediated bone reabsorption [96]. Other recognised complications of prolonged periods of immobilisation include deep vein thrombosis [97], pulmonary embolus [98], loss of muscle strength, impaired cardiac function [99], respiratory complications, urinary tract complications, gastrointestinal tract complications and mental health symptoms [100]. Assisted mobilisation can be achieved with external devices, such as walking frames or hydrotherapy, which is often better tolerated by many patients at the earlier stages of fracture healing.
Interventional methods under study
The principle of vertebroplasty has more recently been attempted for the management of SIF—so called sacroplasty [48]. Polymethylmethacrylate (PMMA) cement is injected into the fracture site under fluoroscopy or CT guidance with the aim of stabilising the fracture [48, 49, 53, 54]. Published cases to date report immediate pain relief and improved quality of life following this procedure [48, 49, 53, 54]. However, sacroplasty remains a technique under study, having so far only been applied in limited specialised centres in few patients without controls. Presently, therefore, strong evidence supporting its widespread use over conservative management is lacking.
Key issues
Subtle clinical presentations and radiographic findings mimicking unrelated or overlapping conditions often result in SIF diagnosis being elusive:
-
In the clinical setting, SIFs should be suspected in patients presenting with low back and pelvic pain and with no history of trauma. Postmenopausal osteopenia is the most significant risk factor.
-
Pregnant women are also at risk.
-
Plain radiographs are often negative, especially in the acute setting. Pubic rami fractures should highlight the possibility of coexistent SIFs. Investigation with MRI, CT scanning or bone scintigraphy may be useful.
-
Reversible causes of secondary osteoporosis should be considered, particularly in men and younger patients.
-
Bisphosphonates are widely prescribed and have an important role in both primary and secondary prevention of osteoporotic fracture, but clinicians should be aware of a potential excessive suppression of bone turnover following long-term therapy and consider their withdrawal if insufficiency fractures develop.
References
Kannus P, Palvanen M, Niemi S et al (2000) Epidemiology of osteoporotic pelvic fractures in elderly people in Finland: sharp increase in 1970–1997 and alarming projections for the new millennium. Osteoporos Int 11:443–448
Kannus P, Palvanen M, Parkkari J et al (2005) Osteoporotic pelvic fractures in elderly women. Osteoporos Int 16:1304–1305
Lourie H (1982) Spontaneous osteoporotic fracture of the sacrum. An unrecognized syndrome of the elderly. JAMA 248:715–717
Ries T (1983) Detection of osteoporotic sacral fractures with radionuclides. Radiology 146:783–785
Gacetta DJ, Yandow DR (1984) Computed tomography of spontaneous osteoporotic sacral fractures. J Comput Assist Tomogr 8:1190–1191
De Smet AA, Neff JR (1985) Pubic and sacral insufficiency fractures: clinical course and radiologic findings. AJR Am J Roentgenol 145:601–606
Schneider R, Yacovone J, Ghelman B (1985) Unsuspected sacral fractures: detection by radionuclide bone scanning. AJR Am J Roentgenol 144:337–341
Guilbeau JC, Arrive L, Maurice F et al (1986) Spontaneous fracture of the sacrum due to “insufficiency”. An overlooked cause of low lumbago in elderly women. J Radiol 67:741–744
Balseiro J, Brower AC, Ziessman HA (1987) Scintigraphic diagnosis of sacral fractures. AJR Am J Roentgenol 148:111–113
Carter SR (1987) Stress fracture of the sacrum: brief report. J Bone Joint Surg Br 69:843–844
Gaucher A, Regent D, Paul JP et al (1987) Fractures caused by bony insufficiency of the sacrum. Clinical, radiographic, scintigraphic and x-ray computed tomographic symptomatology. J Radiol 68:433–440
Pere P, Gaucher A, Pourel J (1987) Fractures caused by osseous insufficiency of the sacrum. Incidence, complications and pathogenesis. Rev Rhum Mal Osteoartic 54:311–313
Davies AM, Evans NS, Struthers GR (1988) Parasymphyseal and associated insufficiency fractures of the pelvis and sacrum. Br J Radiol 61:103–108
Hauge MD, Cooper KL, Litin SC (1988) Insufficiency fractures of the pelvis that simulate metastatic disease. Mayo Clin Proc 63:807–812
Rawlings CE 3rd, Wilkins RH, Martinez S et al (1988) Osteoporotic sacral fractures: a clinical study. Neurosurgery 22:72–76
Brahme SK, Cervilla V, Vint V et al (1990) Magnetic resonance appearance of sacral insufficiency fractures. Skeletal Radiol 19:489–493
Guttner B, Freyschmidt J, Hohlweg-Majert P (1990) Stress fracture of the sacral bone. Rofo 152:236–237
Jones JW (1991) Insufficiency fracture of the sacrum with displacement and neurologic damage: a case report and review of the literature. J Am Geriatr Soc 39:280–283
Kayes K, Coscia M, Braunstein E (1991) Radiologic case study. Sacral insufficiency fracture. Orthopedics 14:817–818
Khorasani R, Nagel JS, Tumeh SS (1991) Radiologic vignette. Sacral insufficiency fracture. Arthritis Rheum 34:1387–1390
Nokes SR, Boyd CM, Kovaleski TM (1991) Radiological case of the month. Insufficiency fractures of the sacrum and left pubis. J Ark Med Soc 87:345–346
Stroebel RJ, Ginsburg WW, McLeod RA (1991) Sacral insufficiency fractures: an often-unsuspected cause of low back pain. J Rheumatol 18:117–119
Abe H, Nakamura M, Takahashi S et al (1992) Radiation-induced insufficiency fractures of the pelvis: evaluation with 99mTc-methylene diphosphonate scintigraphy. AJR Am J Roentgenol 158:599–602
Newhouse KE, el-Khoury GY, Buckwalter JA (1992) Occult sacral fractures in osteopenic patients. J Bone Joint Surg Am 74:1472–1477
Lien HH, Blomlie V, Talle K et al (1992) Radiation-induced fracture of the sacrum: findings on MR. AJR Am J Roentgenol 159:227
Weber M, Hasler P, Gerber H (1993) Insufficiency fractures of the sacrum. Twenty cases and review of the literature. Spine 18:2507–2512
Peris P, Guanabens N, Pons F et al (1993) Clinical evolution of sacral stress fractures: influence of additional pelvic fractures. Ann Rheum Dis 52:545–547
Blomlie V, Lien HH, Iversen T et al (1993) Radiation-induced insufficiency fractures of the sacrum: evaluation with MR imaging. Radiology 188:241–244
Peh WC, Gough AK, Sheeran T et al (1993) Pelvic insufficiency fractures in rheumatoid arthritis. Br J Rheumatol 32:319–324
Leroux JL, Denat B, Thomas E et al (1993) Sacral insufficiency fractures presenting as acute low-back pain. Biomechanical aspects. Spine 18:2502–2506
West SG, Troutner JL, Baker MR et al (1994) Sacral insufficiency fractures in rheumatoid arthritis. Spine 15:2117–2121
Gotis-Graham I, McGuigan L, Diamond T et al (1994) Sacral insufficiency fractures in the elderly. J Bone Joint Surg Br 76:882–886
Stabler A, Beck R, Bartl R et al (1995) Vacuum phenomena in insufficiency fractures of the sacrum. Skeletal Radiol 24:31–35
Peh WC, Khong PL, Ho WY (1996) Insufficiency fractures of the sacrum and os pubis. Br J Hosp Med 54:15–19
Grasland A, Pouchot J, Mathieu A et al (1996) Sacral insufficiency fractures: an easily overlooked cause of back pain in elderly women. Arch Intern Med 156:668–674
Peh WC, Khong PL, Ho WY (1997) Case report: sacral insufficiency fractures masking malignancy. Clin Radiol 52:71–72
Breuil V, Brocq O, Euller-Ziegler L et al (1997) Insufficiency fracture of the sacrum revealing a pregnancy associated osteoporosis. First case report. Ann Rheum Dis 56:278–279
Grimaud A, Oddo F, Thibaud I et al (1997) Fracture of the sacrum caused by bone insufficiency in a pregnant woman. J Radiol 78:511–512
Schulman LL, Addesso V, Staron RB et al (1997) Insufficiency fractures of the sacrum: a cause of low back pain after lung transplantation. J Heart Lung Transplant 16:1081–1085
Parikh VA, Edlund JW (1998) Sacral insufficiency fractures-rare complication of pelvic radiation for rectal carcinoma: report of a case. Dis Colon Rectum 41:254–257
Verhaegen MJ, Sauter AJ (1999) Insufficiency fractures, an often unrecognized diagnosis. Arch Orthop Trauma Surg 119:115–116
Weber M, Hasler P, Gerber H (1999) Sacral insufficiency fractures as an unsuspected cause of low back pain. Rheumatology 38:90–91
Schmid L, Pfirrmann C, Hess T et al (1999) Bilateral fracture of the sacrum associated with pregnancy: a case report. Osteoporos Int 10:91–93
Peh WC (2000) Intrafracture fluid: a new diagnostic sign of insufficiency fractures of the sacrum and ilium. Br J Radiol 73:895–898
Aretxabala I, Fraiz E, Perez-Ruiz F et al (2000) Sacral insufficiency fractures. High association with pubic rami fractures. Clin Rheumatol 19:399–401
Peh WC (2001) Clinics in diagnostic imaging (60). Insufficiency fractures of the pelvis. Singapore Med J 42:183–186
Wild A, Jaeger M, Haak H et al (2002) Sacral insufficiency fracture, an unsuspected cause of low-back pain in elderly women. Arch Orthop Trauma Surg 122:58–60
Garant M (2002) Sacroplasty: a new treatment for sacral insufficiency fracture. J Vasc Interv Radiol 13:1265–1267
Pommersheim W, Huang-Hellinger F, Baker M et al (2003) Sacroplasty: a treatment for sacral insufficiency fractures. AJNR Am J Neuroradiol 24:1003–1007
Hoshino Y, Doita M, Yoshikawa M et al (2004) Unstable pelvic insufficiency fracture in a patient with rheumatoid arthritis. Rheumatol Int 24:46–49
Khanna AJ, Kebaish KM, Ozdemir HM et al (2004) Sacral insufficiency fracture surgically treated by fibular allograft. J Spinal Disord Tech 17:167–173
Fujii M, Abe K, Hayashi K et al (2005) Honda sign and variants in patients suspected of having a sacral insufficiency fracture. Clin Nucl Med 30:165–169
Butler CL, Given CA 2nd, Michel SJ et al (2005) Percutaneous sacroplasty for the treatment of sacral insufficiency fractures. AJR Am J Roentgenol 184:1956–1959
Brook AL, Mirsky DM, Bello JA (2005) Computerized tomography guided sacroplasty: a practical treatment for sacral insufficiency fracture: case report. Spine 30:E450–E454
Dasgupta B, Shah N, Brown H et al (1998) Sacral insufficiency fractures: an unsuspected cause of low back pain. Br J Rheumatol 37:789–793
Denis F, Davis S, Comfort T (1988) Sacral fractures: an important problem. Retrospective analysis of 236 cases. Clin Orthop Relat Res 227:67–81
Lin J, Lane JM (2003) Sacral stress fractures. J Womens Health 12:879–888
White JH, Hague C, Nicolau S et al (2003) Imaging sacral fractures. Clin Radiol 58:914–921
Finiels H, Finiels PJ, Jacquot JM et al (1997) Fractures of the sacrum caused by bone insufficiency. Meta-analysis of 508 cases. Presse Med 26:1568–1573
Negishi H, Kobayashi M, Nishida R et al (2002) Primary hyperparathyroidism and simultaneous bilateral fracture of the femoral neck during pregnancy. J Trauma 52:367–369
Henry AP, Lachmann E, Tunkel RS et al (1996) Pelvic insufficiency fractures after irradiation: diagnosis, management, and rehabilitation. Arch Phys Med Rehabil 77:414–416
Eastell R, Dickson ER, Hodgson SF et al (1991) Rates of vertebral bone loss before and after liver transplantation in women with primary biliary cirrhosis. Hepatology 14:296–300
Peris P, Navasa M, Guanabens N et al (1993) Sacral stress fracture after liver transplantation. Br J Rheumal 32:702–704
Lips P (2001) Vitamin D deficiency and secondary hyperthyroidism in the elderly: concequences for bone loss and fractures and therapeutic implications. Endocr Rev 22:477–501
Lips P, Obrant KJ (1991) The pathogenesis and treatment of hip fractures. Osteoporosis Int 1:218–231
Thienpont E, Simon JP, Fabry G (1999) Sacral stress fracture during pregnancy-a case report. Acta Orthop Scand 70:525–526
Schmid L, Pfirrmann C, Hess T et al (1999) Bilateral fracture of the sacrum associated with pregnancy: a case report. Osteoporos Int 10:91–93
Rousiere M, Kahan A, Job-Deslandre C (2001) Postpartal sacral fracture without osteoporosis. Joint Bone Spine 68:71–73
Kohlmeier L, Marcus R (1995) Calcium disorders of pregnancy. Review. Endocrinol Metab Clin North Am 24:15–39
Black AJ, Topping J, Durham B (2000) A detailed assessment of alterations in bone turnover, calcium homeostasis, and bone density in normal pregnancy. J Bone Miner Res 15:557–563
Kent GN, Price RI, Gutteridge DH et al (1990) Human lactation: forearm trabecular bone loss, increased bone turnover, and renal conservation of calcium and inorganic phosphate with recovery of bone mass following weaning. J Bone Miner Res 5:361–369
McFarland EG, Giangarra C (1996) Sacral stress fractures in athletes. Clin Orthop Relat Res 329:240–243
Thienpont E, Simon JP, Fabry G (1999) Sacral stress fracture during pregnancy-a case report. Acta Orthop Scand 70:525–526
Di Gregorio S, Danilowicz K, Rubin Z et al (2000) Osteoporosis with vertebral fractures associated with pregnancy and lactation. Nutrition 16:1052–1055
Magee DJ (eds) (1997) Orthopedic physical assessment, 3rd ed. W.B. Saunders, Philadelphia
Jacquot JM, Finiels H, Fardjad S et al (1999) Neurological complications in insufficiency fractures of the sacrum. Three case-reports. Rev Rhum Engl Ed 66:109–114
Mathers DM, Major GA, Allen L et al (1993) Insufficiency fractures of the sacrum. Ann Rheum Dis 52:621–623
Peh WC, Ooi GC (1997) Vacuum phenomena in the sacroiliac joints and in association with sacral insufficiency fractures: incidence and significance. Spine 22:2005–2008
Peh WC, Khong PL, Yin Y et al (1996) Imaging of pelvic insufficiency fractures. Radiographics 16:335–348
Grangier C, Garcia J, Howarth NR et al (1997) Role of MRI in the diagnosis of insufficiency fractures of the sacrum and acetabular roof. Skeletal Radiol 26:517–524
Blake SP, Connors AM (2004) Sacral insufficiency fracture. Br J Radiol 77:891–896
Lin J, Lachmann E, Nagler W (2001) Sacral insufficiency fractures: a report of two cases and a review of the literature. J Womens Health Gend Based Med 10:699–705
Black DM, Cummings SR, Karpf DB et al (1996) Randomised trial of effect of alendronate on risk of fracture in women with existing vertebral fractures. Fracture Intervention trial Research Group. Lancet 248:1535–1541
McClung MR, Geusens P, Miller PD et al (2001) Effect of risedronate on the risk of hip fracture in elderly women. Hip Intervention Program Study Group. N Engl J Med 344:333–340
Odvina CV, Zerwekh JE, Rao DS et al (2005) Severely suppressed bone turnover: a potential complication of alendronate therapy. J Clin Endocrinol Metab 90:1294–1301
Mashiba T, Turner CH, Hirano T et al (2001) Effects of suppressed bone turnover by bisphosphonates on microdamage accumulation and biomechanical properties in clinically relevant skeletal sites in beagles. Bone 28:524–531
Ott SM (2005) Editorial: Long term safety of bisphosphonates. J Clin Endocrinol Metab 90:1897–1899
Vogelvang TE, van der Mooren MJ, Mijatovic V (2004) Hormone replacement therapy, selective estrogen receptor modulators, and tissue-specific compounds: cardiovascular effects and clinical implications. Treat Endocrinol 3:105–115
Body JJ, Gaich GA, Scheele WH et al (2002) A randomized double-blind trial to compare the efficacy of teriparatide [recombinant human parathyroid hormone (1–34)] with alendronate in postmenopausal women with osteoporosis. J Clin Endocrinol Metab 87:4528–4535
Neer RM, Arnaud CD, Zanchetta JR et al (2001) Effect of parathyroid hormone (1–34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 344:1434–1441
Dempster DW, Cosman F, Kurland ES et al (2001) Effects of daily treatment with parathyroid hormone on bone microarchitecture and turnover in patients with osteoporosis: a paired biopsy study. J Bone Miner Res 16:1846–1853
Jilka RL, Weinstein RS, Bellido T et al (1999) Increased bone formation by prevention of osteoblast apoptosis with parathyroid hormone. J Clin Invest 104:439–446
Simon AM, Manigrasso MB, O’Connor JP (2002) Cyclo-oxygenase 2 function is essential for bone fracture healing. J Bone Miner Re 17:963–976
Altman RD, Latta LL, Keer R et al Effect of non-steroidal anti-inflammatory drugs on fracture healing: a laboratory study in rats. J Orthop Trauma 9:392–400
Giannoudis PV, MacDonald DA, Matthews SJ et al (2000) Non-union of the femoral diaphysis. The influence of reaming and non-steroidal anti-inflammatory drugs. J Bone Joint Surg Br 82:655–658
Chao EY, Inoue N, Koo TK et al (2004) Biomechanical considerations of fracture treatment and bone quality maintenance in elderly patients and patients with osteoporosis. Clin Orthop Relat Res 425:12–25
Fishmann AJ, Greeno RA, Brooks LR et al (1994) Prevention of deep veil thrombosis and pulmonary embolism in acetabular and pelvic fracture. Clin Orthop Rel Res 305:133–137
Buerger PM, Peoples JB, Lemman GW et al (1993) Risk of pulmonary emboli in patients with pelvic fractures. Am Surg 59:505–508
Chobanian AV, Lillie RD, Tercyak A et al (1974) The metabolic effects and hemodynamic effects of prolonged bed rest in normal subjects. Circulation 49:551–559
Babayev M, Lachmann E, Nagler W (2000) The controversy surrounding sacral insufficiency fractures: to ambulate or notto ambulate? Review. Am J Phys Med Rehabil 79:404–409
Author information
Authors and Affiliations
Corresponding author
Additional information
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article. No funds were received in support of this study.
Rights and permissions
About this article
Cite this article
Tsiridis, E., Upadhyay, N. & Giannoudis, P.V. Sacral insufficiency fractures: current concepts of management. Osteoporos Int 17, 1716–1725 (2006). https://doi.org/10.1007/s00198-006-0175-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-006-0175-1