Article Text

Abstract
Background Stent-assisted coiling is a commonly adopted technique employed in the coiling of broader-based aneurysms. It avoids flow arrest and the risk of vessel rupture associated with balloon-assisted coiling. However, there is a risk of stent thrombosis with the corollary risk of stroke during and after the procedure. Antiplatelet agents are used to mitigate this risk but raise a secondary concern of hemorrhagic complications, particularly with ruptured aneurysm where further interventions such as ventriculostomy occur not infrequently. Stent removal after coil embolization would eliminate the risk of post-procedure stent thromboembolic complications and alleviate the need for continuing antiplatelet therapy.
Methods A prospectively maintained endovascular database was searched to identify patients who underwent stent-assisted coil embolization followed by stent retrieval and removal. The clinical and technical aspects of the cases were obtained in addition to the procedural outcomes.
Results Three cases were identified where the use of the fully resheathable Solitaire AB Neurovascular Remodeling Device permitted the coiling of broad-based aneurysms with subsequent retrieval and removal of the stent. All patients presented with subarachnoid hemorrhage and received aspirin prior to the procedure. Two patients did not require antiplatelet therapy after the procedure. No coil herniation or thromboembolic events were encountered.
Conclusions Stent retrieval and removal can be done safely in selected cases at the end of stent-assisted coil embolization using the Solitaire AB device. This technique avoids the need for continuing antiplatelet therapy, which can be particularly important in the setting of acute subarachnoid hemorrhage.
- Aneurysm
- Brain
- Coil
- Stent
- Subarachnoid
Statistics from Altmetric.com
Background
Stent-assisted coiling has become a routine component of the interventionist’s armamentarium. It facilitates achieving excellent angiographic results in morphologically challenging aneurysms. Stent use mandates starting dual antiplatelet therapy in the peri-procedure period, which causes some practitioners to shy away from their use in the setting of acute subarachnoid hemorrhage (SAH). A recent meta-analysis showed that stent-assisted coiling in the setting of SAH is associated with a high risk of clinically significant intracranial hemorrhage (8%) and clinically significant thromboembolic events (6%).1 Additionally, the risk of hemorrhagic complications during external ventricular drain placement is significantly higher in patients on dual antiplatelet therapy after stent-assisted coiling compared with the coiling procedure without a stent.2 ,3 In cardiac disease studies, long-term aspirin use in any dose is associated with a 1.5–2.5% risk of significant hemorrhage.4 To date, this risk is not apparent in the literature on stent-assisted coiling due to the relatively short-term clinical follow-up.
The use of retrievable stents offers the advantage of aneurysm embolization while maintaining patency of parent and branching vessels. The Solitaire AB Neurovascular Remodeling Device (Covidien, Irvine, California, USA) gives the advantage of fully retrieving and redeploying the stent as needed during the procedure until optimal positioning is achieved. This feature can be used to retrieve the stent at the end of the procedure, which eliminates any risk of future stent thrombosis and the need for continuing antiplatelet therapy. In this report we describe three cases where stent-assisted coiling using the Solitaire AB device was successfully performed followed by safe retrieval of the stent.
Methods
Patients who underwent stent-assisted coil embolization with subsequent stent retrieval and removal were identified from the Alberta Comprehensive Outcome Research in Neurosciences (ACORN) database. This was a retrospective analysis of a prospectively-maintained database of all neurointerventional surgery patients treated at the University of Calgary. Clinical, technical and outcome data were retrieved.
Results
Three patients were identified. All presented with ruptured wide-neck aneurysms and underwent urgent stent-assisted coil embolization using the Solitaire AB Neurovascular Remodeling Device. In all cases the coiling microcatheter (Excelsior SL-10 microcatheter; Boston Scientific, Natick, Massachusetts, USA) was positioned inside the aneurysm fundus first. Subsequently, a transport microcatheter (Prowler Select Plus; Cordis Endovascular, Miami Lakes, Florida, USA) was advanced over a microwire (Headliner 0.016 inch; Terumo Medical Corporation, Ann Arbor, Michigan, USA) bridging the neck of the aneurysm. The microwire was then removed and the Solitaire AB Neurovascular Remodeling Device was advanced inside the transport microcatheter and deployed across the aneurysm neck, jailing the coiling microcatheter inside the aneurysm. The transport microcatheter was left in a proximal position until coil embolization was completed. Finally, the coiling microcatheter was withdrawn and the transport microcatheter was advanced to resheath and retrieve the Solitaire AB completely followed by careful removal of the transport microcatheter.
Case synopses
Case 1
A middle-aged woman presented 3 days after the onset of a thunderclap headache. She was found to have a modified Fischer grade 1 SAH secondary to a ruptured right-sided middle cerebral artery (MCA) bifurcation aneurysm. The aneurysm measured 7×6 mm and the neck of the aneurysm measured 4 mm. Although the aneurysm neck was relatively narrow, the base of the aneurysm incorporated one of the M2 MCA branches making primary coiling challenging. The patient was therefore pretreated with 650 mg aspirin rectally in anticipation of stent use. After access to the aneurysm was obtained, a 4×20 Solitaire AB was placed with its proximal portion in the distal M1 and its distal portion in the superior M2 (Ofigure 1). As the stent was being deployed, gentle forward pressure was applied to the stent wire halfway during deployment to produce some bulging of the stent into the aneurysm neck. Subsequently, six microcoils were used to pack the aneurysm and the stent was then carefully resheathed and removed. A repeat angiogram showed satisfactory exclusion of the aneurysm with no residual or coil herniation. No thromboembolic complications were noted.
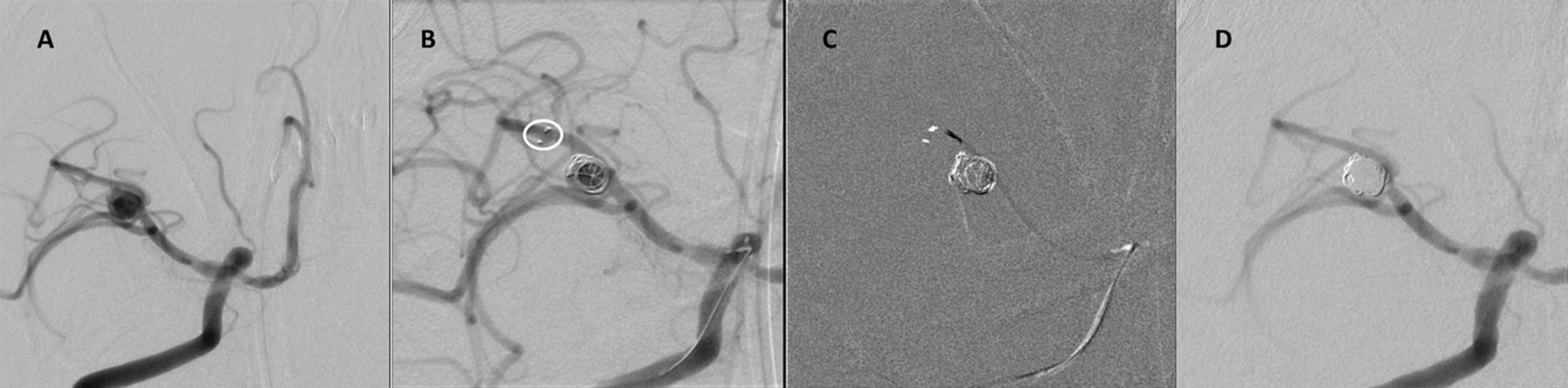
Digital subtraction angiogram (DSA) showing (A) the middle cerebral artery (MCA) aneurysm; (B) Solitaire AB deployed into superior M2-MCA and initial coiling (the circle shows the stent markers); (C) stent resheathing into the microcatheter; and (D) final DSA.
Case 2
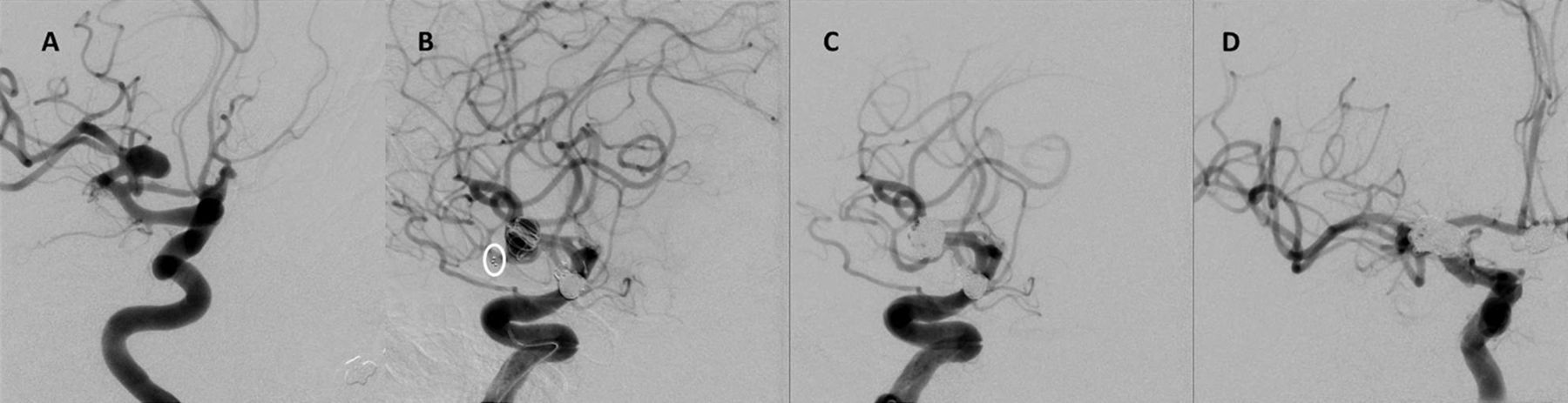
A middle-aged woman with a modified Fischer grade 4 SAH was found to have a ruptured wide-neck 6 mm basilar tip aneurysm with a 4.5 mm wide neck. As the aneurysm incorporated both posterior cerebral arteries (PCAs) and superior cerebellar arteries (SCAs), the patient was loaded with 650 mg aspirin rectally in preparation for stent use.
The initial plan was to deploy a stent in the right PCA and to try to coil the aneurysm. If insufficient, a balloon was to be passed into the left PCA to allow coiling. After a 4×20 Solitaire AB was deployed and detached in the right PCA, we could not advance a balloon through the stent into the left PCA so a 3×20 mm Solitaire AB was deployed into the left PCA but not detached (Ofigure 2). The aneurysm was then coil occluded using nine microcoils. The Solitaire AB in the left PCA stent was then carefully retrieved and withdrawn. Low-dose heparin boluses were given intermittently during the procedure and, once the aneurysm was appropriately secured, an intravenous abciximab load was administered. Final angiography showed complete occlusion of the aneurysm with no evidence of coil herniation or distal thromboembolic complications. The patient was started on aspirin and clopidogrel after the procedure.

Digital subtraction angiogram (DSA) showing (A) the basilar tip aneurysm; (B) two Solitaire AB devices deployed into the right and left posterior cerebral arteries (PCAs) and initial coiling (the circle shows the left PCA stent markers); (C) stent resheathing into the microcatheter; and (D) final DSA.
Case 3
A middle-aged woman presented 5 days after the onset of a thunderclap headache. Imaging identified a modified Fischer grade 1 SAH and the presence of two aneurysms: a 6 mm anterior communicating artery (ACom) aneurysm and an 8 mm right MCA aneurysm with a 5-mm neck. The decision was made to treat both aneurysms in the same setting. The patient was loaded with 325 mg aspirin orally prior to the procedure. Primary coiling of the ACom aneurysm was performed. Subsequently, a 3×30 mm Solitaire AB was deployed across the MCA aneurysm neck (Ofigure 3). Coiling was successfully performed using eight microcoils. The stent was then resheathed and pulled out. No antiplatelet agents were required after the procedure.
{kind=link}
{kind=link}
{kind=link}
(A) Middle cerebral artery (MCA) aneurysm prior to coiling; (B) first few coils deployed into the aneurysm with the Solitaire AB stents deployed into the inferior MCA branch (the circle shows the stent markers); (C, D) final DSA after the stent was withdrawn.
Discussion
Stent-assisted coiling facilitates the endovascular treatment of broad-based ruptured and unruptured aneurysms. However, stent use is associated with risks of hemorrhagic and thrombotic complications that are not trivial, especially in ruptured aneurysms. Retrieving the stent after coil embolization alleviates the need for continuing antiplatelet therapy and reduces hemorrhagic risks associated with antiplatelet use. While retrievable stents have been successfully used in endovascular stroke treatment, the Solitaire AB device has particular advantages with respect to the described technique. It is simple to deploy and retrieve and its closed cell design should minimize trapping coil loops. In addition, the presence of an electrolytic detachment system gives operators the option of permanent detachment of the stent if safe stent retrieval is not possible. While the safety of this technique is yet to be proven, it avoids some of the risks associated with balloon-assisted coiling, particularly transient flow arrest, balloon-related intraprocedural thromboembolic events and trapping of the microcatheter. Such risks were behind some modifications of the classical technique of balloon-assisted coiling.5 There is, in addition, a very small risk of vessel rupture associated with balloon inflation.
A number of reports have described the feasibility of stent-assisted coiling using the Solitaire AB Neurovascular Remodeling Device.6 ,7 However, long-term safety results on stent-assisted coiling technique in general are sparse. A nine-center registry published 2-year follow-up data on 229 patients treated with Enterprise (Cordis Neurovascular) stent-assisted coiling, 32 of whom had ruptured aneurysms at the time of treatment.8 Angiographic in-stent stenosis was found in 3.4%, thromboembolic events occurred in 4.4% and 1.0% suffered intracerebral hemorrhage.
The technique of temporary neck remodeling has been described using the Enterprise stent.9 ,10 However, the use of the Solitaire stent has a number of advantages. First, the Solitaire stent is fully resheathable, even after complete deployment, which allows proper positioning of the stent. In addition, if forward pressure is applied during deployment of the stent, part of the stent might bulge into the aneurysm neck for added parent vessel protection. In cases where the stent cannot be resheathed, the Solitaire can be detached.
Our report has limitations. In the reported cases stent retrieval was deemed to be safe after a clear margin was seen between the coil mass and expected location of the stent. Stent retrieval is not advisable in situations where such a safety margin is not present or is hard to appreciate. While the stent can be hard to visualize, the safety margin would be the area at the aneurysm neck between where the stent is expected to reside and the coil mass. The retrieval process was done very carefully by an experienced operator (MG). Stent retrieval may result in coil herniation and arterial occlusion if some coil loops are tangled inside the stent. However, the overlapping design of the stent onto itself when the stent size is larger than the target vessel further decreases the likelihood of coils entangling inside the stent. Stent retrieval may not affect the decision to continue antiplatelet therapy if another stent is to be permanently detached, as in Y-configuration stent use. However, reducing the number of stents used may theoretically reduce the thromboembolic risk. Finally, stent retrieval would not affect the intraprocedural use of antiplatelets nor the immediate thromboembolic risk while the stent is deployed. As this technique is not associated with any procedural cost saving, its overall impact on the cost would be minimal.
Conclusion
We demonstrate the feasibility of stent retrieval and removal after stent-assisted coil embolization in carefully selected patients with ruptured intracranial aneurysms. The use of this technique is implied to decrease the risk of any future stent-related thromboembolic complications and the hemorrhagic risk from dual antiplatelet therapy.
Footnotes
-
Contributors All authors contributed to the conceptual design, data acquisition, literature review, drafting or critical revision of the manuscript.
-
Competing interests None.
-
Ethics approval Ethical approval was obtained from the Conjoint Health Research Ethics Board at the University of Calgary.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement These cases are part of a prospectively maintained database.