Article Text

Abstract
Background and purpose Basilar artery occlusion remains one of the most devastating subtypes of stroke. Intravenous and intra-arterial therapy have altered the natural history of this disease; however, clinical results remain poor. Therefore, exploring more aggressive and innovative management is warranted.
Methods Six consecutive patients presenting with a basilar artery occlusion were treated with the same general algorithm of intra-arterial tissue plasminogen activator and mechanical thrombectomy with the Merci retrieval system. If complete recanalization was not achieved after two passes, manual syringe aspiration through a 4.3F catheter was employed.
Results All interventions utilizing aspiration thrombectomy resulted in recanalization, with five out of six cases displaying TIMI3/TICI3 flow and one patient resulting in complete recanalization of the basilar artery with persistent thrombus in one P2 segment (TIMI2/TICI2B). All patients survived, with five out of six independent in activities of daily living at 3 months (mRS 0–2).
Conclusions Our small case series indicates that aspiration thrombectomy performed manually through a 4.3F catheter can facilitate recanalization of basilar artery occlusion with acceptable clinical outcomes.
- Intra-arterial
- basilar occlusion
- aspiration
- thrombectomy
- atherosclerosis
- stroke
- angiography
- thrombectomy
- thrombolysis
Statistics from Altmetric.com
- Intra-arterial
- basilar occlusion
- aspiration
- thrombectomy
- atherosclerosis
- stroke
- angiography
- thrombectomy
- thrombolysis
Introduction
The clinical syndrome of basilar artery occlusion (BAO) was first described in detail by Kubik and Adams in 1946.1 Based on clinical and pathological studies, BAO was recognized early on as having particularly dismal outcomes. Today, with 20% of all ischemic strokes occurring in the posterior circulation, BAO remains the stroke subtype with the highest mortality.2 Neurological injury is caused by direct damage to the brain stem, cranial nerves and autonomic centers, with death and dependency rates of >70% even after treatment.3 Vertigo, headache, dysarthria, ataxia, cranial nerve palsies (IV, VI, VII, IX–X11), altered level of consciousness, hemi- or tetraparesis and gaze paresis constitute the most common signs and symptoms on admission.4
Regardless of treatment, recanalization is the single greatest predictor of good outcome.3 5 The likelihood of a good outcome in non-recanalized patients is in single digits.3 Given the poor natural history without recanalization, many centers resort to primary intra-arterial therapy or intravenous tissue plasminogen activator (TPA) with intra-arterial bridging therapy in patients who do not recanalize and have sufficient penumbral brain to allow a good recovery. In selected cases, this has been shown to be possible as far out in time as 50 h.6 Considering the higher rates of recanalization with intra-arterial therapy and the short time window required for administration of intravenous thrombolytics, intra-arterial therapy with or without intravenous therapy is considered the standard form of therapy used in many centers.3 7–9
The current armamentarium for intra-arterial therapy includes thrombolytics and a variety of devices intended to disrupt, stent or aspirate thrombus. The latter has been described with the Penumbra System (Penumbra Inc., Alameda, California, USA), which uses continuous aspiration through a pump connected to a catheter.10 A recently introduced 4.3F catheter provides another method to remove clot via intermittent, manual aspiration. We describe six consecutive cases of BAO treated with aspiration thrombectomy and short-term follow-up.
Materials and methods
Study population
This retrospective study was approved by an institutional review committee. The subjects or their families were enrolled in our prospectively collected research registry. Six consecutive patients admitted to the University of Pittsburgh Medical Center (UPMC) were evaluated for treatment by the stroke service and determined to have a BAO by non-invasive imaging. Our imaging protocol typically included non-contrast CT followed by CT angiography (CTA) and CT perfusion (CTP). Based on our previous experience, we typically consider intra-arterial therapy for any patient presenting within 6 h, regardless of their neurological examination, and any patient over 6 h who, in the opinion of the treating stroke neurologist, lacks a significant stroke burden on MRI to preclude a good outcome. If presenting within 3 h, intravenous TPA (Activase; Genentech, San Francisco, California, USA) was administered.
Treatment algorithm
Digital subtraction angiography (DSA) was performed. If an occlusive or flow-limiting subocclusive lesion remained, intra-arterial therapy was initiated. For patients who did not receive intravenous TPA, heparin was given as a bolus only unless otherwise contraindicated. We followed a protocol of placing either a 6F Envoy (Cordis, Miami Lakes, Florida, USA) or 8F Merci balloon guide catheter (Concentric Medical, Mountain View, California, USA) into the dominant vertebral artery (VA). An MC18L Merci microcatheter (Concentric Medical) was advanced over a 0.014 inch X-Celerator guidewire (ev3, Irvine, California, USA) through the clot. TPA was administered into the thrombus while gently advancing and retracting the microcatheter. The total volume of intra-arterial TPA given depended on the amount of previously administered systemic anticoagulation or thrombolytic, clot morphology and stroke burden on preprocedural imaging study. If the clot failed to dislodge, then the MC18L microcatheter was advanced distal to the clot and the Merci Retriever (Concentric Medical) was deployed for a maximum of two passes.
Failure to recanalize after two passes led to the use of the Outreach Distal Access Catheter (DAC) (Concentric Medical).11 The DAC is a single-lumen, small diameter catheter designed to provide distal access and support for interventions in tortuous anatomy. The inner and outer diameter (OD) measure 3.3F (0.044 inch) and 4.3F (0.056 inch), respectively. It was initially intended to enhance the effectiveness of the Merci Retrieval System to aid in clot removal. This catheter was advanced in a tri-axial system up to or into the proximal clot over an MC18L microcatheter with a 0.014 inch guidewire. After removal of the microcatheter and guidewire, vigorous aspiration with a 20 cc syringe was employed. The catheter was gently advanced and retracted, followed by careful but quick removal while maintaining continuous suction. Suction was not employed through the guide catheter.
As we gained experience and success utilizing the aspiration catheter, we bypassed the use of the Merci Retriever and even TPA in the last two cases in an attempt to expedite revascularization. Prior to treatment of patient #6, the Penumbra system became available at our institution.
Clinical variables and measurement of outcome
The medical history, physical examination, NIHSS and radiographic images were reviewed by an attending stroke neurologist (M.H., K.U., L.W., T.J.) upon admission (table 1). Radiographic outcomes were graded blindly according to the Thrombolyis in Myocardial Infarction (TIMI) and Thrombolysis in Cerebral Infarction (TICI) grading systems by a neurointerventional fellow (table 2).12 13 Clinical outcomes were graded according to the modified Rankin Scale (mRS) by a stroke certified registered nurse practitioner at 3 months (table 3).14
Demographic information
Procedural information
Outcome information
Results
Case 1
A 37-year-old woman with no significant past medical history (PMH) underwent a left sided craniotomy for resection of a peri-sylvian meningioma. Hours after waking neurologically intact, she developed a dense hemiparesis, gaze deviation and lethargy for an NIHSS of 20. She was taken for an urgent intervention. DSA revealed a distal BAO. After instillation of 4 mg TPA into the clot, two passes with the V2.5 soft retriever failed to restore flow. The DAC was advanced into the proximal clot followed by aspiration. Blood products were immediately aspirated into the syringe. After suction of ∼20 cc of blood, a control run through the DAC displayed a patent vessel with no residual stenosis or delayed perfusion (TIMI3/TICI3). At her 3-month follow-up, the patient exhibited full independence in activities of daily living (mRS 2).
Case 5
A 62-year-old man with a PMH of hypertension presented with dizziness, vertigo, nausea, vomiting, hearing loss, gaze paresis, dysarthria and progressive right hemiparesis (NIHSS 17). MRI/MRA/CTA confirmed a BAO with a left paramedian medullary infarct. He was taken to the angiography suite 15 h after the initial symptoms. DSA revealed a distal left VA occlusion with clot burden extending up to the origin of the superior cerebellar arteries. Due to the extent of thrombus, DAC aspiration was chosen first. Significant particulate thrombus was seen in the aspirate. The VA was now patent; however, a high-grade proximal basilar stenosis with distal occlusive thrombus was evident. After administering TPA into the thrombus, the stenosis was angioplastied with a 2.5 mm Voyager RX coronary dilation catheter (Abbott, Abbott Park, Illinois, USA). Due to residual clot in the distal basilar, the DAC was passed through the angioplastied segment for repeat aspiration. This resulted in complete recanalization of the vertebrobasilar system. Residual proximal BA stenosis was stented with a 3 mm×12 mm Multi-Link Vision coronary stent (Abbott). The final angiographic result was TIMI3/TICI3 flow. At 3-month follow-up, the patient was able to ambulate independently and carry out all activities of daily living alone, with disability caused by vertigo, dizziness, hearing loss and a left abducens palsy (mRS 2).
Case 6
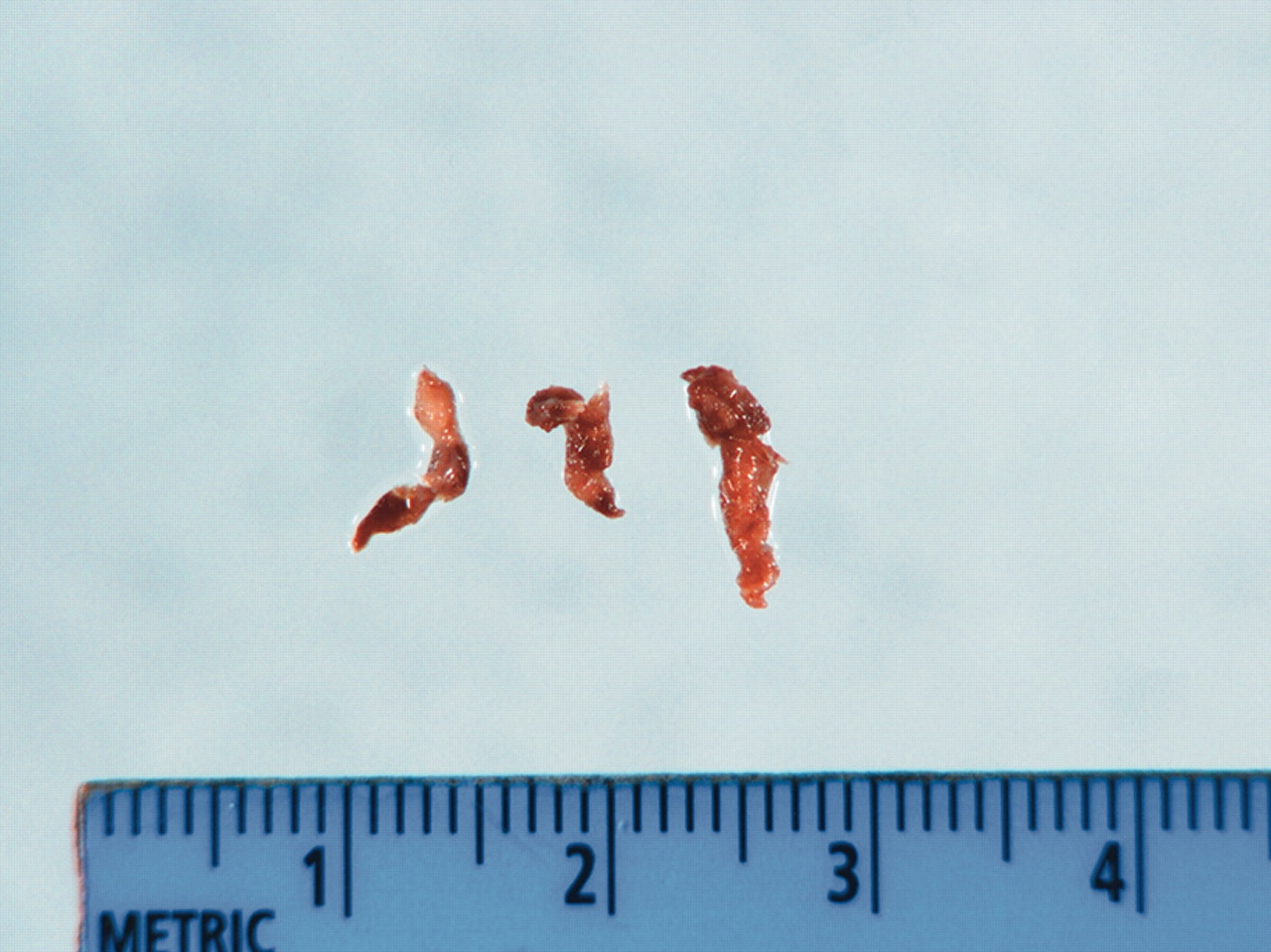
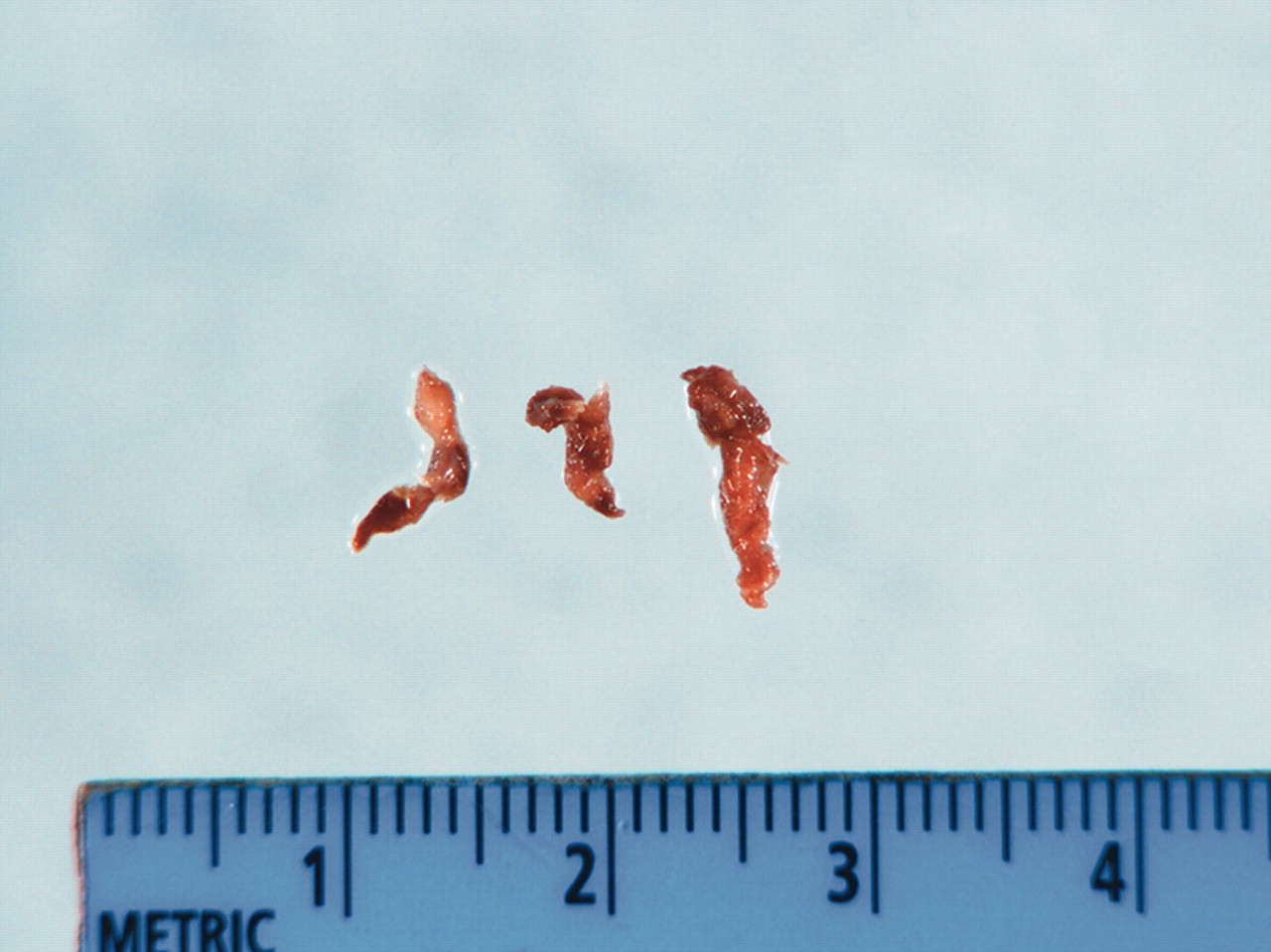
A 57-year-old man with no significant PMH presented with fluctuating hemiparesis and dysarthria. CTA confirmed a BAO. He was taken to the angiography suite 3 h after his last progressive symptomatic decline (NIHSS 15). DSA revealed a left VA origin high-grade stenosis with a concomitant mid-basilar occlusion (figure 1). After angioplasty of the VA stenosis with a 3 mm×15 mm Quantum Maverick balloon catheter (Boston Scientific, Natick, Massachusetts, USA), the 0.041 inch Penumbra aspiration catheter was advanced to the proximal clot interface. Ten minutes of suction aspiration with the 0.041 inch separator resulted in no flow. The DAC was then advanced into the proximal clot. Two repetitions of manual aspiration resulted in complete recanalization (figure 2). Three large fragments of thrombus were noted in the aspirate (figure 3). At 3-month follow-up, the patient remained dysarthric with resolving hemiparesis and was able to complete all activities of daily life (mRS 2).

Left vertebral artery injection showing a midbasilar occlusion. Note the 4.3F catheter tracking over an MC18L microcatheter in the distal left vertebral artery.

Left vertebral artery injection showing complete recanalization of the basilar artery after manual suction thrombectomy.
{kind=link}
{kind=link}
{kind=link}
Thromboembolism collected in the catheter aspirate.
Discussion
The cardiac literature provides the best data delineating the benefits of mechanical thrombus aspiration during revascularization procedures. In a prospective, randomized study, Burzotta et al15 showed that manual thrombus aspiration results in better angiographic and ECG myocardial reperfusion compared with standard PCI. Subgroup analysis showed that patients with lower TIMI scores and higher thrombus burden might have a greater benefit from thrombus aspiration. In another randomized trial, aspiration thrombectomy improved myocardial reperfusion when compared with standard stenting.16 The latter study only showed an improvement in perfusion, not TIMI scores, which highlights one important limitation of assessing success in stroke intervention; namely, that recanalization does not equal reperfusion. In the presence of large vessel occlusions, reperfusion is essential for preservation of brain tissue. This, in turn, is thought to be a prerequisite for favorable clinical outcomes. While reperfusion is most commonly achieved through arterial recanalization, it is important to recognize that recanalization and reperfusion are notions distinct from one another as not every instance of recanalization results in reperfusion just as not every instance of reperfusion is necessarily the consequence of recanalization. Reperfusion appears to be necessary for brain recovery but it is clearly not sufficient. Recanalization/reperfusion may not be beneficial and, due to an increased risk of hemorrhage, they may be detrimental if the territory supplied by the occluded vessel is already infracted. Furthermore, similar to the ‘no-reflow’ phenomenon encountered in the coronaries and believed to be caused by disturbed microcirculation, recanalization may occur without adequate tissue reperfusion. Greater reliance on the TICI grading system may focus attention on these outcome parameters as aspiration and the resultant decrease in clot burden may not only improve recanalization, but may also reduce distal micro-emboli and enhance perfusion.12
On the other hand, there is concern that aspiration may result in fragmentation of thrombus with distal embolization. While none of the patients described herein experienced this shortcoming, the number of treated patients is too small to allow any meaningful conclusions on the incidence of distal embolization with this technique. Potential methods to limit this problem include occlusion or flow reversal through the proximal balloon guide catheter.
There is a paucity of data regarding the utility of intracranial aspiration thrombectomy. A Medline search revealed few relevant published reports. There are scant published reports describing suction thrombectomy in large, extracranial vessels; however, these are limited to cervical ICA occlusion or near-occlusion.17 18 Nedeltchev et al19 describe two cases of basilar artery aspiration thrombectomy using a Tracker-38 catheter through a 7F guide catheter. They achieved complete recanalization utilizing simultaneous manual suction from the guide catheter and microcatheter. Chapot et al20 also describe the use of manual aspiration in the treatment of two patients with basilar artery occlusion using a 4F and 5F catheter to achieve complete and partial recanalization, respectively. They highlighted the need for favorable anatomy and fresh non-adhesive clot, the reduced time for recanalization, low hemorrhagic risk and possible prevention of distal clot migration.
The Penumbra System is a new FDA-approved embolectomy device designed to remove thrombus with aspiration and manual disruption-extraction. Initial reports were promising, with 100% recanalization rates of intracranial vessels which included the BA, ICA and middle cerebral artery.10 A more recent multi-center study of 125 patients with a large intracranial vessel exhibiting complete or near-complete occlusion treated within 8 h revealed 81.6% of patients were successfully revascularized to TIMI2 or 3.21 Of particular interest, all 11 patients with vertebrobasilar occlusions achieved TIMI2 or 3 recanalization. We have employed manual suction thrombectomy in preference to the Penumbra system mainly because the latter had not been available for use at our institution. It was only during the last intervention that we were able to utilize the device. We aborted use of the Penumbra system after only 10 min in favor of our standard protocol, primarily due to our inexperience with the device. As such, it should be emphasized that this current report does not intend to provide a comparison between two suction thrombectomy methods.
It should also be noted that all cases presented herein involved aspiration preceded by some form of mechanical clot manipulation. It is possible that the latter facilitated aspiration by disrupting the clot.
Theoretical advantages of our currently used approach include its rapidity of use because manual aspiration does not require connection to a pump. The 4.3F OD appears to balance trackability and utility. All catheters were easily advanced into the distal basilar artery in a tri-axial fashion. The 4.3F catheter also allows the procedure to be combined with mechanical thrombectomy by deploying the MC18L microcatheter and the Merci retriever through the catheter immediately pre- or postaspiration. As seen in the last patient, less reliance on thrombolytics may be possible to reduce the incidence of resultant hemorrhage. Additionally, continuous pump-driven suction as used in the Penumbra system may be associated with reduced flow though the occluded vessel as evidenced in a recent TCD-based study.22 Although the implications of these findings are uncertain, there is concern about prolonged near-reversal of flow in the distal vasculature throughout a pump-driven suction procedure.
Summary
Manual aspiration thrombectomy with a 4.3F catheter adds to the current armamentarium of existing recanalization methodologies. Our small case series indicates that its use can result in high rates of recanalization and consequently improved clinical outcomes compared with the historic data regarding the natural history of the disease.
Key messages
Basilar artery occlusion remains one of the most devastating subtypes of stroke. Intravenous and intra-arterial therapy have altered the natural history of this disease; however, clinical results remain poor, and exploring more aggressive management is warranted. Our small case series indicates that aspiration thrombectomy performed manually through a 4.3F catheter can facilitate recanalization of basilar artery occlusion with acceptable clinical outcomes.
References
Footnotes
Competing interests Jovin has received consulting and speaker fees from Co-Axia, ev3, and Concentric Medical.
Ethics approval This study was conducted with the approval of the IRB.
Provenance and peer review Not commissioned; externally peer reviewed.