Article Text

Abstract
Background and purpose Intracranial stenting with the Wingspan system has been used as a revascularization strategy in symptomatic patients with intracranial atherosclerotic disease (ICAD). The latest results of the Stenting versus Aggressive Medical Therapy for Intracranial Artery Stenosis (SAMMPRIS) trial challenge this approach. Our experience in the treatment of symptomatic ICAD with the Wingspan system is reported.
Materials and methods Patients who underwent stenting for symptomatic ICAD were included in the analysis. Demographic data, periprocedural complications, long term radiological and clinical outcomes are reported.
Results 46 lesions were treated in 45 patients. 13 patients (29%) presented with a transient ischemic attack and 32 (71%) with a stroke. 43 patients (95.5%) failed antithrombotic therapy at presentation. One (2%) symptomatic periprocedural (24 h) complication occurred. The 30 day incidence of stroke and vascular death was 6.6%—a fatal hemorrhagic stroke and two non-fatal hemorrhagic strokes. In-stent stenosis (≥50%) was seen in nine (42.8%) lesions, two were symptomatic.
Conclusions This cohort of patients with symptomatic ICAD who failed antithrombotic medications benefited from angioplasty and stenting with the Wingspan system.
Statistics from Altmetric.com
Introduction
Intracranial atherosclerotic disease (ICAD) causes between 8% and 10% of all transient ischemic attacks (TIAs) and strokes.1 Endovascular revascularization therapies such as angioplasty with or without stent deployment have emerged as alternative therapies. The only stenting system approved by the Food and Drug Administration (FDA) for the treatment of symptomatic ICAD is the self-expanding Wingspan stent system (Stryker, Fremont, California, USA). Retrospective registries have reported a 6% rate of periprocedural complications (ischemic and hemorrhagic stroke and death within 24 h).2–4 The 30 day incidence of stroke and death in these studies has ranged between 4.5% and 9.6%. These outcomes were deemed ‘acceptable’ compared with the natural history of the disease with only medical therapy. However, recent results from the Stenting versus Aggressive Medical Management for Preventing Recurrent Stroke in Intracranial Stenosis (SAMMPRIS) trial reported a 30 day rate of death or stroke of 14% in the stenting arm versus 5.8% in the solely medical therapy treatment arm.5 In light of the unexpected good performance of the medical therapy arm, and suboptimal outcome of the interventional arm, a new conservative approach has been adopted in the treatment of ICAD.
We report the immediate, periprocedural and short term follow-up results of our experience with the Wingspan system for the treatment of symptomatic ICAD who have failed antithrombotic medications.
Methods
Patient population
We reviewed the database of patients treated at the two participating institutions. Institutional review board approval was obtained for the study at each center. All patients with symptomatic ICAD who underwent angioplasty and stenting with the Gateway–Wingspan system under the FDA Humanitarian Device Exemption protocol were included. Patients who presented with an acute stroke and underwent emergent stent placement were excluded. The primary outcome was stroke and vascular death within 30 days of the procedure.
Patients were referred by a neurologist who considered that patients were symptomatic despite maximized medical treatment. For the most part, patients had to ‘fail’ at least one antithrombotic medication (warfarin, aspirin, clopidogrel or aspirin and dipyridamole) to be considered candidates for endovascular intervention. Lesions deemed appropriate for intervention had to be at least 50% of stenosis in the same vascular territory of the TIA or stroke at presentation. The degree of stenosis was quantified by catheter based angiography compared with a reference diameter of the normal proximal vessel, as described previously.6
Procedure
Patients were loaded with 600 mg of clopidogrel and 325 mg of aspirin 24 h before the intervention if they were not on dual antiplatelet therapy at least 3 days before the procedure. Briefly, a guiding catheter was advanced and positioned proximal to the target lesion. Angioplasty was performed with the Gateway balloon (Stryker) with nominal dilatation diameter calculated to 80% of the vessel diameter distal to the lesion. Subsequently, using an over the wire exchange technique, angioplasty was followed by deployment of the Wingspan stent. Stent size was calculated based on vessel diameter distal to the target lesion. Intravenous heparin was administered before stent deployment to achieve an activated clotting time >250 s. Post-stent angioplasty was performed in cases when the residual stenosis was >20%. Dual antiplatelet therapy was maintained for at least 3 months.
Evaluation and follow-up
Angiographic follow-up was obtained at 3–6 months, and at 12 months if possible. Otherwise clinical follow-up was obtained during the office visit or by telephone interview by a nurse practitioner or physician certified for assessing the modified Rankin Scale (mRS) score. A ≥50% stenosis was considered in-stent restenosis (ISR). Adjudication of all strokes and all other complications of stenting were performed by the study investigators only.
Results
Forty-five patients were included in the analysis and 46 target lesions were treated. Patient demographics are described in table 1. Thirteen patients (29%) presented with a TIA and 32 (71%) with a stroke.
Clinical and radiographic characteristics of the 45 patients
The mean time from presentation to intervention was 27 days (range 2–300 days). Forty-three patients (95.5%) were in some form of antithrombotic therapy at presentation. Two patients underwent intervention without a trial of antithrombotic therapy. The first patient was a 46-year-old man who presented with 80% stenosis of his left middle cerebral artery (MCA) and watershed zone infarcts. The second patient was a 66-year-old man who presented with a right pontine stroke and 95% stenosis of his distal right vertebral artery in the setting of occlusion of the contralateral left vertebral artery. Both patients had evolving neurological deficits despite optimal medical management and it was decided to perform stenting before a trial of antithrombotic medication.
Three (6.5%) asymptomatic procedural complications occurred: two flow limiting dissections that required stenting and one in-stent thrombosis that resolved with intra-arterial administration of 10 mg of abciximab.
One (2%) symptomatic reperfusion hemorrhage in the same territory of the stented vessel occurred 2 h after the intervention. The 30 day overall incidence of stroke and death was 8.9%: one non-vascular death, a hemorrhagic stroke that ultimately caused death and two non-fatal hemorrhagic strokes (table 2). One patient died with hospital acquired pneumonia despite successful endovascular treatment. Thus the 30 day incidence of stroke and vascular deaths was only 6.6%. One patient who presented with a TIA underwent stenting of an 80% right MCA stenosis. He died 4 days later with a massive intracerebral hemorrhage (ICH) after stopping his antihypertensive medications despite medical orders. One patient developed a small symptomatic basal nuclei hemorrhage 2 h after stenting of an 80% left MCA stenosis. Despite initial worsening of her neurological condition, she returned to baseline after 3 weeks in rehabilitation. The second non-fatal ICH occurred in a 46-year-old woman who underwent stenting of a 90% stenosis of her left MCA due to TIAs despite dual antiplatelet medication. A few hours after the procedure she developed aphasia due to a subarachnoid hemorrhage.
Clinical and radiological outcomes
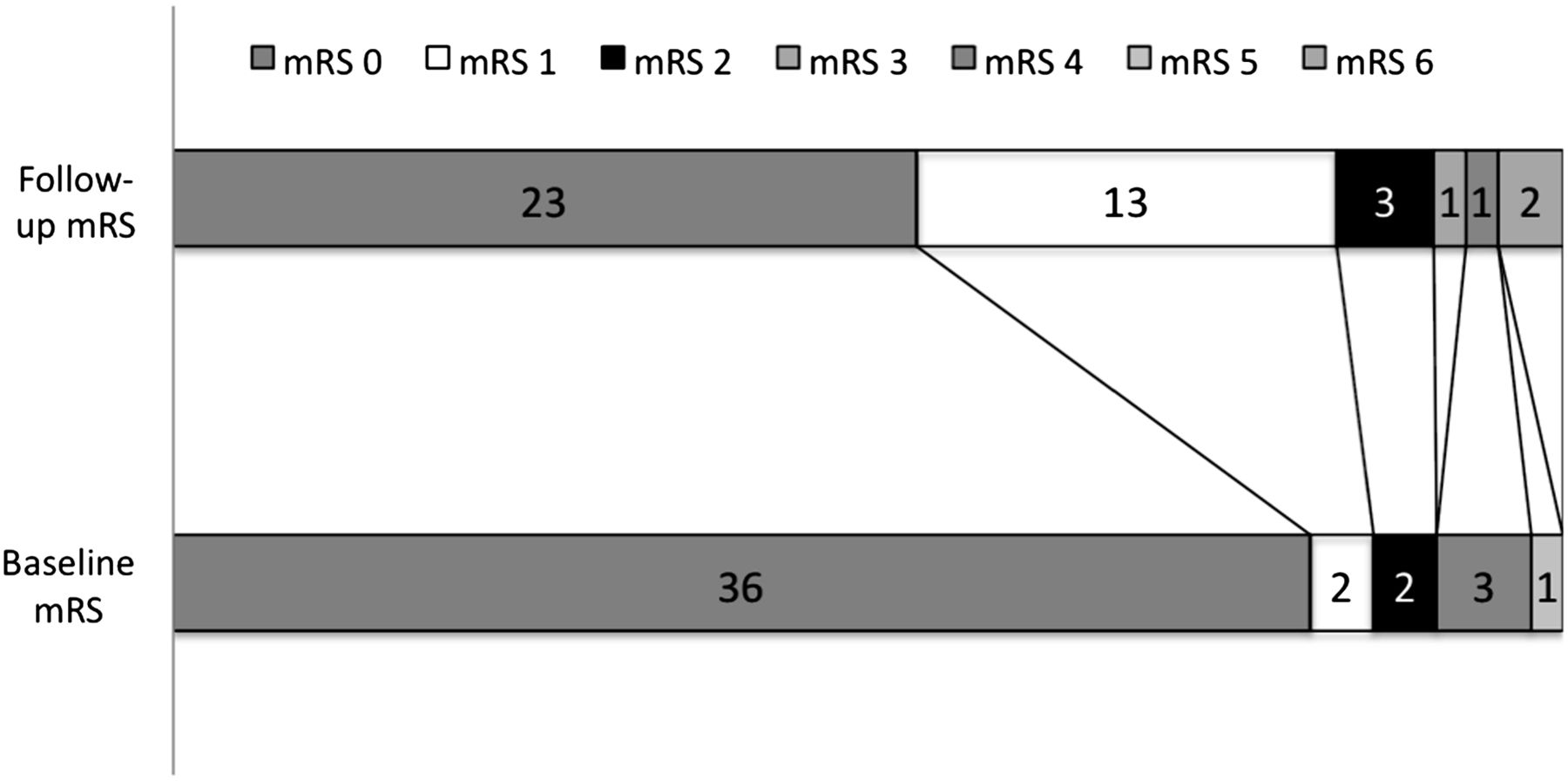
Two patients were lost to follow-up. One additional stroke in the territory of the stented artery occurred beyond 30 days. However, angiography did not demonstrate ISR. Mean follow-up time was 10 months (range 0.5–37 months). Thirty-six (85.7%) patients did not have significant disability (mRS 0 and 1) on follow-up compared with 38 (86.3%) patients at presentation (figure 1). One patient who presented with severe disability (mRS=5) had minimal symptoms on follow-up (mRS=1). One patient who presented with TIAs (mRS=0) died after the procedure. A patient who presented with TIAs and underwent stenting of a 75% MCA stenosis had moderate disability (mRS=3) on follow-up due to bilateral subdural hematomas from unrelated trauma.

{kind=link}
Modified Rankin Scale (mRS) scores at presentation and at follow-up: mean follow-up was 10 months.
Follow-up angiography was performed in 21 (46.6%) patients at a mean of 10.6 months after stenting (range 2–37 months). ISR (≥50%) was seen in nine (42.8%) lesions (1=50%, 2=70%, 1=75%, 1=80%, 2=90% and 2=100%). Two patients were symptomatic. The first patient stopped taking clopidogrel and experienced TIAs. An angiogram demonstrated 70% ISR. Symptoms resolved after an angioplasty was performed 7 months after the initial stenting. The second patient presented 4 months after the procedure with TIAs. An angiogram demonstrated 90% ISR of the previously stented MCA. After angioplasty her symptoms resolved. Two in-stent occlusions were documented in asymptomatic patients during routine follow-up angiograms performed 2 and 8 months after stenting. Collateral flow developed since the time of stenting in these two patients.
Discussion
The technical feasibility and safety of stenting with the Wingspan system has been demonstrated in this and other reports with ‘acceptable’ periprocedural complication rates between 2% and 6%.2–4 7–9 The 30 day incidence of stroke and vascular death encountered in this study (6.6%) resembles previous retrospective case series and registries (table 3).3 ,4 ,10 Overall, this is lower than the 30 day rate of stroke and death of 10.7% in the Warfarin–Aspirin Symptomatic Intracranial Disease trial (WASID; Clinical Trials.gov number NCT00004728). Previous reports describing the experience with the Wingspan system in the treatment of symptomatic ICAD sparked enthusiasm among the neurointerventional community. However, recent results from SAMMPRIS which demonstrated a 14.7% rate of 30 day stroke and death do not seem to justify stenting over medical management.
Comparison of different series that utilized the Wingspan system in the treatment of symptomatic intracranial atherosclerotic disease
In contrast with SAMMPRIS where only 64.7% of patients were already receiving antithrombotic therapy at the time of the qualifying event, almost all patients (95%) treated in our study ‘failed’ antithrombotic therapy at the time of intervention. This is similar to the prospective multicenter single arm study by Bose et al that led to limited FDA approval of the Wingspan system.4 Patients with ≥50% stenosis who failed antithrombotics were treated, and the 30 day ipsilateral stroke and death rate was 7%. The heterogeneity of the patient populations and study designs does not allow any solid comparisons. However, our results and the initial study by Bose et al suggest that stenting may be the last option for patients who continue to experience strokes despite treatment with antithrombotics.
Despite the great results of the medical arm of SAMMPRIS, it may be difficult to achieve and replicate such targeted medical goals: low density lipoprotein <70 mg/dl, systolic blood pressure <140 mm Hg (<130 mm Hg in diabetics) and lifestyle program modification. This is particularly challenging in metropolitan areas with a large non-compliant patient population. This is reflected in the low rate of follow-up angiograms (46.6%) performed in our study.
The overall clinical outcome at follow-up was favorable. Two patients experienced TIAs after the initial 30 days due to ISR and were successfully treated with angioplasty. Another patient suffered a small cerebellar infarct 2 months after the procedure. Interestingly, repeat cerebral angiography revealed no evidence of ISR. The degree of disability at presentation and follow-up was the same (figure 1) despite the high incidence of stroke (71%) as the qualifying event in our cohort.
The rate of ISR in our series (42%) is higher than what has been reported in other post-marketing series (25–29.7% at 6 months).2 ,10 ,11 However, only two patients (9.5%) were symptomatic (70% and 90% ISR). Interestingly, two patients had complete stent occlusion and three had severe ISR (1=80% and 2=90%) in routine follow-up angiograms. These patients were asymptomatic and their angiograms demonstrated development of collateral flow to supply the vascular territory of the occluded artery. In these cases, stenting may have worked as a bridging therapy for the development of collaterals.
Symptomatic ICH, whether due to vessel perforation or reperfusion, appears to be a major concern in the periprocedural period. In our cohort, one periprocedural reperfusion hemorrhage occurred 2 h after the intervention. Similarly, SAMMPRIS reported nine symptomatic periprocedural ICHs, and previous studies have reported rates of between 50% and 60%.2 ,3 ,10 We did not experience any perforation but two patients suffered symptomatic reperfusion hemorrhages 2 and 72 h after the procedure. As operators continue to gain familiarity with new devices, the rate of periprocedural complications such as wire perforations continues to decline (table 3).
This study has the same limitations encountered in previous retrospective studies and registries. Data were not acquired in an unbiased and blinded manner. Adjudication of degree of stenosis, periprocedural complications, occurrence of ipsilateral strokes in the treated vessel and evidence of ISR were performed by the study investigators and not by unbiased independent collaborators. Moreover, follow-up angiograms were acquired in only 46.6% (21/45) of patients.
Two retrospective studies comparing stenting and medical therapy to solely medical therapy in the treatment of symptomatic IAD showed similar ischemic event rates in both cohorts.12 ,13 Furthermore, Kaplan–Meier analysis of both groups demonstrated similar event rates in long term follow-up. Whether these findings will be replicated in SAMMPRIS has yet to be determined.
References
Footnotes
-
Competing interests None.
-
Ethics approval Ethics approval was provided by the institutional review board committee.
-
Provenance and peer review Not commissioned; not externally peer reviewed.