Article Text

Abstract
Currently in use by interventional cardiology for the intravascular evaluation of coronary arteries, optical coherence tomography (OCT) has proven to be effective in the evaluation of atherosclerotic disease and further therapeutic management. We report a novel use of OCT technology in the case of a 46-year-old man with sudden onset blurred vision and greater than 70% stenosis of his left vertebral artery. To date, no detailed descriptions or case reports have previously been reported regarding the use of neuroendovascular OCT in diseased arteries.
- Angiography
- Atherosclerosis
- Intervention
- Stent
- Stenosis
Statistics from Altmetric.com
Introduction
Optical coherence tomography (OCT) is an established medical imaging technique used to obtain in vivo high resolution images of biological tissue. Currently it is used in a wide array of applications, notably in ophthalmology where it provides high resolution images of the retina, and more recently in interventional cardiology for the intravascular evaluation of coronary arteries. Utilizing coronary artery data, one can theoretically extrapolate from the cardiology literature and apply it to the vertebral arteries in regards to characterization of atherosclerotic plaque as well as stent assessment. In this article, we aim to depict a novel use of intravascular OCT in the vertebral arteries.
Case report
A 46-year-old Caucasian man presented with sudden onset blurred vision lasting for 10–15 min on at least three separate occasions prior to seeking medical attention. The past medical history was significant for hypertension, obstructive sleep apnea, obesity, and gout. He drinks alcoholic beverages once a week socially but denies smoking or other illicit drug use. Home medications included amlodipine 10 mg daily, lisinopril 40 mg daily, and allopurinol 300 mg daily.
During hospitalization, a lipid profile disclosed a slightly elevated total cholesterol and low density lipoprotein of 210 mg/dl and 146 mg/dl, respectively. Admission MRI of the brain with MR angiography of the head and neck arterial system demonstrated a significant stenosis of approximately 70% at the origin of the left vertebral artery without evidence of acute cortical infarct, additional stenoses, or dissection. Based on his age and symptoms, and after optimizing medical therapy, including starting the patient on 75 mg of clopidogrel daily and titrating his dose of simvastatin from 10 mg daily after discharge from the hospital to an eventual dose of 40 mg daily, a more aggressive course of action was planned by his neurologist.
The patient subsequently presented to the neurointerventional suite for a cervical angiogram with the intent of endovascular treatment of the left vertebral artery stenosis. Angiography demonstrated severe stenosis at the origin of the left vertebral artery measuring >75% (figure 1). No collateral vessels were identified and the diminutive contralateral right vertebral artery was otherwise unremarkable. Thereafter, an 8 F guide catheter was placed in the left subclavian artery for support. A Medtronic 3.0 mm×12 mm balloon mounted stent delivery system was then navigated to the stenosis in the proximal left vertebral artery and deployed under live fluoroscopy. Repeat cervical angiogram status post angioplasty and stent placement, in conjunction with images obtained from the OCT catheter (Light-Lab; St Jude Medical, St Paul, Minnesota, USA), demonstrated satisfactory placement of the stent as well as marked interval improvement of the proximal left vertebral artery to less than 5% residual stenosis compared with the midcervical segment (figure 2A). The OCT catheter was repositioned and diagnostic images were subsequently acquired (figure 2B, 2C). The patient encountered no complications during the procedure and was discharged home the next morning after an uneventful night.
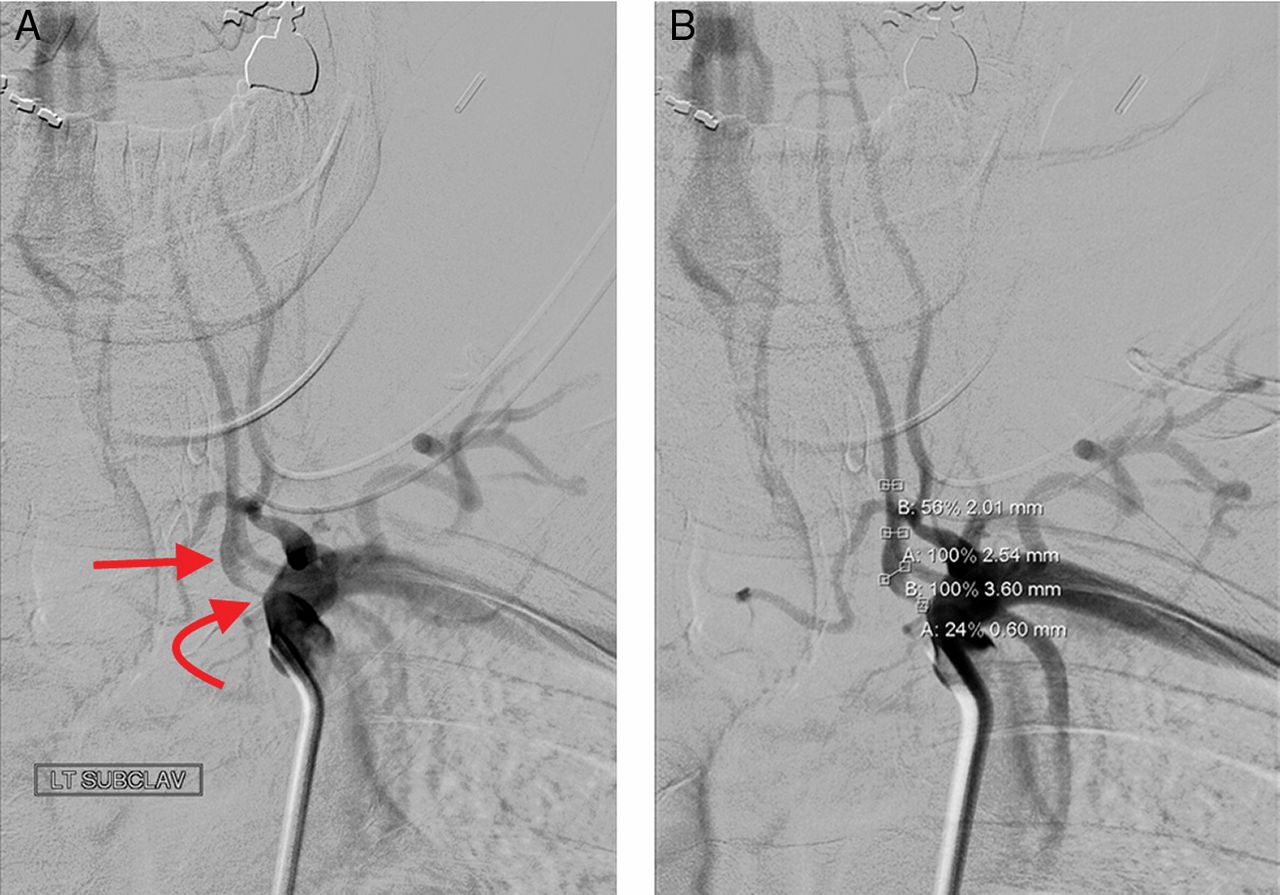
Digitally subtracted anteroposterior angiogram over the left chest and neck. (A) The proximal left subclavian artery is widely patent with no narrowing or stenosis. Note is made of a severe stenosis at the origin of the left vertebral artery measuring >75% (curved arrow). Post stenotic dilatation of the proximal cervical left vertebral artery is seen (arrow). The remainder of the visualized mid to distal cervical left vertebral artery is within normal limits. (B) Corresponding digital subtraction angiography of the left subclavian artery with measurements—proximal left vertebral artery (0.60 mm), post stenotic dilatation of the proximal cervical left vertebral artery (3.60 mm) and midcervical left vertebral artery (2.01 mm).

Post stent inspection of the left vertebral artery by optical coherence tomography (OCT), from distal to proximal. (A) Cervical angiogram status post angioplasty and stent placement demonstrates satisfactory placement of the stent as well as <5% residual stenosis within the proximal left vertebral artery (2.18 mm) compared with the midcervical left vertebral artery (2.25 mm). (B) Longitudinal OCT image of the left vertebral artery from distal to proximal with respective cross sectional images, I–IV. (C) Cross section OCT images demonstrate (I–IV from midcervical left vertebral artery to the origin of the left vertebral artery): I, non-diseased midcervical left vertebral artery with a mean diameter of 2.82; II, distal stent malapposition relative to the wall of the left vertebral artery (*). Native artery lumen of 3.35 mm compared with inner stent lumen with a mean diameter of 2.69 mm; III, better apposition of the stent struts relative to the diseased proximal left vertebral artery (2.49 mm compared with 2.39 mm); IV, heavily diseased origin of the left vertebral artery with demonstration of residual white thrombus between the stent and the native arterial wall (curved arrows).
Discussion
Analogous to intravascular ultrasound (IVUS), OCT is a minimally invasive catheter based imaging modality that provides a cross sectional view of the artery being interrogated. Images generated utilizing OCT are based on the emission of near infrared light which enables 10–25 times higher in vivo resolution imaging of the arterial wall, of the order of 10–20 μm, about twice the size of a red blood cell. Clinically this translates to tissue penetration of 1–3 mm compared with the 4–8 mm achieved by IVUS.1 ,2 The spatial resolution yielded from OCT exceeds what is possible with routine imaging methods such as from catheter directed angiography or even non-invasive CT angiography or MR angiography.
Intravascular OCT utilizes a single fiberoptic wire to emit light at a bandwidth in the near infrared spectrum with central wavelengths of approximately 1300 nm. The images are then generated when back scattered or reflected light from the target tissue produces a measurable signal intensity and echo time delay.3 The single fiberoptic image wire is designed to handle both light emission as well as record the reflection or backscatter of light. Two main technologies are utilized to obtain these OCT images, frequency domain and time domain OCT systems, with the latter using a moving reference mirror to obtain images at varying tissue depth. By simultaneously scanning through the entire bandwidth of near infrared wavelengths and in turn analyzing thousands of data points or echo time delays, frequency domain OCT imaging technology is significantly faster than analyzing the tissue point by point as in time domain OCT.4
The single fiberoptic image wire used to acquire the OCT images rotates inside an over the wire catheter with an external lumen of 0.019 inch and is designed to be compatible with a standard 0.014 inch microwire and 6 F guide catheter for easy adoption. During image acquisition, blood in the field of view can cause significant signal attenuation and artifact whereby necessitating clearing of blood from the lumen of the artery. Initial experience with earlier generation OCT catheters within the coronary arteries suggests this can be resolved by proximal balloon occlusion with subsequent infusion of saline or Ringer's lactate at a rate of 0.5–1.0 ml/s. It is recommended that a power injector be used to maintain a constant rate; furthermore, multiple pullbacks can be made in order to completely evaluate the complete extent of the lesion at a rate of approximately 0.5–3.0 mm/s. Balloon occlusion can affect image clarity primarily by inadequate clearing of blood from the field of view. Other limiting factors include lesions exceeding 30 mm in length.5 Non-occlusive techniques with newer generation catheters have recently been developed and studied where simultaneous infusion of viscous iso-osmolar contrast agents and pull back of the image wire/catheter system are employed so as to reduce imaging time and increase clearing of blood from the lumen.
Morphological characteristics of atherosclerosis by OCT have been well studied in the coronary arteries. Precise high resolution visualization and quantification of the thickness of the fibrous cap and calcium are possible and well documented. However, it should be noted that light absorbed by lipid pools, which is sharply demarcated from the overlying signal rich fibrous cap, acts as a diffuse signal poor region making the extent difficult to quantify. Plaque rupture and/or ulceration can be detected by OCT as an area of contiguity between the lipid pool and the fibrous cap at a rate similar to that of pathologic studies5 (figure 3A). Kume et al suggested possible discrimination of red and white thrombus with the aid of OCT, as confirmed by histopathologic correlation6 (figure 3B, 3C).

{kind=link}
{kind=link}
{kind=link}
Cross sectional optical coherence tomography (OCT) images of diseased coronary arteries. (A) Large ruptured plaque is noted with demonstration of contiguity between the overhanging thin fibrous cap (curved arrow) and the lipid pool (arrow). (B) Red thrombus (curved arrow) causes marked signal attenuation owing to the presence of red blood cell components. (C) Contrary to this, white thrombus (curved arrow) is platelet rich and exhibits lower signal attenuation than that of red thrombus. Also on this image, superiorly located, is a sharply demarcated curvilinear low attenuating calcified plaque (arrow). (D) OCT imaging clearly demonstrates good apposition of the stent struts in relation to the diffusely thickened arterial wall.
Similar to IVUS, but at a higher spatial resolution, information yielded from the OCT cross sectional view of a diseased artery cannot only aid in lesion assessment prior to intervention but furthermore in proper stent sizing prior to deployment. Likewise, discrepancies between degrees of stenosis by different imaging modalities can be resolved.7 ,8 One may underestimate the size of a diseased artery when using only conventional angiographic techniques as this measures only luminal diameter. Conversely, because of the accurate measurements of both the luminal stenosis as well as the true diameter of the artery, one can choose the correct balloon or stent size when utilizing OCT. In addition, the precise length of the diseased stenotic area can be assessed so that a proper stent length may be determined ahead of time. In doing so, this can reduce the need for overlapping stents which are known to increase the risk of thrombosis.9 After selecting a proper stent, in conjunction with OCT, one can confirm optimal stent placement and stent wall apposition, as well as ensuring full expansion of the stent, thereby reducing complications such as the incidence of in-stent thrombosis. Once the stent has been implanted, OCT can clearly demonstrate the stent struts in relation to both the arterial wall and plaque (figure 3D). When compared with IVUS, OCT demonstrates higher sensitivity in assessing strut apposition.10 ,11 Furthermore, if there is any area that requires further attention post stent deployment, a larger balloon can be directed to the area of concern so as to optimally expand the stent.
The surgical approach to the vertebral arteries is difficult and therefore in cases of stenosis, such as in our case, intravascular stenting is a very attractive option; albeit, a disproportionately high in-stent restenosis rate has been observed within the vertebral arteries which has been attributed to a wide variety of factors. One of the causes of in-stent thrombosis or restenosis in neurovascular stenting may be poor stent apposition, such as when the stent may not have been fully expanded to the width of the artery. A direct correlation between rates of in-stent restenosis with the length of an atherosclerotic lesion was seen in one series of 88 patients with 90 lesions by Lin et al.10 Another key contributor to in-stent restenosis is intimal hyperplasia, with robust evidence demonstrating lower rates of restenosis associated with drug eluting stents compared with bare metal stents.12 ,13
Other potential cerebrovascular applications that may be amenable to and benefit from intravascular high resolution OCT cross sectional images are varied.14 Mathews et al recently reported on the clinical feasibility of neuroendovascular OCT within non-diseased arteries of the intracranial circulation in three human cadaveric patients and two pigs with corresponding ex vivo tissue samples for histologic comparison.15 Studies such as Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy (SAPPHIRE) as well as the Carotid Revascularization Endarterectomy versus Stenting Trial (CREST) have increased the use of stents within stenotic carotid arteries with relatively low complication and restenosis rates.16 ,17 Poor stent approximation has been noted as a cause for restenosis; however, with OCT guidance improved stent placement as well as better patient risk stratification may be possible. Intracranial artery stenosis, unruptured aneurysms and even arteriovenous malformations are areas in which future applications of OCT imaging technology may prove to be a powerful diagnostic modality in the neurointerventionalist's armamentarium.
References
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The author list has been reordered to reflect Daniel P Hsu as senior author.
-
Contributors All authors provided substantial contributions to the conception and design as well as the acquisition and interpretation of the data; drafting the article or revising it critically for important intellectual content; and final approval of the version to be published. IJP and DPH are the designated guarantors and take full responsibility for the integrity of the work as a whole, from inception to published article.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval The study was approved by the institutional review board.
-
Provenance and peer review Not commissioned; externally peer reviewed.