Article Text

Abstract
Introduction Haemorrhagic transformations are pejorative for patients with acute ischaemic stroke (AIS). We estimated flat-panel CT performances to detect brain parenchymal hyperdense lesions immediately after mechanical thrombectomy directly on the angiography table in patients with AIS, and its ability to predict haemorrhagic transformation. We also evaluated an easy-reading protocol for post-procedure flat-panel CT evaluation by clinicians to enable them to determine the potential risk of haemorrhage.
Methods Two neuroradiologists retrospectively reviewed post-procedural flat-panel CT and 24 h follow-up imaging. We evaluated hyperdense lesions on flat-panel CT to predict the occurrence of haemorrhagic transformation within 24 h detected with conventional imaging.
Results Of 63 patients, 60.3% presented post-procedural parenchymal hyperdensity and 54.0% had haemorrhagic transformation. Significantly more patients with hyperdense lesions on post-thrombectomy flat-panel CT presented haemorrhagic transformation (84.2% vs 8.0%; p<0.0001). No significant haemorrhagic transformations were detected for patients without parenchymal hyperdensity. Sensitivity and specificity of hyperdense lesions on flat-panel CT for the prediction of haemorrhagic transformation were 94.1% (80.3–99.3%) and 79.3% (60.3–92.0%), respectively. The positive and negative predictive values for the occurrence of haemorrhage were 84.2% (68.8–94.0%) and 92.0% (74.0–99.0%), respectively. For significant parenchymal haemorrhage type 2, sensitivity and negative predictive values were 100%. We observed good homogeneity between the different readers. Hyperdensity on post-procedural flat-panel CT was associated with a tendency for higher risk of death and lower risk of good clinical outcome.
Conclusions Flat-panel CT appears to be a good tool to detect brain parenchymal hyperdensities after mechanical thrombectomy in patients with AIS and to predict haemorrhagic transformation.
- Stroke
- Hemorrhage
- CT
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy is becoming more frequently used to recanalise intracranial arteries in patients with acute ischaemic stroke (AIS). This treatment can result in recanalisation rates as high as 79% and around 40% of patients achieve good clinical outcomes1. However, loss of integrity of the blood–brain barrier (BBB) resulting from ischaemia/reperfusion can lead to haemorrhagic transformations, which are observed in 22–29%1–3. Predicting haemorrhagic transformation is critical in the setting of therapy for AIS.
Immediately after completion of mechanical thrombectomy, in most institutions, a non-enhanced CT scan is performed to assess potential haemorrhagic complications4 ,5. In our institution, we perform a CT-like control at the end of the treatment with a C-arm-mounted flat-panel detector immediately after completion of the procedure, on the angiography table. This flat-panel CT technology allows the detection of haemorrhagic lesions6–8. Nevertheless, to the best of our knowledge, flat-panel CT has not been evaluated for BBB detection in the setting of AIS. The aim of this study was to evaluate the ability of flat-panel CT to detect BBB rupture after mechanical thrombectomy in patients with AIS to predict haemorrhagic complications. We also evaluated an easy-reading protocol for post-procedure flat-panel CT analysis to be used by non-radiologists for management in the acute setting.
Methods
Study population
We retrospectively reviewed the radiological records of all patients with AIS treated with mechanical thrombectomy and with post-procedure flat-panel CT. Patients were identified from a prospective clinical registry of patients with AIS who were treated between January 2009 and November 2011 at our institution. All patients with proximal arterial occlusion were referred for mechanical thrombectomy. Age was not a contraindication for mechanical revascularisation. Patients with a National Institutes of Health Stroke Scale (NIHSS) score <6 for the anterior circulation and patients with spontaneous NIHSS improvement were not included. Patients presenting within 4.5 h from symptom onset were initially treated with intravenous thrombolysis (recombinant tissue plasminogen activator 0.9 mg/kg) before mechanical recanalisation. Patients presenting after 4.5 h or with unknown symptom onset were treated with thrombectomy alone and an MRI scan was systematically performed to detect positive lesions on fluid attenuated inversion recovery (FLAIR) sequence. In patients with a positive FLAIR sequence, mechanical recanalisation was not attempted and these patients were not included in the study. The time window for anterior circulation strokes was up to 8 h after symptom onset. For patients with posterior circulation strokes, a combined approach was performed up to 24 h, depending on the extent of the ischaemic lesions and the clinical status.
Data collection and definitions
Patient demographics, imaging findings, vital signs before treatment, severity of ischaemic stroke and clinical outcomes were collected using a structured questionnaire. The severity of ischaemic stroke was assessed by NIHSS score. Time from symptom onset (or time from when the patient was last seen in a healthy condition) to initiation of treatment was also recorded. All patients had a post-procedural flat-panel CT and a follow-up CT or MRI scan 24 h after starting treatment. Symptomatic intracerebral haemorrhage was defined as a haemorrhage seen on the follow-up CT/MRI scan associated with an increase of at least four points in the NIHSS score according to the European Cooperative Acute Stroke Study (ECASS) criteria9. All mechanical revascularisation procedures were performed under general anaesthesia. In all cases, the device used for mechanical endovascular treatment was a stent retriever, Solitaire FR revascularisation device (EV3, Irvine, California, USA). During endovascular procedures, recanalisation was monitored and the time to recanalisation was noted at the end of the procedure. Recanalisation was considered achieved when Thrombolysis in Cerebral Infarction (TICI) score was 2b (partial) or 3 (complete). After the procedure the patients were admitted to the intensive care unit. Functional outcome was assessed at 3 months by a senior vascular neurologist using the modified Rankin scale (mRS) dichotomised into favourable (mRS 0–2) and unfavourable (mRS 3–6) outcomes. Our institutional ethical committee approved the study.
Imaging protocol and analysis
The flat-panel CT acquisition protocol and post processing were embedded in two different angiographic systems (FD20 and FD20/10 Allura Interventional Angiographic Systems, Philips Healthcare, Best, The Netherlands)10–12. The imaging systems consisted of a motorised rotational movement (so-called propeller scan) of a C-arm in the plane perpendicular to the longitudinal table axis around the head of the patient positioned at the system isocenter, which acquired 620 fluoroscopic frames in a circular motion at a frame rate of 30 frames/s, total rotation time of 20 s, over an angle of 240° (±120°) with a rotation speed of 22°/s, using a 1024×1024 pixel matrix detector with a 48 cm field of view. Different types of image post processing (beam hardening and scatter corrections) were applied to achieve maximum spatial and contrast resolution qualities. Additional reconstructions could be performed with variable volume matrixes or dimensions of reconstructed volume (5123 spatial resolution matrix as a maximum). Once displayed on the three-dimensional monitor, the reconstructed results could be rotated, zoomed and panned, and furthermore, displayed in different volume rendering formats and display modes (multiplanar reconstruction or single slice view). Maximum intensity projection thickness could vary from 1 to 100 mm according to the physician's wish (in most instances, a 2–5 mm thickness was chosen).
For the purpose of this study, two investigators (a board-certified neuroradiologist and a neuroradiology fellow) who were blinded to the follow-up imaging (not analysed in the same time) and clinical data independently and retrospectively reviewed the post-procedure flat-panel CT on a dedicated workstation (Xtravision, Philips Healthcare, The Netherlands). They focused on the presence or absence of any visible hyperdense intracranial lesion to achieve a rapid, simple and easily reproducible analysis of the examination. We divided the patients into those with and without hyperdense brain parenchymal lesions on the post-procedure flat-panel CT. After independent analysis, any differences in opinion were analysed to find a consensus between both investigators. To evaluate the ability of a non-radiologist physician to detect hyperdensities on post-procedure flat-panel CT scans, an intensivist physician independently reviewed all the flat-panel CT scans. This analysis by the intensivist physician was performed with a non-dedicated workstation with no possibility of adapting slice thickness, spacing or measuring density in Hounsfield units.
All patients were followed up with a conventional CT or MRI with a T2* sequence, performed within 24 h of mechanical thrombectomy to detect any haemorrhagic transformation, which was defined as any parenchymal hyperdensity on the 24 h follow-up CT or any hyposignal on the MRI T2* images3 ,5 ,13. Haemorrhagic transformations were evaluated in accordance with the ECASS criteria9. Significant haemorrhage was defined as parenchymal haemorrhage type 2 (PH-2) or confluent haematoma with a significant mass effect that compressed and displaced the surrounding brain parenchyma3 ,14.
Statistical analysis
Patient demographics and stroke characteristics and outcomes are presented as median (range) for continuous variables and percentage (number) for dichotomous variables for all study samples and according to the presence of brain parenchymal hyperdense lesions detected on post-procedural flat-panel CT. Bivariate comparisons were done using the Mann–Whitney U test for continuous variables and the χ2 test for categorical variables (or using Fisher's exact test when the expected cell frequency was <5).
For the analysis of flat-panel CT, inter-observer reliability was assessed using a κ test. For the analysis of the post-procedure flat-panel CT by the intensivist physician, we performed a κ test using the consensus data of the two neuroradiologists as the reference. The sensitivity, specificity, positive predictive value and negative predictive value of flat-panel CT for the prediction of haemorrhagic transformation were calculated and expressed with exact CIs. Statistical analyses were performed using commercially available software (SPSS release V.10.0).
Results
During January 2009 to November 2011, mechanical thrombectomy and immediate flat-panel CT were performed for 63 patients. The baseline characteristics of the 63 patients are shown in table 1, along with time to recanalisation, recanalisation findings and 3-month outcomes. Satisfactory revascularisation status (TICI grade ≥2b) was achieved in 82.5% of patients. Flat-panel CT was not taken into account to adapt adjuvant treatments. Regarding baseline characteristics of patients, NIHSS at inclusion, previous intravenous thrombolysis, number of passes of the stent-retriever device (SolitaireFR; ev3 Inc, Plymouth, Minnesota, USA), endovascular procedure duration, time from symptom onset to recanalisation, and TICI score at the end of the procedure, there was no statistically significant difference between the two groups of patients according to the presence or absence of brain parenchymal hyperdensity on post-procedural flat-panel CT (table 1). Detection of hyperdense lesions on post-procedural flat-panel CT was associated with a tendency for higher risk of death (34.2% vs 25.0%, OR=2.08; 95% CI 0.63 to 6.82; p=0.23) and lower risk of good clinical outcome (36.8% vs 56.0%, OR=0.46; 95% CI 0.16 to 1.28; p=0.14).
Baseline patient characteristics and recanalisation findings
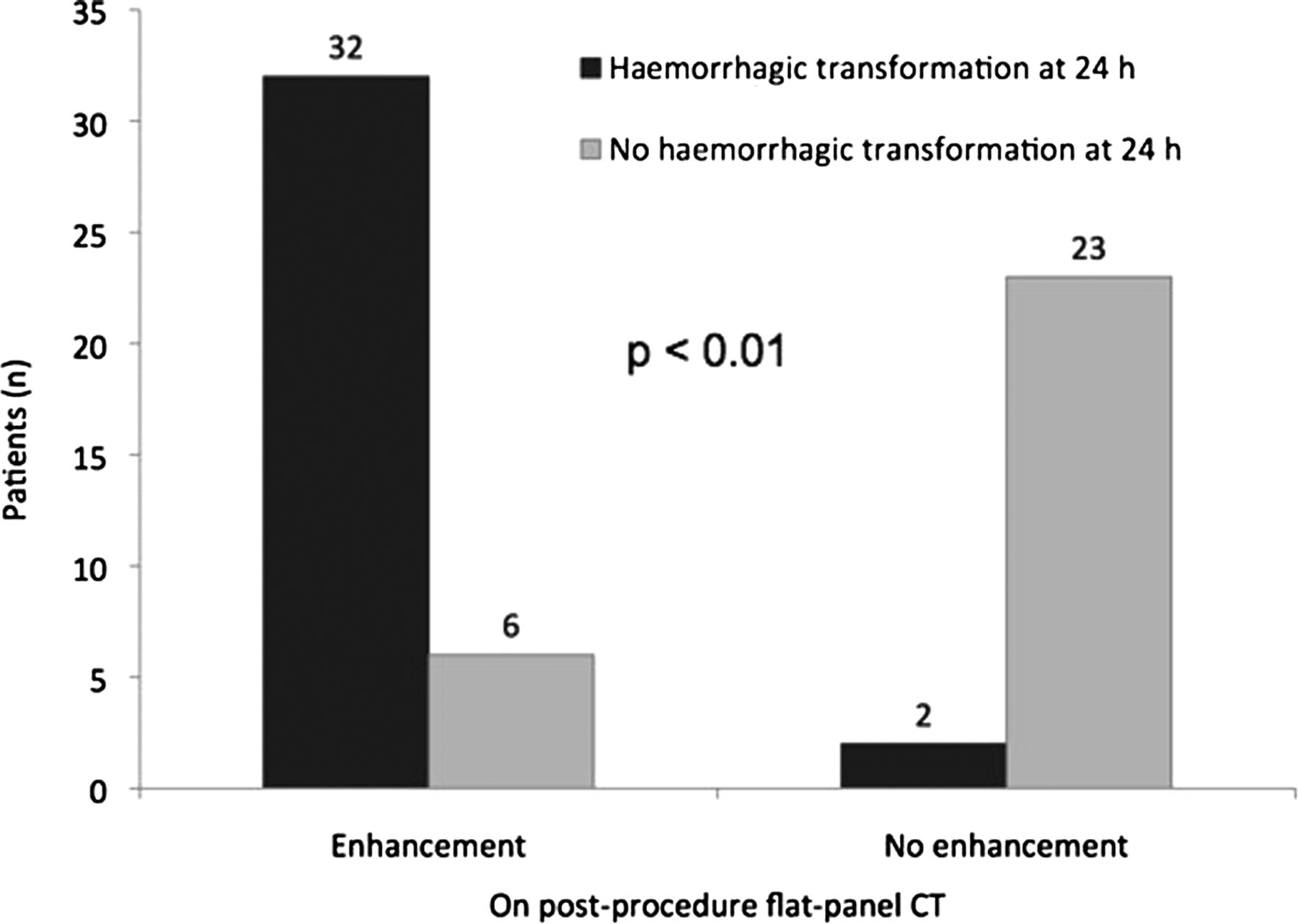
Of the 63 patients, 38 (60.3%) had hyperdense lesions on the post-procedure flat-panel CT. At 24 h, 38 (60.3%) patients underwent conventional non-enhanced CT and 25 (39.7%) underwent MRI. Follow-up imaging detected haemorrhagic transformation in 34 patients (54%). Significantly more patients who had hyperdense brain parenchymal lesions on post-procedural flat-panel CT subsequently had haemorrhagic transformation (32/38 (84.2%) vs 2/25 (8.0%) without hyperdensity; p<0.0001; figure 1). Significant haemorrhage (PH-2) was detected at 24 h follow-up in 11/38 (28.9%) patients with hyperdensity and no patients without (p=0.002). Both of the patients without enhancement but with haemorrhagic transformation had an ECASS II haemorrhagic infarction grade 1. Sample flat-panel CT scans and corresponding CT or MRI scans are shown in figure 2.
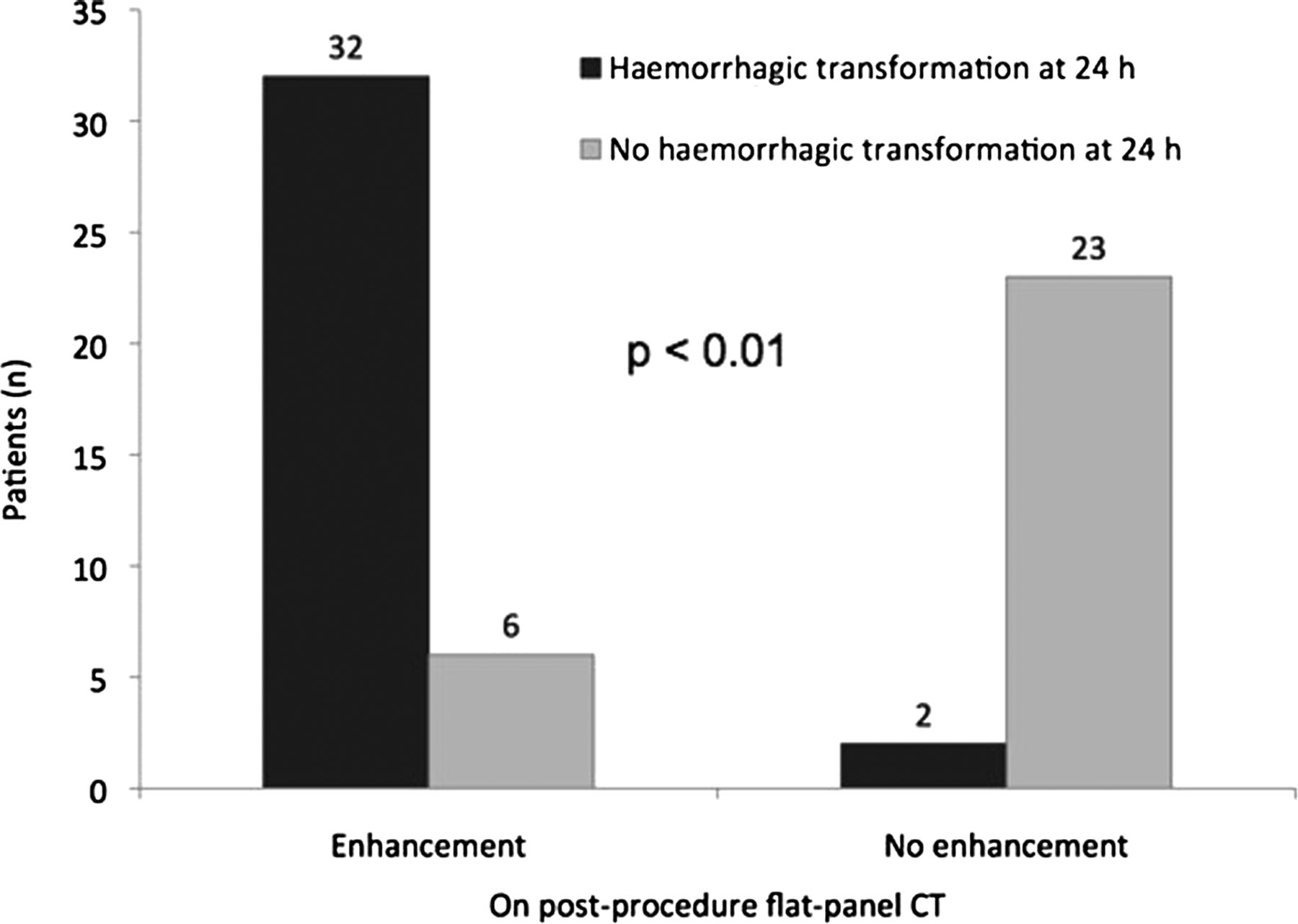
Haemorrhagic transformation on 24 h CT or MRI by presence or absence of brain parenchymal hyperdensity at post-procedure flat-panel CT.
{kind=link}
{kind=link}
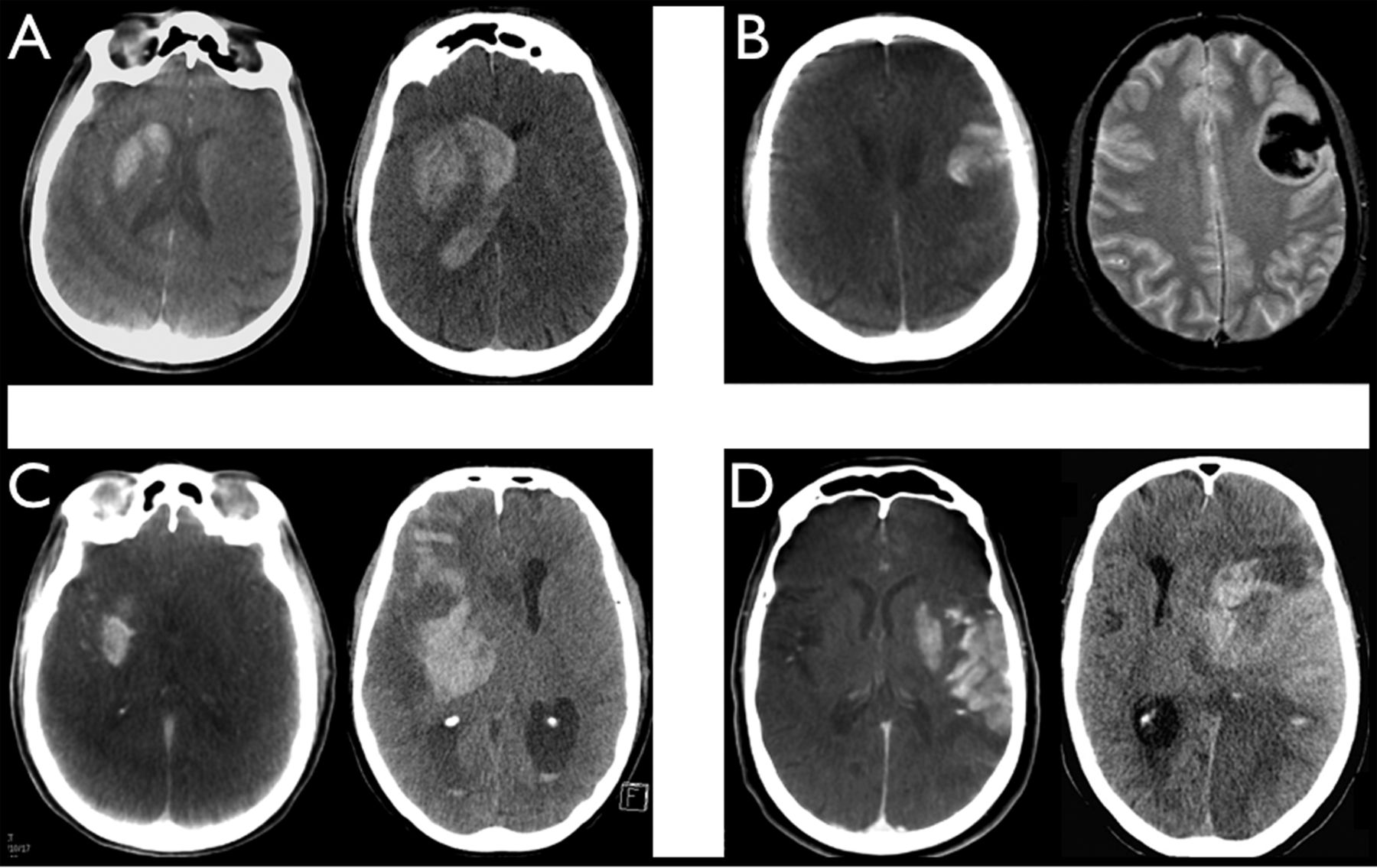
Images of post-thrombectomy flat-panel CT (left) and 24 h non-enhanced conventional CT or T2* MRI (right) for four patients. (A) Patient 1: post-thrombectomy flat-panel CT shows parenchymal hyperdensity in the head of the right caudal nucleus and in the lenticular nucleus; 24 h conventional CT depicts parenchymal haemorrhage type 1 (PH-1) haemorrhagic transformation in the head of the right caudal nucleus and the lenticular nucleus, and intraventricular haemorrhage. (B) Patient 2: post-thrombectomy flat-panel CT shows parenchymal cortico-subcortical hyperdensity in the left frontal lobe; 24 h T2* MRI depicts PH-1 haemorrhagic transformation in the left frontal lobe. (C) Patient 3: post-thrombectomy flat-panel CT shows parenchymal hyperdensity in the right lenticular nucleus; 24 h conventional CT depicts PH-2 haemorrhagic transformation in deep and superficial right middle cerebral artery (MCA) territory. (D) Patient 4: post-thrombectomy flat-panel CT shows parenchymal hyperdensity in the left lenticular nucleus and in the superficial left MCA territory; 24 h conventional CT depicts PH-2 haemorrhagic transformation in deep and superficial left MCA territory.
Sensitivity, specificity, and positive and negative predictive values of the flat-panel CT performed just after the completion of mechanical thrombectomy for the prediction of 24 h haemorrhagic transformation and PH-2 transformation are expressed in table 2.
Sensitivity, specificity, and positive and negative predictive values of post-thrombectomy brain parenchymal hyperdensity on flat-panel CT for prediction of haemorrhagic transformation
The inter-observer κ score for the flat-panel CT images was 0.867 (95% CI 0.742 to 0.993), showing good agreement between the neuroradiologist and the neuroradiology fellow. There was also good agreement between these investigators and the intensivist (κ score 0.735; 95% CI 0.563 to 0.906).
Discussion
Various studies have shown that the presence of contrast enhancement on conventional CT scans after intra-arterial thrombolysis, reperfusion therapy or revascularisation therapy for stroke increases the risk of detectable haemorrhage,3–5 ,13 ,14. There is also evidence to suggest that patients who have higher Hounsfield units are more likely to have significant haemorrhage13 ,14.
However, to the best of our knowledge, no previous studies have evaluated the performance of flat-panel CT for the detection of risk factors for the prediction of haemorrhagic complications after mechanical thrombectomy for patients with AIS.
We evaluated post-recanalisation flat-panel CT and its ability to predict haemorrhagic transformation in AIS. To have an easy and rapid interpretation, we focused on the presence or absence of brain parenchymal hyperdensity as a risk factor for haemorrhagic transformation. This simple analysis allows non-radiologist physicians to interpret flat-panel CT by their own and adapt adjuvant treatments in the setting of AIS.
The analysis of post-procedure flat-panel CT performed by two neuroradiologists found that 60.3% of patients had parenchymal hyperdense lesions, which is in line with the results from other studies (33–60%)4 ,13–15. The inter-observer κ score (0.867; 95% CI 0.742 to 0.993) showed good consensual agreement between observers, and the sensitivity was similar to that reported in the literature with conventional CT4 ,13–15. These factors indicate that flat-panel CT is a reliable and reproducible imaging technique to detect parenchymal hyperdensities after mechanical thrombectomy in patients with AIS, which can be assimilated to BBB rupture.
There was no difference between the two groups (presence or absence of hyperdense lesions on the post-procedural flat-panel CT) according to previous thrombolysis administration, previous CT with contrast medium loading dose, initial NIHSS score, site of the arterial occlusion, time to recanalisation, recanalisation procedure duration, number of passages of the stent-retriever device or TICI recanalisation grade.
Moreover, hyperdense lesions on post-procedure flat-panel CT predicted the haemorrhagic transformation risk on 24 h follow-up imaging, with a high positive predictive value (84.2%) and a high negative predictive value (92.0%). In our series, when PH-2 haemorrhagic transformation was considered (symptomatic haemorrhage affecting the mRS at 3 months), sensitivity and negative predictive values were 100%14 ,16–18. These results are in accordance with previous studies using conventional CT scans, which reported haemorrhagic transformations in 58% of patients (19% symptomatic) when hyperdense lesions were detected on post-procedure CT scans4 ,13 ,14 ,19.
This study presents the limitations of any small, single-centre, retrospective study. Also, we focused on several factors which constitute predictive factors for haemorrhage transformation but we did not take into account other critical factors, such as blood pressure, medical history and stroke aetiology, in contrast to previous studies17 ,20 ,21.
Unlike most studies that have evaluated post-revascularisation conventional CT scans to predict haemorrhagic risk, this study used a simple and rapid protocol to interpret post-procedure flat-panel CT and to detect patients at high risk of haemorrhagic transformation. In contrast to many previous studies3 ,13 ,14, there is no distinction between the different types of BBB ruptures, even if different entities can be mixed under these criteria. Rather, attention is focused on the presence or absence of any hyperdense lesions without taking into account Hounsfield unit measurement, contrast enhancement location, volume estimation of the lesion or any differentiation between contrast extravasation and contrast enhancement. Pooling all the hyperdense lesions diagnosed on post-procedural flat-panel CT implies dealing with different entities such as BBB breakdown due to the ischaemia/reperfusion phenomenon and also iatrogenic complications, especially after stent retriever usage, due to arterial perforation leading to intraparenchymal haematoma of subarachnoid haemorrhage. Even if flat-panel CT has previously been evaluated for the diagnosis of complications such as arterial perforation during neuroendovascular procedures22 ,23, it unfortunately presents limits in term of spatial resolution and it is not possible to strictly discriminate hyperdensity due to BBB rupture or to iatrogenic complications, especially in the acute phase of AIS because these two entities often overlap. Nevertheless in previous studies, distinction between BBB rupture and contrast extravasation did not imply different management attitudes13.
However, whatever the origin of intracranial hyperdensity after mechanical revascularisation, this study shows that detection of intracranial hyperdensity is associated with a higher risk of haemorrhage and poor clinical outcome. Physicians who take care of patients in the acute phase have to know when patients are at high risk of haemorrhagic transformation so that adjuvant treatments can be adapted. Acute stroke management involves a multidisciplinary team, including neurologists, intensivists and neuroradiologists. Our easy-reading protocol permits interpretation by non-radiologist physicians as shown by the high inter-observer κ score between the neuroradiologists and the intensivist (0.735). Without the need for a dedicated workstation allowing Hounsfield unit measurement, non-radiologist physicians are able to draw conclusions for acute patient management. The simple analysis protocol of this study with no subanalysis facilitates interpretation by non-radiologists with no dedicated analysis workstation, allowing them to quickly identify patients at high risk of haemorrhagic transformation and to adapt their treatment (eg, blood pressure control, antiplatelet therapy).
The high negative predictive value of flat-panel CT may preclude the need for 24 h follow-up CT or MRI. Furthermore, flat-panel CT can be performed in the angiographic suite where mechanical thrombectomy is performed. This avoids the need to transfer patients to the conventional CT suite, thereby saving time, improving safety (especially if the patient is intubated, if the procedure is conducted under general anaesthesia) and reducing costs.
Moreover, detection of hyperdense parenchymal lesions on post-procedure flat-panel CT seems to be an important marker for higher risk of death (OR=2.08; 95% CI 0.63 to 6.82; p=0.23) and lower risk of good clinical outcome (OR=0.46; 95% CI 0.16 to 1.28; p=0.14).
Further studies could evaluate early or delayed antiplatelet therapy based on the presence or absence of brain parenchymal enhancement on flat-panel CT at the end of the revascularisation procedure. Likewise, the impact of more aggressive blood pressure control in the prevention of haemorrhagic transformation could be tested in cases of brain parenchymal enhancement.
Conclusion
Flat-panel CT, analysed using an easy-reading protocol (presence or absence of hyperdense lesions), appears to be a good tool for the prediction of risk of 24 h haemorrhagic transformation in the acute phase of recanalisation for patients with AIS.
References
Footnotes
-
Contributors AR, SP and MP: contributed to conception and design of the study; SP, RB, BB and MP: acquired the data; AR, SP and NE: analysed and interpreted the data; AR, SP and MP: drafted the article; RB and MP: critically revised the article for important intellectual content; MP: finally approved the article to be published.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Rothschild Institutional Ethical Committee.
-
Provenance and peer review Not commissioned; internally peer reviewed.