Article Text

Abstract
A middle aged patient presented with acute ischemic stroke due to basilar artery occlusion. The patient clinically deteriorated despite intravenous thrombolysis and was referred for mechanical thrombectomy. The right vertebral artery was occluded and could not be accessed despite attempting various shaped catheters, even when a radial artery access was used. The left vertebral artery ended in the posterior inferior cerebellar artery. Eventually, ultrasound guided V3 segment vertebral artery direct puncture was successfully done and the procedure was completed. No access related complications were encountered. Direct cervical arterial puncture can be safely used by experienced operators as a last resort in acute stroke cases with difficult access.
- Angiography
- Stroke
- Ultrasound
Statistics from Altmetric.com
Background
Severe tortuosity can cause significant delays in reaching the target occlusion site for mechanical thrombectomy in the acute ischemic stroke setting. We present a case where access to the posterior circulation was successfully obtained through direct puncture of the cervical vertebral artery (VA).
Case presentation
A middle aged ex-smoker with no known medical comorbidities presented after a witnessed collapse at 06:30 h which was preceded by a sense of dizziness. Initial blood pressure was 170/95 mm Hg. Initial examination demonstrated an altered level of consciousness, gaze deviation to the right, a right homonymous hemianopia, right hemiplegia, and severe anarthria. The initial National Institutes of Health Stroke Scale (NIHSS) score was 25.
Investigations
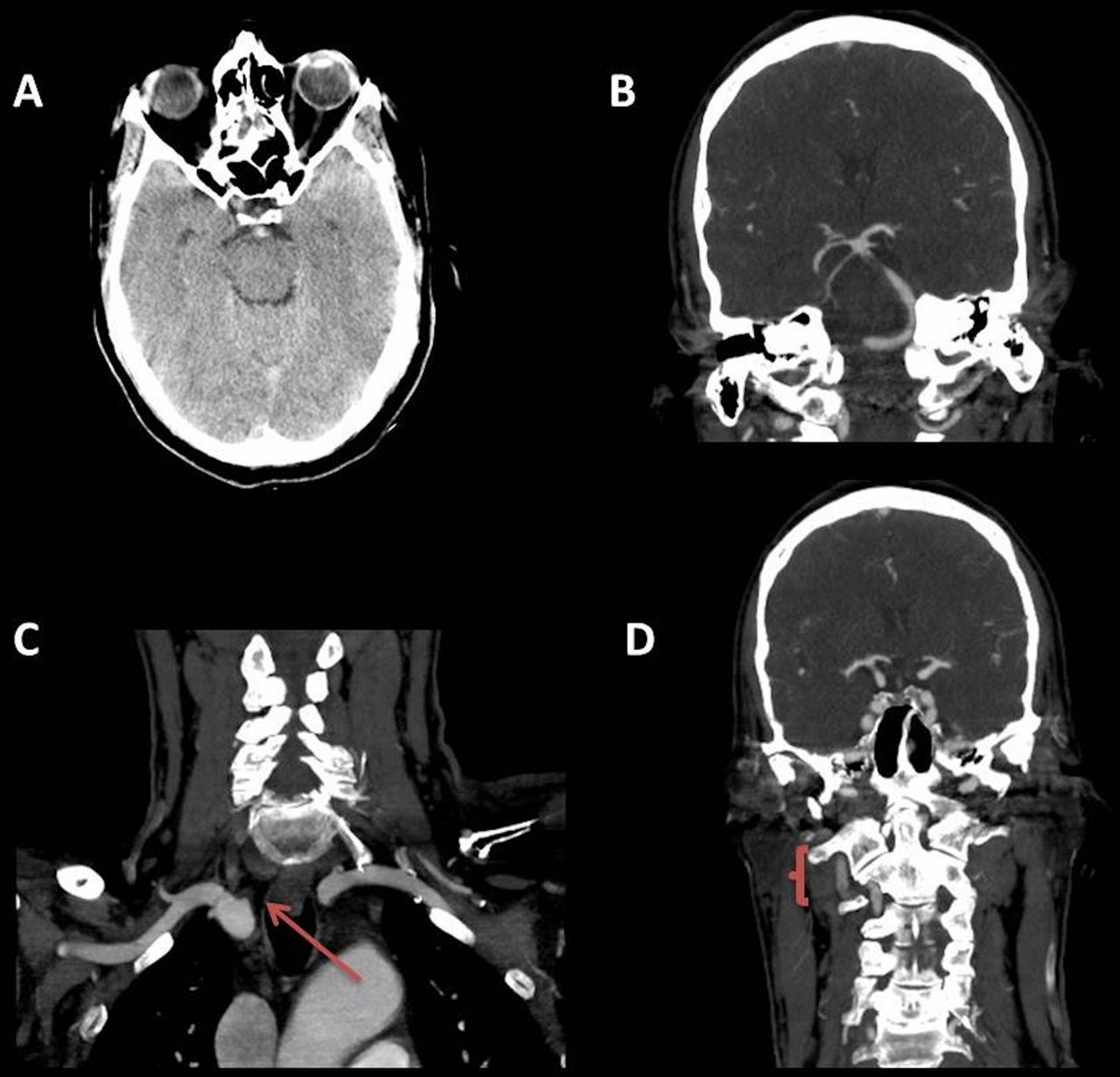
CT head and CT angiography (CTA) from the aortic arch to the vertex at 08:00 h demonstrated early ischemic change in the left posterior cerebral artery (PCA) territory (figure 1A) with an obvious basilar hyperdense sign and a non-occlusive thrombus (figures 1A, 1B) within the intracranial portion of the right VA extending into the proximal basilar artery. Additionally, the right VA was occluded distal to its origin (figure 1C). The left VA was patent but non-dominant and ended in the posterior inferior cerebellar artery. The left P2 segment of the PCA and superior cerebellar artery were also occluded (figure 1B). Patchy opacification of the right V3 segment (figure 1D) and basilar artery was noted secondary to collateral flow from the thyrocervical trunk and occipital artery.

(A) CT scan of the head demonstrating a hyperdense basilar artery. (B) Coronal view CT angiography (CTA) showing a non-occlusive thrombus in the distal basilar artery with occlusion of the left superior cerebellar artery and posterior cerebral artery. (C) Coronal view of the arch CTA showing occlusion at the origin of the right vertebral artery (VA) (arrow). (D) Coronal view CTA of the V3 segment of the right VA where the puncture was performed (brace).
Treatment
Intravenous tissue plasminogen activator was administered at 08:04 h. The patient further deteriorated clinically with bifacial weakness, quadraparesis, and intermittent decerebrate posturing. NIHSS score was 31. The patient was rapidly intubated and transported to the interventional suite for mechanical thrombectomy.
A 6 French sheath was placed in the right common femoral artery for access. Multiple attempts were made to access the right VA using various shaped diagnostic catheters but were unsuccessful due to the extreme tortuosity in the subclavian artery leading to the VA origin and occlusion of the right VA origin. A right transradial approach to gain access to the right VA in a retrograde manner from the subclavian artery was unsuccessful as we could not advance the wire beyond the occluded origin of the VA. Obtaining direct access to the VA via surgical cutdown versus direct puncture was considered. Owing to the acute nature of the basilar occlusion, the ongoing infusion of intravenous tissue plasminogen activator, and the time elapsed, direct V3 puncture was favored. No sizable anastomotic branches from the occipital or cervical arteries to the VA could be visualized. Therefore, this access route was not considered.
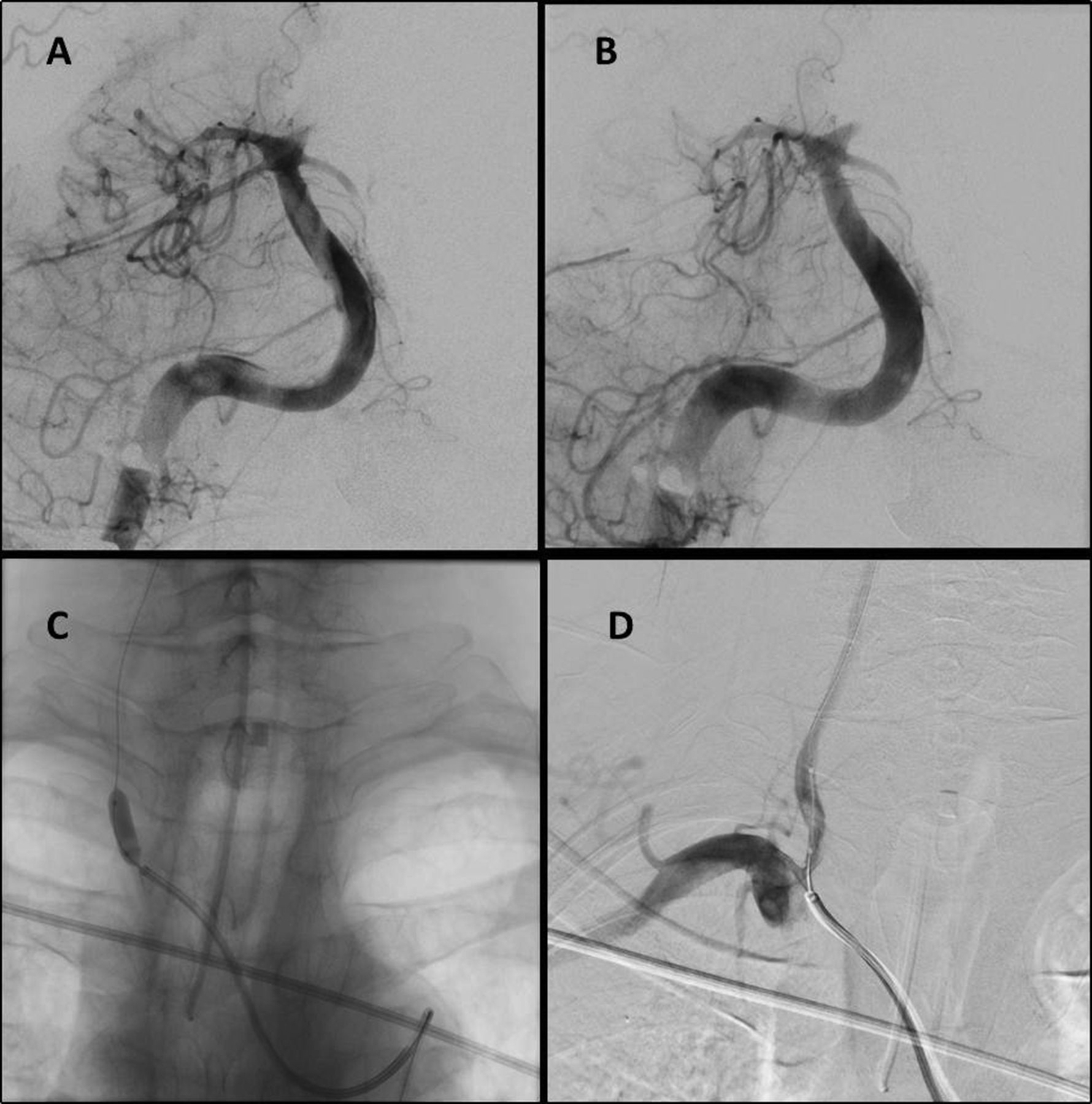
The appropriate superficial landmarking was decided based on CTA. For percutaneous ultrasound guided puncture, the right vertebral access site at the V3 segment was determined to be inferior to the tip of the mastoid process (figure 3). A linear high frequency probe was used in the transverse orientation to the vessel. A regular micropuncture access needle was successfully placed into the V3 segment of the VA and a micropuncture sheath was inserted. Through the sheath, an exchange length stiff wire (Glidewire, Terumo, Somerset, New Jersey, USA) was advanced caudally and maneuvered through the occluded origin of the right VA and subsequently into the aortic arch. From there, the wire was engaged using a vascular snare device (16 mm GooseNeck Snare; Covidien, Irvine, California, USA) and pulled out through the right femoral sheath. Subsequently, a 6 F guide catheter (Neuron 070; Penumbra Inc, Alameda, California, USA) was advanced over the exchange length wire beyond the occluded VA origin into the distal V2 segment (figure 2). TIMI grade 3 recanalization of the basilar artery was achieved using one deployment of a 6 mm×30 mm Solitaire device (Covidien) at 11:45 h. Revascularization of the persistently occluded superior cerebellar arteries and the left PCA was not attempted mechanically. However, 2 mg of intra-arterial tissue plasminogen activator was administered locally. Finally, angioplasty without stent placement was performed at the origin of the right VA using a non-compliant balloon (5 mm Sterling; Boston Scientific, Natick, Massachusetts, USA), to promote forward flow (figure 4C, D).
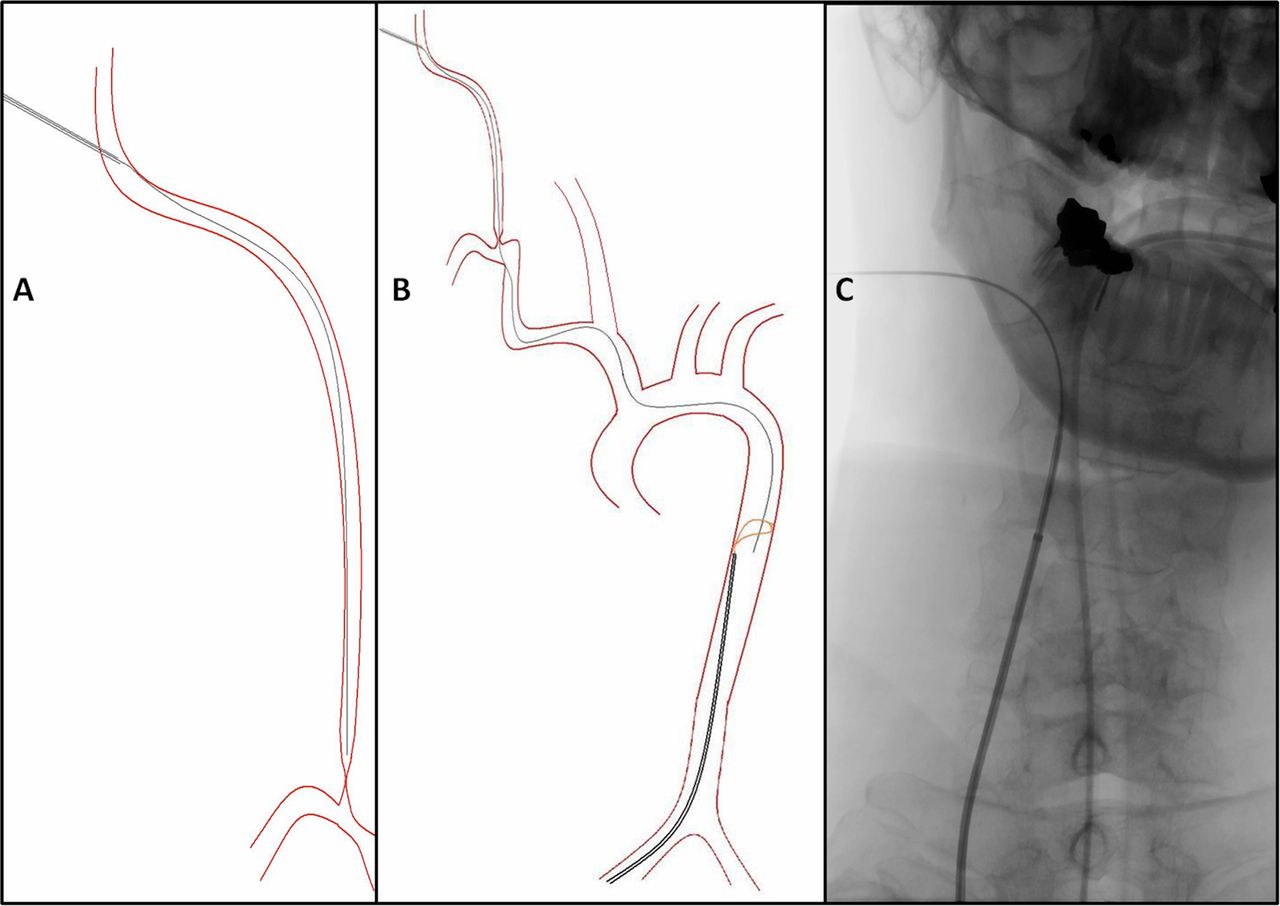
Direct V3 vertebral artery (VA) puncture. (A) Ultrasound guided puncture was performed and an exchange length wire was advanced caudally across the occluded proximal right VA. (B) The wire was snared in the descending aorta and pulled through the femoral sheath. (C) The guide catheter was advanced over the wire into the distal V2 segment.
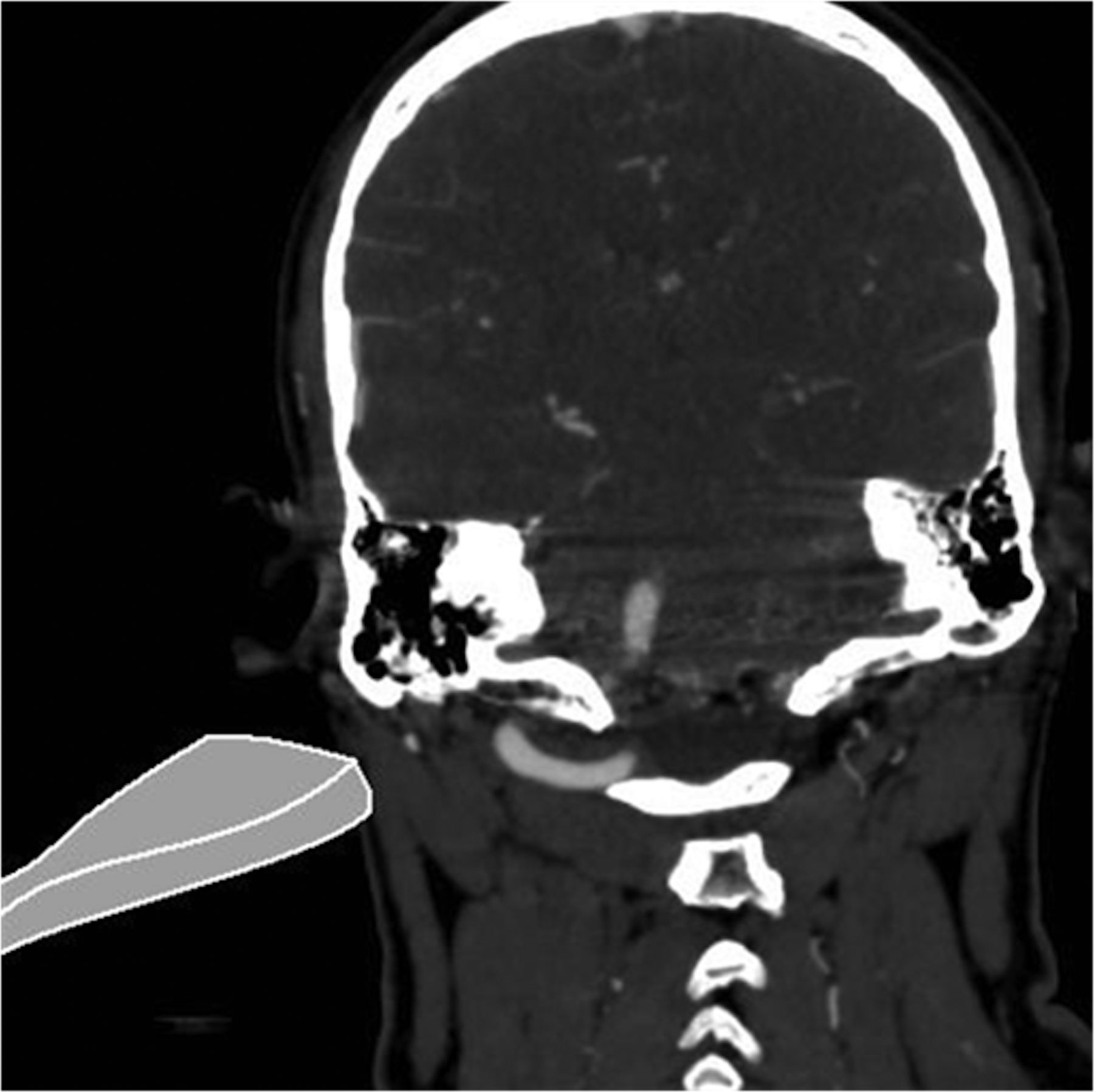
Positioning of the ultrasound probe for vertebral artery insonation.
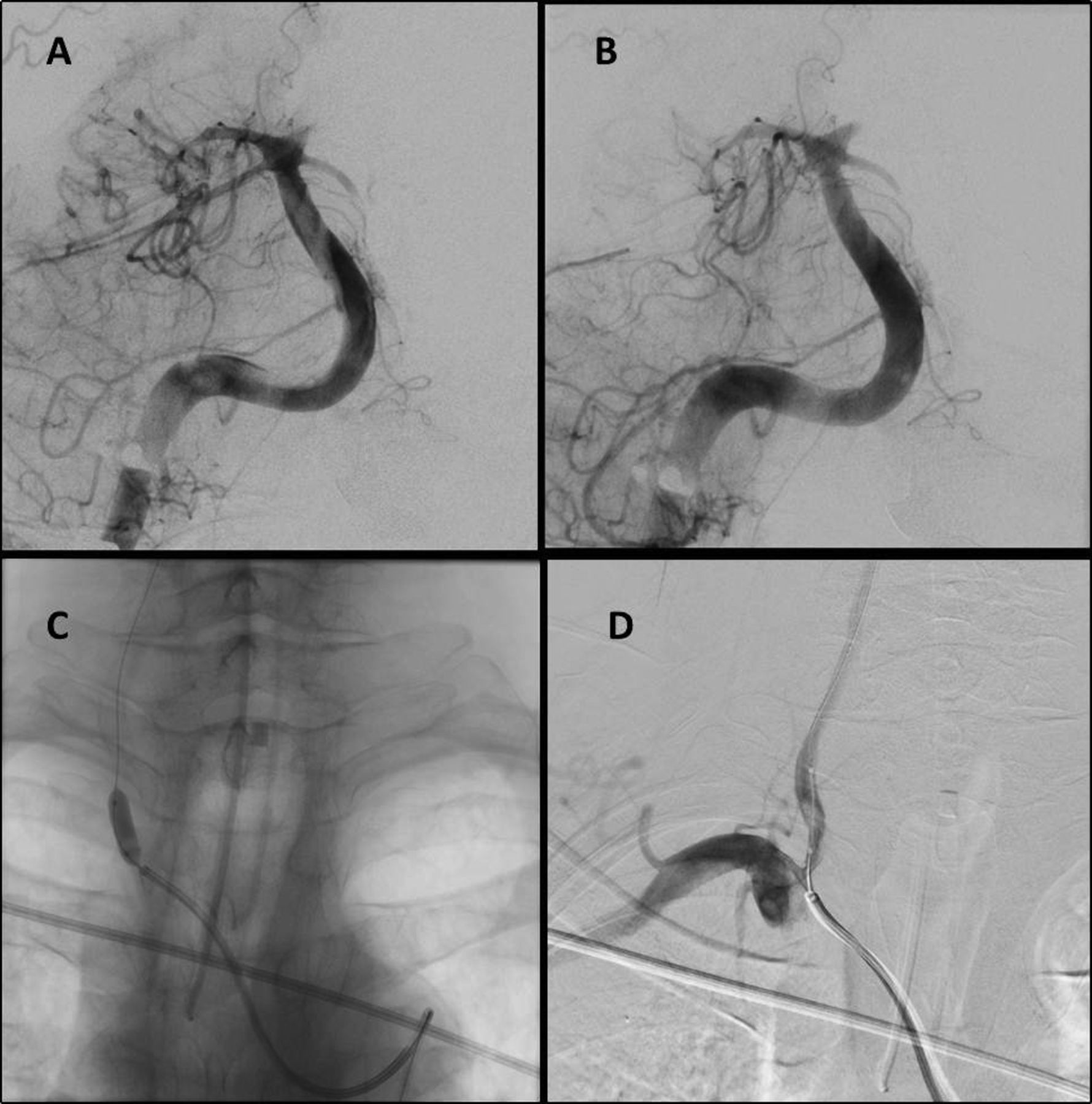
Catheter angiogram images showing the thrombus in the basilar artery before (A) and after (B) stent retrieval use. The left superior cerebellar artery and posterior cerebral artery remained occluded. Balloon angioplasty was performed at the origin of the right vertebral artery (C) with residual moderate stenosis (D).
Outcome and follow-up
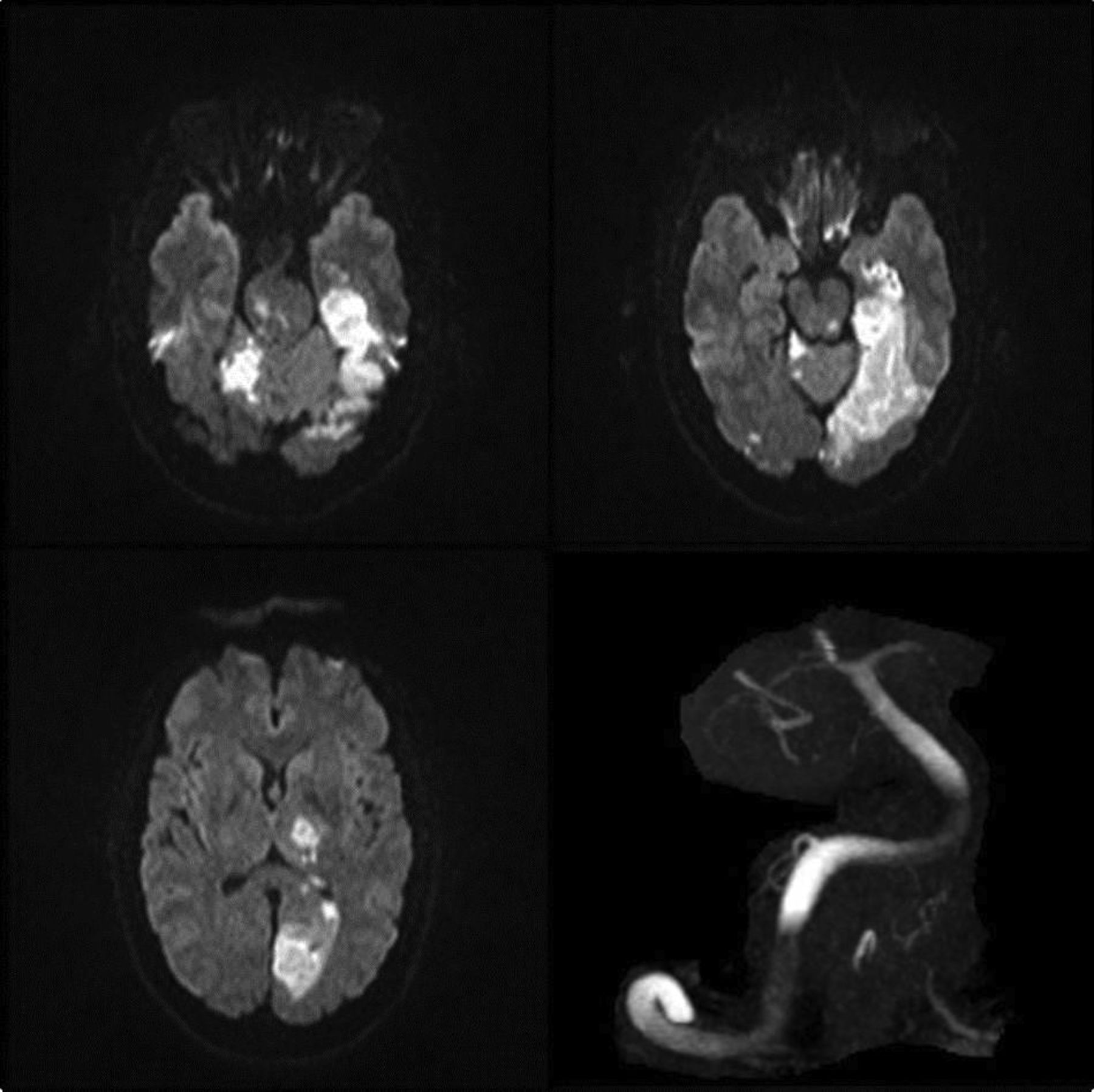
The patient was successfully extubated that evening. Follow-up MRI showed evolved infarcts in the left PCA territory with scattered infarcts involving the right PCA, the cerebellar hemispheres, and pons (figure 5). MRA revealed poor signal through the vertebrobasilar system (figure 5) and the patient was loaded with acetylsalicylic acid 650 mg rectally and clopidogrel 300 mg by the nasogastric route. The patient continued to improve clinically, with day14 examination demonstrating partial right homonymous hemianopia, right arm pronator drift, right facial droop, right arm severe dysmetria, and severe dysarthria (NIHSS=7). Unfortunately, on day 17 the patient had an abrupt decease in level of consciousness. Urgent imaging revealed bilateral pontine and left occipital hemorrhages into regions of previous infarcts. The patient was palliated in accordance with the family wishes and passed away shortly after.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
MRI of the brain post procedure, showing acute ischemic changes in the right cerebellar hemisphere, left thalamus, and left occipital lobe. Time of flight MR angiography shows poor signal in the vertebrobasilar system.
Discussion
Vertebral angiography was pioneered by Moniz and Alves in 1936, and initially performed by exposure and direct injection of subclavian or vertebral arteries.1 A percutaneous lateral atlanto-occipital approach was refined by Maslowski in 1950.2 Currently, if femoral access is difficult, the transradial approach can be done with high rates of success and safety.3 ,4 In small series of patients where transfemoral or radial approaches were difficult, direct percutaneous puncture and surgical cutdown techniques appeared effective and safe, with >90% success rate of canulating the target vessel.5 ,6 Common complications of direct arterial puncture included cervical hematomas, transient vasospasm, puncture related vasospasm with secondary thrombus formation, pseudoaneurysms at the puncture sites, and injury to the caudal loop of the posterior inferior cerebellar artery.5 ,7 ,8 However, complications are rare and can be minimized by using micropuncture access and performing a single wall puncture technique.
Direct punctures for posterior circulation access have been reported in the context of aneurysm coiling or arteriovenous malformation embolization. In acute stroke cases where intra-arterial therapy is deemed appropriate and routine vascular access has failed, direct percutaneous puncture or surgical cutdown exposure of the VA should be entertained. Ultrasound guided direct percutaneous puncture of the V2 or V3 segment is more expeditious than surgical cutdown and can be performed in conventional angiography suites, obviating the involvement of a neurosurgeon and need for a surgical suite. Because basilar artery thrombosis is associated with such high morbidity and mortality, early consideration of this approach should be undertaken when standard routes of access are unavailable.
Key messages
-
Vascular access can pose a significant challenge preventing timely recanalization in acute stroke mechanical treatment.
-
Direct carotid or vertebral arterial puncture has been reported to be a safe option when used for elective endovascular brain interventions.
-
Direct cervical vertebral artery puncture might be considered as a last resort by experienced operators to access the intracranial vasculature for mechanical treatment of ischemic stroke.
Footnotes
-
Republished with permission from BMJ Case Reports published 27 March 2013; doi:10.1136/bcr-2012-010601
-
Contributors Conceptual design: JAD, MAA and ME. Drafting: JAD and MAA. Figure preparation: MAA and ME. Critical review: MDH, MG and ME.
-
Competing interests None.
-
Ethics approval The patient was included in a prospectively maintained database for endovascular acute ischemic stroke patients. This database received approval from the University of Calgary Conjoint Health Research Ethics Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.