Article Text

Abstract
Background Successful neuroendovascular treatments rely on microcatheter stability from guide catheter support. We present our experience using a new large-bore 0.058 inch or 0.072 inch inner diameter (ID) hyperflexible access catheter placed deep within the intracranial circulation during the neurointervention.
Methods We retrospectively reviewed all neurointerventions performed by the senior author during an 18-month period to identify patients in whom the Navien intracranial catheter was placed in an ultra-distal position, defined as beyond the clinoidal internal carotid artery (ICA) or V3 segment of the vertebral artery. Procedural data collected included parent artery tortuosity, technique for Navien advancement, intraprocedural Navien position and periprocedural complications.
Results The Navien, either 6 F 0.072 inch ID or 5 F 0.058 inch ID, provided ultra-distal large-bore access in the following 11 intracranial interventions: anterior circulation aneurysm treatment with Pipeline embolization device (PED) (n=3); posterior circulation aneurysm single-stage stent coiling (n=5); liquid embolization of arteriovenous malformations (n=2); PED coiling of posterior circulation aneurysm (n=1). The Navien was tracked into position over a Marksman microcatheter in 10/11 cases and a Headway 27 microcatheter in one case. Intraprocedural Navien positions were as follows: supraclinoid ICA (n=2); mid M1 (n=1); V3–V4 junction (n=2) (both using 6 F Navien); distal V4 (n=3); proximal basilar (n=1); proximal-mid basilar (n=1); mid basilar (n=1). No significant catheter-related complications occurred.
Conclusions The Navien is the newest hyperflexible access catheter that is highly trackable into ultra-distal intracranial positions. It maneuvers atraumatically, providing improved distal intracranial support for a variety of complex cerebrovascular interventions and preserves necessary ID for quality intraprocedural roadmaps and angiography.
- Aneurysm
- Arteriovenous Malformation
- Catheter
- Coil
- Flow Diverter
Statistics from Altmetric.com
Introduction
Microcatheter stability provided by the guide catheter is fundamental to successful and safe endovascular interventions. The rigidity of traditional guide catheters restricts their positioning to extracranial locations. New generations of hybrid catheters such as the Neuron (Penumbra, Alameda, California, USA) and Outreach Distal Access Catheter (DAC; Stryker, Kalamazoo, Michigan, USA) have flexible soft tips allowing distal intracranial access. Experiences with these distal intracranial catheters (DICs) have demonstrated their trackability into intracranial locations.1–8
The Navien distal intracranial support catheter (Covidien Vascular Therapies, Mansfield, Massachusetts, USA) is the latest innovation of hybrid DICs on the market designed in the new era of flow diversion. These types of catheters have a sufficiently large inner diameter (ID) to accommodate the 0.027 inch microcatheters required for deployment of flow diverters such as the Pipeline embolization device (PED; Covidien Vascular Therapies). The larger inner lumen also provides additional room for improved flush and injections. The Navien catheter is available in 5 F or 6 F outer diameter (OD), 0.058 inch or 0.072 inch ID, respectively. The large bore and hyperflexible nature of the Navien catheters render them highly desirable tools for a variety of complex neuroembolizations.
We present our experience using these new hyperflexible Navien distal intracranial support catheters to achieve large-bore (0.058 inch or 0.072 inch ID) access deep within the intracranial circulation during neurointervention.
Methods
Patient selection
We retrospectively reviewed all neurointerventions performed by the senior author from September 2011 to December 2012, identifying all patients in whom either a 6 F 0.072 inch ID (0.084 inch OD, 105 cm length) or 5 F 0.058 inch ID (0.070 inch OD, 115 cm length) Navien catheter was placed in an ultra-distal position, beyond the clinoidal internal carotid artery (ICA) or beyond the V3 segment of the vertebral artery.
Data collection
Data were collected with respect to patient demographics and pathology treated. Procedural data analyzed included equipment used, parent artery tortuosity, technique for DIC advancement, final intraprocedural catheter position, periprocedural complications related to the catheter position and immediate angiographic results. Data are presented as counts.
Results
Procedural characteristics
In 11 intracranial interventions, either a 6 F 0.072 inch ID or 5 F 0.058 inch ID Navien was positioned beyond the clinoidal ICA or V3 segment. Details of these procedures are presented in table 1. The mean patient age was 52.8 years (range 41–67). There were eight women and three men in this series. Figures 1 and 2 demonstrate the parent vessel tortuosity for each of these patients. The Navien was tracked into position using a 0.027 inch Marksman microcatheter (Covidien Vascular Therapies) in all but one case (patient 10) in whom the 0.027 inch Headway microcatheter (MicroVention, Tustin, California, USA) was used for its smaller proximal OD (compared with the Marksman) in jailing of the coiling microcatheter.
Summary of neurointerventions using the Navien distal intracranial catheter (6 F 0.072 inch ID or 5 F 0.058 inch ID) in an ultra-distal location
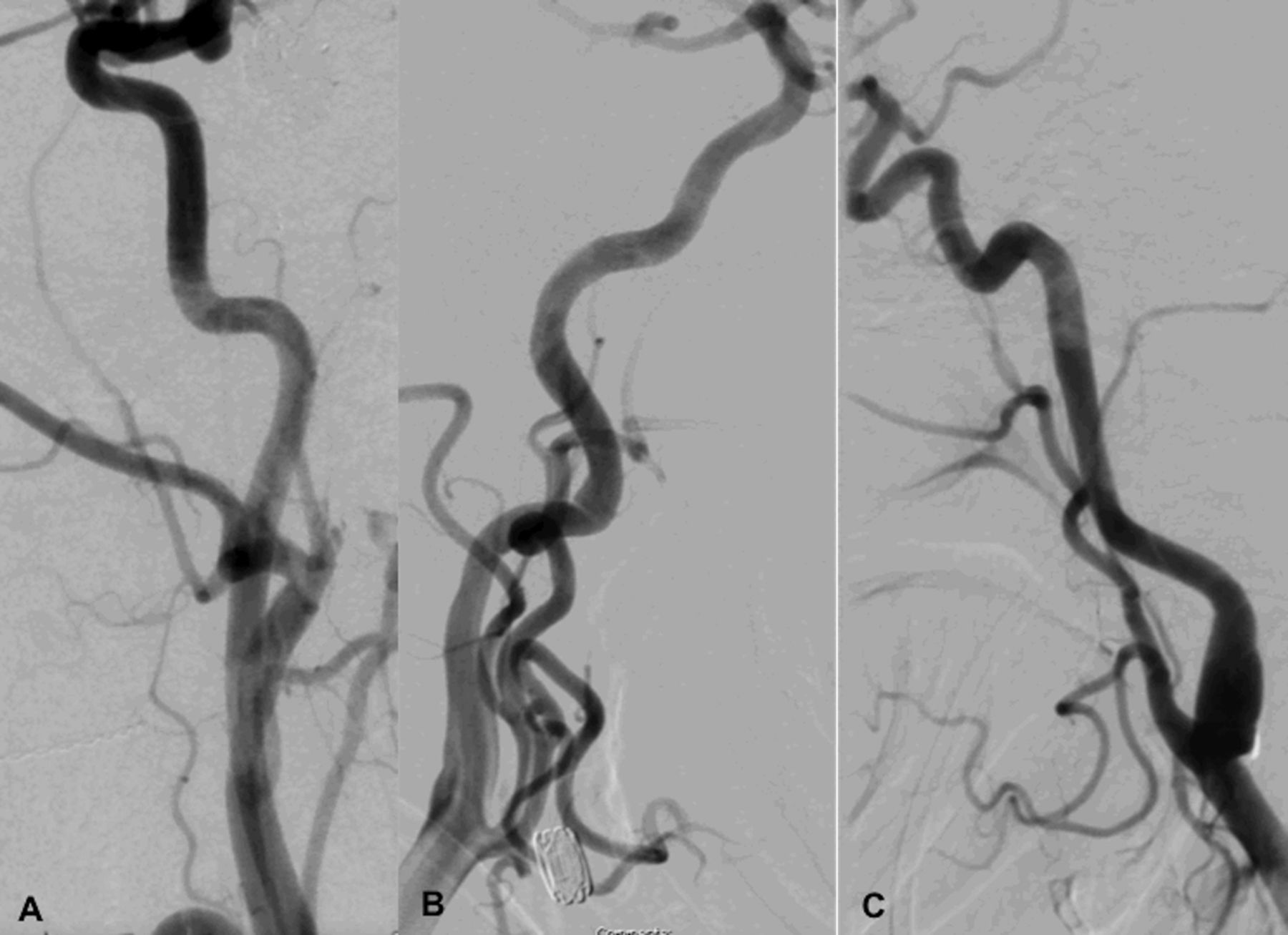
Parent internal carotid artery (ICA) from each of the anterior circulation interventions. (A) Right common carotid digital subtraction angiography (DSA) of patient 1 demonstrating tortuosity of the petrocavernous ICA. (B) Left common carotid DSA of patient 2 demonstrating tortuosity of the cervicopetrous ICA. (C) Left common carotid DSA of patient 3 demonstrating tortuosity throughout the length of the ICA.

Parent vertebral artery accessed from each of the posterior circulation interventions. (A) Left vertebral digital subtraction angiography (DSA) of patient 4. (B) Left vertebral DSA of patient 5. (C) Left vertebral unsubtracted angiography of patient 6. (D) Left vertebral DSA of patient 7. (E) Left vertebral DSA of patient 8. (F) Left vertebral DSA of patient 9. (G) Left vertebral DSA of patient 10. (H) Left vertebral intraprocedure roadmap of patient 11.
Of the 11 interventions, three were located along the anterior circulation and were all PED treatments of wide-necked aneurysms. In one of these cases, two aneurysms were treated. The aneurysms were in the following locations: posterior communicating artery, ICA termination, A2–A3 junction and M2. For these three anterior circulation PED embolizations, the 5 F 0.058 inch ID Navien was used in conjunction with a 90 cm 6 F Flexor Shuttle sheath (Cook Medical, Bloomington, Indiana, USA) positioned in the proximal cervical ICA providing a triaxial support system. PED embolization procedures were performed as previously described.9 The final intraprocedural Navien position was in the middle of the M1 segment for one case and the distal supraclinoid ICA for the other two.
The remaining eight interventions involved the posterior circulation for the following treatments: single-stage stent coiling of superior cerebellar artery (SCA) aneurysm (n=2), single-stage stent coiling of basilar apex aneurysm (n=1), single-stage Y stent coiling of basilar apex aneurysm (n=2), liquid embolization of arteriovenous malformations (AVM; n=2) and coil-assisted PED treatment of posterior inferior cerebellar artery (PICA) aneurysm (n=1). In these cases the Navien served as the primary guide catheter within either a 5 F or 6 F long sheath (≥55 cm) positioned in the subclavian artery proximal to the vertebral artery origin. Typically, the proximal vertebral artery was first selected with a 5 F JB-1 glide catheter (Terumo Medical Corporation, Somerset, New Jersey, USA). The JB-1 catheter was then exchanged for the Navien. Thereafter, the Navien was tracked over a 0.027 inch microcatheter into its final ultra-distal location. Of the eight posterior circulation cases, the 5 F Navien was used in six cases with the following final intraprocedural positions: distal V4 (n=3), proximal basilar (n=1), proximal to mid basilar (n=1) and mid basilar (n=1). The 6 F 0.072 inch ID Navien was used in the other two posterior circulation interventions. For one of these cases the 6 F Navien was positioned in the V3–V4 junction to allow jailing of the coiling microcatheter during PED coiling of a PICA aneurysm. For the other embolization, the 6 F Navien was positioned in the V3–V4 junction for added stability in single-stage Y-stent coiling (with jailing) of a small wide-necked basilar apex aneurysm.
No complications (eg, dissection) were encountered during positioning. All but one intervention was completed successfully. The one incomplete case was a small choroidal AVM where no definitive large arterial feeders were identified with microcatheter angiography. For this reason, embolization was not possible.
Case examples
Case illustration 1: Improved microcatheter support for microcatheter manipulations in PED deployment
A 56-year-old patient (patient 3) with a remote history of microsurgical clipping of two right middle cerebral artery (MCA) bifurcation aneurysms in the setting of subarachnoid hemorrhage presented with new right facial droop secondary to Bell's palsy. Subsequent evaluation revealed recurrence of the previously clipped aneurysms, a new 20 mm right cavernous ICA aneurysm and a new 6 mm fusiform left M2 segment aneurysm. Considering the large size of the right ICA aneurysm, this was treated first using the PED. Follow-up angiography 6 months after PED treatment of the ICA aneurysm demonstrated expected flow remodeling of the ICA aneurysm with marked decrease in the aneurysm pouch. However, there was interval growth of the fusiform left M2 aneurysm to 8 mm (figure 3A,B). Given the fusiform nature of the left M2 aneurysm and the patient's need for continued dual antiplatelet therapy, a decision was made to treat the enlarging M2 aneurysm with the PED.

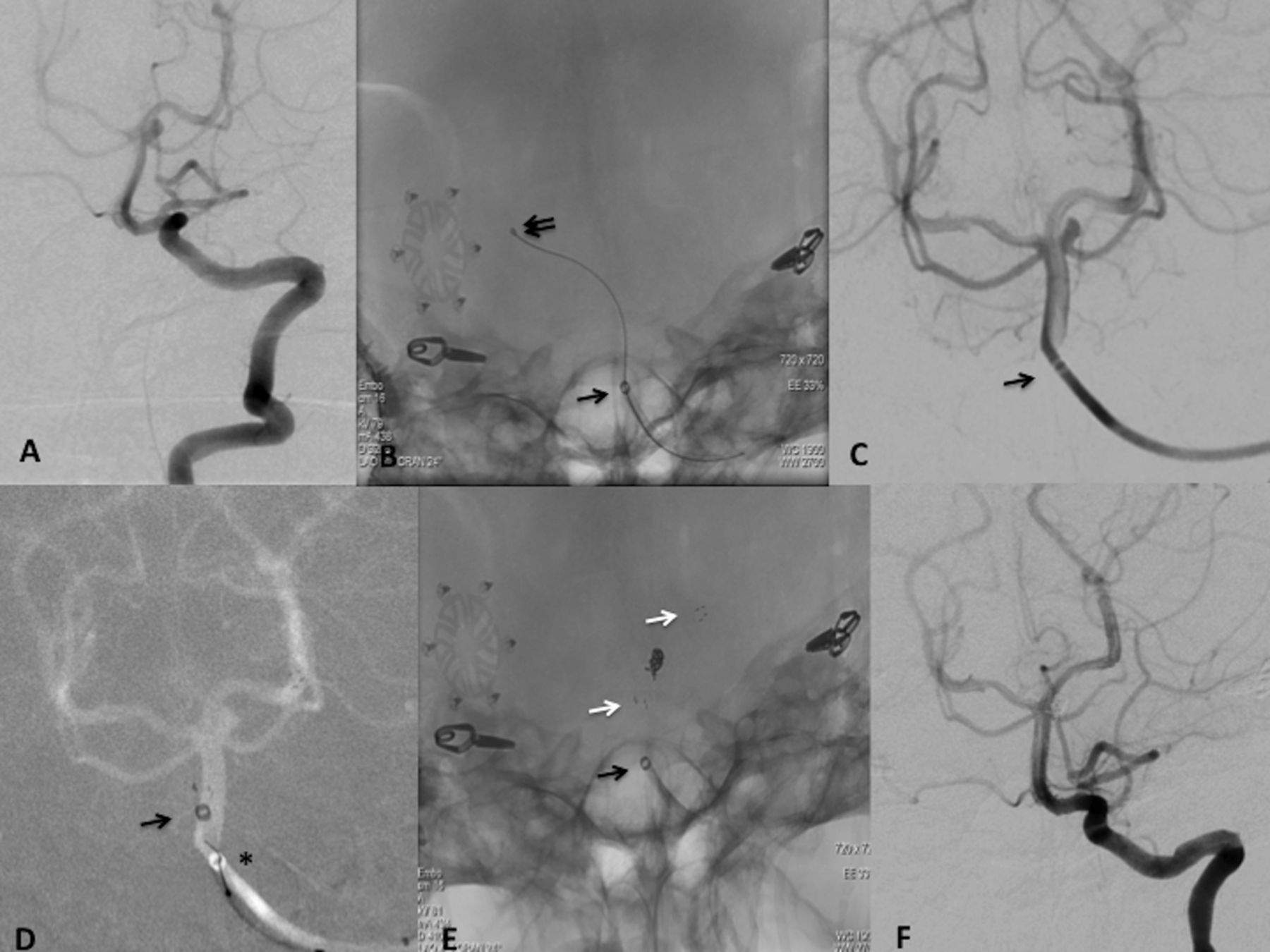
Proximal middle cerebral artery (MCA) Navien support during Pipeline embolization of a 8 mm left M2 segment fusiform aneurysm in a 56-year-old patient with internal carotid artery (ICA) and MCA tortuosity. (A, B) Left common carotid digital subtraction angiography (DSA), anteroposterior and lateral views, demonstrating the fusiform M2 aneurysm. (C) Intraprocedure roadmap (from the 6 F Flexor Shuttle sheath) for tracking the Navien (black arrow indicates Navien tip) over the Marksman (black double arrows indicate Marksman tip) into the mid M1 position. (D) Pre-Pipeline embolization device (PED) deployment single shot native fluoroscopy image in contralateral oblique view showing the Navien positioned in the mid M1 segment (black arrow indicates Navien tip, black double arrows indicate Marksman tip, white arrow indicates distal end of the constrained PED). (E) Post-PED deployment single shot native fluoroscopy image in contralateral oblique view (black arrow indicates Navien tip, black double arrows indicate Marksman tip, asterisk marks the fully deployed PED). (F) Control DSA injection of the left MCA from the Navien catheter after PED implantation. The Navien catheter (black arrow indicates tip) is seen conforming to the tortuosity of the ICA. (G) Final control DSA injection of the left ICA after withdrawal of the Navien catheter into the cervical ICA. There was no evidence of vasospasm or dissection, representative of the atraumatic maneuverability of the Navien catheter. (H) Dyna CT without contrast after PED implantation.
The PED embolization was performed as previously described.9 A triaxial system through right common femoral artery access was built with a 90 cm 6 F 0.087 inch ID Flexor Shuttle sheath, a 115 cm 5 F 0.058 inch ID Navien catheter and a 150 cm 0.027 inch ID Marksman microcatheter. The Navien's smaller 5 F OD (compared with the 5.2 F DAC and 6 F proximally Neuron) allowed superior intraprocedure roadmaps through the Shuttle sheath (figure 3C). The Navien was tracked smoothly over the Marksman with a Synchro 2 standard 0.014 inch microwire (Stryker) to its final position in the mid left M1 segment (figure 3D). This ultra-distal positioning of the Navien catheter in the M1 allowed one-to-one tactile feedback during the pushing/pulling microcatheter manipulations needed for PED deployment. A 3 mm×18 mm PED was successfully implanted across the aneurysm neck despite multiple vessel turns traversed to reach the target landing zone. No complications occurred during the procedure and final control angiography demonstrated patency of the parent vessels without evidence of vasospasm or dissection (figure 3G).
Case illustration 2: Ease of stent delivery and improved microcatheter stability during aneurysm access through stent tines in stent-assisted aneurysm embolization
A 50-year-old patient (patient 5) with a long-standing history of headaches and cardiopulmonary disease presented with episodic dizziness and non-invasive imaging suggestive of a basilar apex aneurysm. Diagnostic cerebral angiography revealed a 4 mm wide-necked left SCA aneurysm (figure 4A), a 6 mm right MCA bifurcation aneurysm and a 5 mm left MCA bifurcation aneurysm. Considering both MCA aneurysms were irregular and wide-necked, the therapeutic plan was to first microsurgically clip the MCA aneurysms sequentially, then treat the SCA aneurysm 6 weeks after the last craniotomy with single-stage stent-assisted coiling.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Proximal to mid basilar Navien support during single-stage stent coil embolization of a 4 mm left superior cerebellar artery (SCA) aneurysm in a 50-year-old patient with vertebral artery tortuosity. (A) Left vertebral pre-embolization digital subtraction angiography (DSA) demonstrating the wide-necked SCA aneurysm and the tortuosity of the vertebral artery. (B) Single shot native fluoroscopy image in Townes view showing the Navien positioned in the proximal to mid basilar. The Navien (black arrow indicates tip) was tracked into position over a Marksman microcatheter (black double arrows indicate tip) positioned in the right posterior cerebral artery. (C) DSA injection from the Navien catheter (black arrow indicates tip) at its final intraprocedure position. (D) Intraprocedure roadmap image immediately after deployment of the Neuroform EZ stent demonstrating slight migration of the Navien catheter forward as slack was removed during the deployment process (black arrow indicates the new position of the Navien tip and the asterisk marks the prior position of the Navien tip). (E) Post-embolization single shot native fluoroscopy image in Townes view (black arrow indicates Navien tip, white arrows indicate proximal and distal stent markers). (F) Final control DSA injection of the left vertebral artery after withdrawal of the Navien catheter into the proximal vertebral artery. There was no evidence of vasospasm or dissection, representative of the atraumatic maneuverability of the Navien catheter.
One week before embolization the patient was pretreated with oral aspirin 325 mg and clopidogrel 75 mg daily. The procedure was performed under general endotracheal anesthesia. The right common femoral artery was accessed with a 5 F short sheath (Terumo Medical Corporation) and then exchanged for a 6 F 55 cm sheath (Cook Medical) placed in the mid descending aorta. The left subclavian artery was selected with a 5 F JB-1 glide catheter and the sheath was advanced over the JB-1 into the left subclavian artery, proximal to the left vertebral artery origin. The JB-1 and glidewire were removed. A 115 cm 5 F Navien was then coaxially introduced with a 150 cm Marksman microcatheter. Under roadmap guidance, the Marksman was advanced over a Synchro 2 standard 0.014 inch microwire into the distal left vertebral artery, then into the basilar artery and the right posterior cerebral artery (PCA). The Navien catheter was tracked over the Marksman into its final position in the proximal to mid basilar junction (figure 4B,C). The Marksman and microwire were removed.
A 150 cm XT27 microcatheter (Stryker) was advanced through the Navien catheter past the aneurysm into the left PCA. A 3 mm×20 mm Neuroform EZ stent (Stryker) was advanced through the XT27 microcathteter and deployed across the aneurysm neck. Despite tortuosity of the left vertebral artery, the Neuroform EZ stent was easily maneuvered and deployed from the left P1 to the mid basilar artery. Of note, as the stent was deployed and slack removed from the system, the Navien catheter migrated slightly forward (figure 4D). The XT27 microcatheter and stent delivery wire were then removed.
A SL-10 microcatheter (Stryker) was advanced through the Navien catheter over a Synchro 2 standard microwire into the basilar artery and the left SCA aneurysm was accessed through the stent tines without any forward jump of the microwire. Coil embolization proceeded with Target 360 Ultra coils (Stryker), 2 mm×6 cm followed by 1 mm×3 cm (figure 4E). The SL-10 microcatheter was extremely stable during the coiling with little catheter kickback. No complications occurred during the procedure. Final control angiography demonstrated patency of the parent vessels without evidence of vasospasm or dissection (figure 4F).
Discussion
In this report we describe our experience using either the 5 F 0.058 inch ID or the 6 F 0.072 inch ID Navien distal intracranial support catheter in ultra-distal locations for neurointerventions of various complex cerebrovascular pathologies. The Navien provided enhanced microcatheter support in neuroembolizations ranging from traditional single-stage stent-assisted aneurysm coiling and liquid embolization of AVMs to more complex Y-stent-assisted aneurysm coiling with microcatheter jailing and PED procedures. In our experience, the 5 F catheter was positioned as far as the mid M1 segment in the anterior circulation and the mid basilar in the posterior circulation. The 6 F catheter was needed in an ultra-distal location only in the posterior circulation for jailing of the coiling microcatheter and was negotiated as far as the V3–V4 junction. These ultra-distal intracranial positions of the Navien catheter were achievable without any catheter-related injuries to the parent vessel.
Traditional guide catheters provided proximal support based on their rigid design, but this rigidity also limited their ability for intracranial positioning.10 As such, microcatheters often traveled significant distances unconstrained before reaching the target lesion intracranially, resulting in unpredictable microcatheter behavior. Advances in guide catheter technology led to the development of newer access catheters with a hybrid design of soft flexible distal tips while maintaining proximal support. Clinical experiences with these catheters, such as the Neuron and DAC, have demonstrated the safety of their routine positioning above the skull base for various types of neurointerventions.1–8 Intracranial guide catheter placement reduces the distance that the microcatheter travels unconstrained, allowing for a more stable microcatheter with more predictable behavior and enhanced control.1
Prior to this report, ultra-distal intracranial purchase in the cerebrovasculature with a guide catheter was described using the 5 F distal/6 F proximal 0.053 inch ID Neuron.5 Chaudhary and colleagues detailed 12 neurointerventions using the 0.053 inch ID Neuron in various distal locations including the M1, A1 and P1. In this report we were able to achieve similar ultra-distal positions with the larger 0.058 inch ID Navien as far as the M1 and with the 0.072 inch ID Navien in the V3–V4 junction without any complications. We concur with Chaudhary et al that distal guide catheter placement is essential in eliminating the increased friction between the microcatheter and the arterial wall in tortuous anatomy, thereby allowing more one-to-one movement of the microcatheter. Similar to the results of Chaudhary and colleagues, we found ultra-distal guide catheter positioning with the Navien facilitated the safety and effectiveness of various neurointerventions including stent-assisted coiling and liquid embolics. As described in the second illustrative case, the distal position of the Navien allowed SL-10 microcatheter access of the aneurysm through the stent tines without any forward jump of the microwire. Additionally, the SL-10 was extremely stable during coil deployments with little microcatheter kickback. Finally, the ultra-distal purchase with the 0.058 inch ID Navien was critical in providing needed support for PED deployments, which require significant microcatheter manipulations of pushing/pulling and subsequently more stresses on the distal guide catheter than traditional neurointerventions. The Navien catheter was able to absorb such added stresses to provide the necessary microcatheter support, and ultimately increase the success as well as safety of these neurointerventions with its ultra-distal intracranial location. Although the small number of cases in this report limits the generalizability of the data, the combined experience from this report and that of Chaudhary et al5 demonstrates that the added benefit afforded by ultra-distal intracranial purchase of the support catheter is achievable without catheter-related vascular injury.
The Navien catheters are the newest type of DICs designed in the era of flow diversion. These catheters have a larger ID to accommodate the 0.027 inch ID microcatheters needed for deployment of flow diverters.11 Similar to the Neuron and DAC, the Navien imparts support from the stability of being anchored around multiple bends rather than from the rigidity of traditional guide catheters. Among the guide catheters currently available in the USA, the 6 F 0.072 inch ID Navien at present provides the largest access. The additional room of the 0.072 inch ID compared with the 6.3 F 0.070 inch ID DAC and the 6 F 0.070 inch ID Neuron was particularly useful for jailed microcatheter coiling interventions.
Compared with its predecessors (5.2 F DAC and 5 F distal/6 F proximal Neuron), the 5 F 0.058 inch ID Navien has a smaller OD, being a true 5 F throughout its entire length. Its smaller profile permits its improved conformability to the parent vessel, higher trackability and atraumatic nature. We attribute the success of our previously described pseudo-corking technique in PED procedures12 to the superior performance profile of the Navien. Additionally, in our previous report of using the Navien in PED procedures, we demonstrated 100% clinical success with tracking the Navien to its intended final position (most commonly the proximal cavernous ICA).11 In this current report we were able to obtain ultra-distal access with the Navien as far as the M1 segment and basilar artery. Such ultra-distal intracranial access in anterior circulation interventions can be readily achieved with the triaxial system. This technique eliminates potential friction forces between the Navien and the parent arterial wall, allowing more proximal support of the Navien which can then be advanced into more distal intracranial locations. Previous experiences with the Neuron and DAC have demonstrated the safety and ease of the triaxial system.3–5 ,8 Compared with traditional access with a proximally placed guide catheter, this technique of ultra-distal intracranial access with the triaxial system provides added advantages of improved microcatheter feedback and one-to-one microcatheter movement, improving the overall procedural safety and success. Additionally, the modern neurointerventionalist will need to become facile with constructing triaxial support systems as neuroendovascular technology continues to evolve with new devices, such as flow diverters, that require larger (0.027 inch ID) microcatheters and subsequently distal intracranial support.
The combination of a smaller OD with a larger ID in the Navien catheter also provides several ways to acquire necessary intraprocedural roadmaps and runs. Intraprocedural injections were previously impaired with the predecessor catheters, Neuron and DAC. Hauck and colleagues reported that using a DAC with a 6 F Envoy (Codman Neurovascular, Raynham, Massachusetts, USA) compromised the ability to obtain roadmaps and recommended using a 7 F guide instead.4 In our experience, the true 5 F nature of the Navien when used in the triaxial system enables sufficient intraprocedure runs/roadmaps previously not possible with the 5.2 F DAC and 5 F distal/ 6 F proximal Neuron. Figure 3C demonstrates the typical quality of these roadmaps. The larger ID of the Navien also enables functional intraprocedure roadmaps and angiography with a microcatheter endoluminally. The 5 F Navien has a larger 0.058 inch ID compared with the 0.057 inch ID DAC and the 0.053 inch ID Neuron. This larger ID provides adequate room for improved flush and contrast injections while accommodating larger profile balloons or 0.027 inch microcatheters. This was not previously possible with the Neuron and DAC, which had sacrificed the necessary larger ID for their soft flexible tips. In their experience with the DAC, Binning and colleagues noted that, although distal intracranial positioning was feasible, sufficient roadmaps through the DAC were impaired with the microcatheter in place.7
The successes of the Navien catheters are not without a few limitations. Although the hyperflexibility of the Navien catheter allows for its atraumatic maneuverability and high trackability, this also limits the catheter's proximal support. This drawback can be remedied in anterior circulation interventions by using a triaxial system where the Shuttle sheath can provide the necessary proximal support and in posterior circulation embolizations by using a long sheath ((≥55 cm) positioned in the subclavian artery or the proximal vertebral artery. When used in the posterior circulation, the Navien's soft straight tip makes direct catheterization of the supra-aortic vessels challenging. As such, we recommend an exchange technique with a diagnostic glide catheter to introduce the Navien catheter into the subclavian artery or the proximal vertebral artery.
Conclusion
The Navien catheter is the newest type of hyperflexible guide catheter that can be successfully negotiated atraumatically into ultra-distal intracranial positions that were unachievable with previous generations of similarly sized guide catheters. This can be routinely performed as part of a triaxial construct. Enhanced microcatheter control with the distal intracranial access overcomes technical challenges inherent with increased parent vessel tortuosity, ultimately enhancing the safety of the procedure. These Navien catheters have allowed neurointerventionalists to move more distally into the cerebrovasculature and to perform complex intracranial interventions without sacrificing the necessary ID for injections and roadmaps.
Footnotes
-
Contributors All authors contributed to the design, implementation and writing of this manuscript.
-
Competing interests ALC is a proctor for the Pipeline Embolization Device (Covidien, Mansfield, Massachusetts, USA) and a consultant for Covidien. The other authors have no conflicts of interest. No author received financial support in conjunction with the generation of this submission.
-
Ethics approval Ethical approval was obtained from the Johns Hopkins University School of Medicine Institutional Review Board.
-
Provenance and peer review Not commissioned; externally peer reviewed.