Article Text

Abstract
Background The Pipeline Embolization Device (PED) has become an important tool in the treatment of complex cerebrovascular pathology since it was approved by the Food and Drug Administration in April 2011.
Objective To determine the overall complication rate (permanent and transient) associated with the use of this new device from a single institution.
Methods We retrospectively examined a prospectively maintained database of our patients treated with the PED since its availability to the current time. 126 patients (24 men, 102 women; age range 14–83 years, mean 59.8 years) were treated for a total of 137 intracranial aneurysms, one cervical internal carotid artery dissection, one cervical vertebral artery dissection, and one carotid-cavernous fistula with a total of 217 PEDs (1.72 PED/patient).
Results A total of 40 complications were experienced by 33 patients in our cohort. Four complications (4/126, 3.2%) in four patients were permanent, resulting in three deaths and one permanent disability. The other 36 complications (28.6%) occurred in 29 patients, all of whom went on to recover completely. The total complication rate associated with the use of the PED was 31.7% (40/126).
Conclusions Despite a low rate of permanent complications associated with the PED in this series, the total complication rate was high. This finding supports the conclusion that this device should be reserved for the most challenging aneurysms. Patients should be advised of this higher rate of transient periprocedural complications.
Trial registration number IRB#:14BN027 Q7.
- Complication
- Device
Statistics from Altmetric.com
Introduction
With the introduction of the Pipeline Embolization Device (PED; eV3/Covidien, Irvine, California, USA) and flow-diverting stent (FDS) technology in 2011, neurointerventional surgeons have been able to tackle an increasingly more difficult subset of cerebrovascular pathology. In particular, large or giant, wide-necked, and/or fusiform cerebral aneurysms, which previously may have been considered untreatable by conventional neurointerventional or surgical techniques, have been cured with PEDs. An extensive body of published medical literature now exists describing the use of this new technology to the betterment of patient care.1–9
While the on-label indications for use of the PED have been limited to wide-necked aneurysms of the petrous to superior hypophyseal internal carotid artery (ICA), the medical literature is replete with case reports and series describing the use of FDS in original and creative new ways. This off-label use of PED, in particular, is a natural progression in the evolution of novel medical technologies.4 ,10–17
While FDS in general, and PED in particular, represent a significant technological advancement in the treatment of cerebrovascular pathology, caution must be exercised in the wholesale adoption of the ‘new’ without a thoughtful and judicious examination of the unintended consequences that that technology may harbor. Thus, it is incumbent upon the practitioner to better understand the potential risks and complications of any new intervention, technique, and/or medical device which one may wish to offer those under their care. To this end, we examined the temporary and permanent complications, neurological and otherwise, associated with the use of the PED in the treatment of on-label and off-label cerebrovascular pathology at our center.
Materials and methods
Approval for this research project, including a waiver of informed consent, was obtained from the Institutional Review Board at Barrow Neurological Institute.
A retrospective review of a prospectively maintained endovascular neurosurgical database was performed to identify all patients treated with the PED at our institution following completion of enrollment in the Pipeline for Uncoilable or Failed Aneurysms (PUFs) study in June 2009.3 Data collected from the inpatient and outpatient medical records and imaging studies included demographics (patient age and gender), cerebrovascular pathology treated, vessel location, size of aneurysm (if applicable), number of PEDs used in the procedure, dates of angiographic follow-up, and any complications related directly or indirectly to the device or the procedure (table 1). Furthermore, in the event of a procedure- or device-related complication, we attempted to identify any potential cause, contributing factor, or mitigating circumstance with regard to the untoward event.
Patient demographics
All procedures were performed by the senior authors (CGMcD and FCA) at a single institution. All patients underwent the neurointerventional procedure under general anesthesia with neuromonitoring (EEG, somatosensory evoked potentials (SSEP) and, for posterior circulation cases, brainstem auditory evoked response (BAER)) and placement of arterial lines for blood pressure monitoring and indwelling Foley catheters. Patients were routinely administered a loading dose of heparin (70 units/kg) following groin puncture and maintained activated clotting times between 250 and 300 s throughout the duration of the procedure. Patients were either premedicated with aspirin 325 mg and clopidogrel 75 mg daily for at least 5 days prior to the procedure or received a loading dose of abciximab (Reopro; Eli Lilly, Indianapolis, Indiana, USA) after deployment of the PED followed by an oral loading dose of aspirin 625 mg and clopidogrel 600 mg as early as possible after extubation. The response to antiplatelet medications was routinely assessed with aspirin response and VerifyNow (Accumetrics, San Diego, California, USA) P2Y12 inhibition assays.
At the completion of the procedure the femoral access sites were all closed with the Angio-Seal closure device (St Jude Medical, Austin, Texas, USA). Foley catheters were routinely removed either prior to extubation or 2 h after femoral access site closure when the patient could be mobilized from bed. All patients were admitted to a dedicated neurointensive care unit for the first 24 h following the procedure. Follow-up cerebral angiography was routinely obtained 6, 18, and 36 months after the initial procedure. Dual antiplatelet coverage was continued until the first follow-up cerebral angiogram was performed (minimum 6 months), after which the patient was changed to single antiplatelet coverage with aspirin 325 mg daily.
Results
Patient characteristics
One hundred and twenty-six consecutive patients (24 men, 102 women) were treated from May 2011 to October 2013 with the PED for various intra- and extracranial cerebrovascular pathologies (table 1). The age range of the patients was 14–83 years (mean (SD) 59.8 (14.7) years).
There were a total of 137 cerebral aneurysms, two arterial dissecting pseudoaneurysms (one cervical ICA, one cervical vertebral artery), and one carotid-cavernous fistula treated with a total of 217 PEDs (1.72 PED/patient). Two patients were treated in the setting of a subarachnoid hemorrhage. The mean (SD) size of the cerebral aneurysms was 12.1 (8.3) mm. One hundred and twelve cases involved the anterior circulation and 16 patients were treated with PEDs in the posterior circulation. Forty-eight cases were for on-label indications and 80 were used off-label. The mean (SD) length of follow-up for the series was 9.0 (5.6) months.
There were four permanent complications (3.2%, 4/126) resulting in three deaths and one instance of permanent morbidity. A further 36 complications occurred in 29 patients (26.5%, 36/126), all of whom made complete recoveries from the complications. The total complication rate in our series was 31.7% (40/126).
The mean (SD) age of the 33 patients who experienced any type of complication was 60.5 (16.3) years (table 1). There were seven men and 26 women in this group. Thirty-one patients had intracranial cerebral aneurysms, one patient had a traumatic pseudoaneurysm of the supraclinoid ICA, and one patient had an extracranial dissecting pseudoaneurysm of the ICA treated with PEDs. Twenty-six of the procedures involved the anterior circulation and seven involved the posterior circulation. The mean (SD) size of cerebral aneurysms treated with the PED was 14.3 (9.3) mm. There were 12 on-label procedures and 21 off-label cases among the patients who developed complications. The mean (SD) follow-up was 7.3 (3.8) months. No independent factor was found to be a statistically significant predictor of complications.
Complications
Overall, there were four permanent complications in four patients (4/126, 3.2%) resulting in death or permanent morbidity and 36 temporary complications in 29 patients (36/126, 28.6%), all of whom went on to recover to their full baseline states. There were four cerebrovascular accidents (CVA) resulting in one death within 30 days of the treatment (4/126, 3.2%). Two deaths occurred more than 30 days after the treatment date.
The types of complications can be analyzed in a number of ways. While any classification scheme for these events is somewhat arbitrary, we have attempted to organize the complications according to those occurring at the time of the procedure versus those presenting in a delayed fashion (box 1). In addition, procedural complications can be further subdivided into those which one could potentially encounter during any neurointerventional procedure versus complications related to the unique attributes of the PED and the technique required to deploy it. Often the complications cannot be neatly placed within one distinct category but, rather, result from a combination of related factors.
Complications
Permanent complications
3 delayed thromboembolic events resulting in CVA and death
1 delayed contralateral CVA/hemorrhage
Temporary complications
Procedural complications
Procedure-related
4 vessel dissections
3 groin hematomas
3 vessel perforations
2 UTI/pyelonephritis
2 return to angio suite during same hospitalization
1 aneurysm perforation
1 urethral trauma
Device-related
2 perforator/side branch occlusions
1 intraprocedure PED occlusion
1 lead wire breakage
Delayed complications
Device-related
4 delayed PED occlusions
3 TIA/CVA post-procedure
2 PED contractions
2 neurological deficits from mass effect of treated aneurysm
1 delayed development of CCF
1 delayed occlusion of side branch
Medication-related
3 GI bleeds
40 total complications in 33 patients
CCF, carotid-cavernous fistula; CVA, cerebrovascular accidents; GI, gastrointestinal; PED, Pipeline embolization device; TIA, transient ischemic attacks; UTI, urinary tract infection.
Procedural complications
There were eight instances of injury to the vessel or aneurysm (four iatrogenic dissections, three vessel perforations, and one cavernous ICA aneurysm perforation resulting in carotid cavernous fistula). Other procedural complications not necessarily related to the PED included groin/retroperitoneal hematomas, urinary tract infections/pyelonephritis, and urethral trauma following attempted Foley catheter placement requiring placement of a suprapubic catheter.
One PED did not expand fully resulting in complete occlusion of the parent vessel during the procedure (figure 1). Fortunately, the patient had sufficient collateral circulation to tolerate the acute occlusion without changes to SSEP monitoring and the decision was made to reinforce the unintentional vessel occlusion with coil embolization of the parent artery to minimize the opportunity of thromboembolic events.

Intraprocedural occlusion of the parent artery by incompletely expanded Pipeline embolization device (PED). (A) Cerebral angiogram in the working angle projection of a patient with an 18 mm left cavernous internal carotid artery (ICA) aneurysm. (B) Mid-deployment of the PED demonstrating incomplete expansion of the device around the supraclinoid ICA (arrows indicate area of incomplete expansion). (C) Despite incomplete expansion of the PED, mid-deployment angiogram demonstrates patency of the distal ICA. (D) Final deployment native view with foreshortened and incompletely expanded PED (arrows). (E) Post-deployment angiogram demonstrating complete occlusion of the left ICA. (F) Right ICA angiogram demonstrating collateralization across patent anterior communicating artery. (G) Final native view following coil embolization of cavernous ICA aneurysm and parent artery occlusion. Used with permission from Barrow Neurological Institute.
In another instance the lead portion of the delivery wire could not be removed. The lead wire was torqued off and left within the vessel (figure 2).

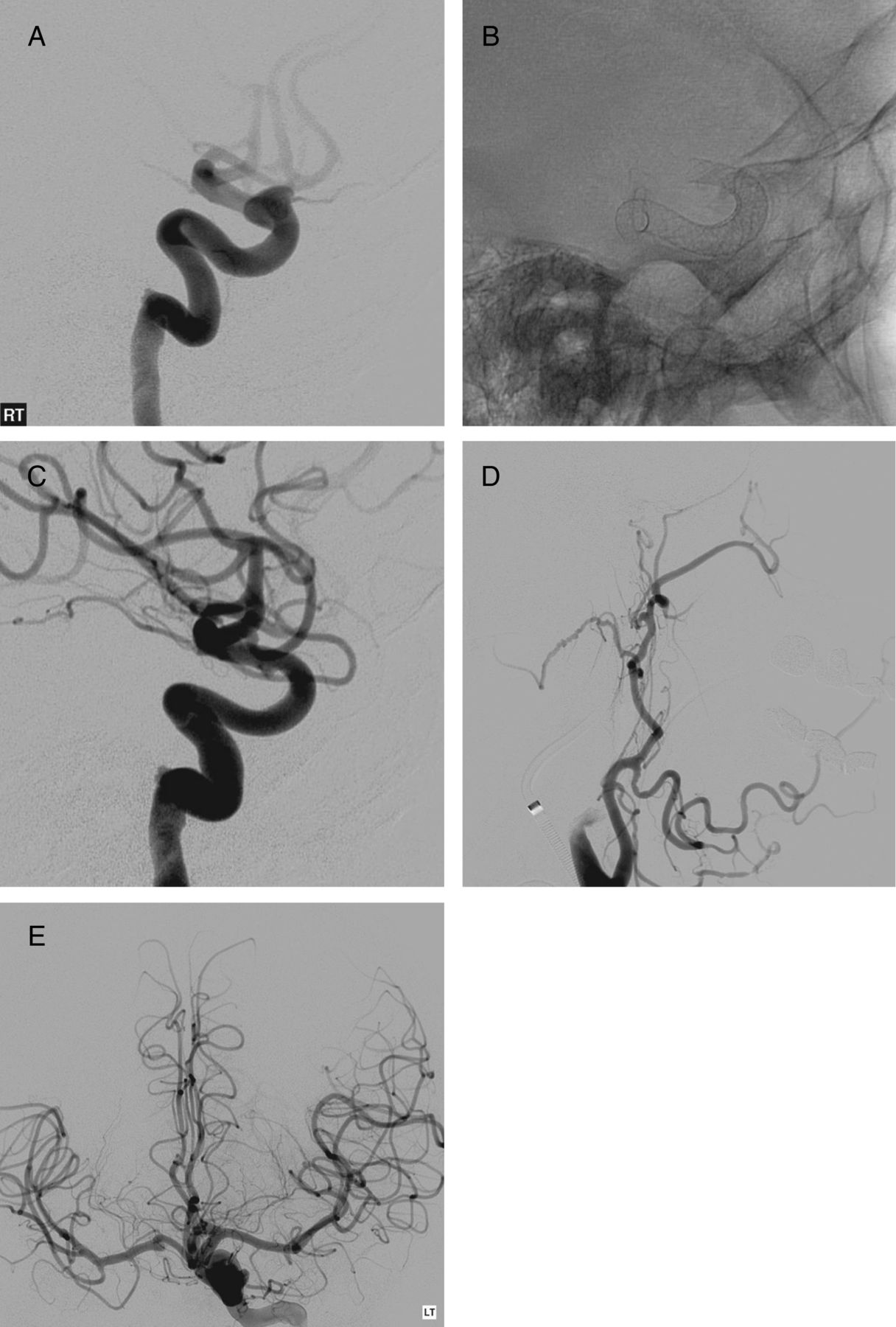
Lead wire breakage during deployment of the Pipeline embolization device (PED). (A) Pretreatment angiogram of a recurrent mid-basilar artery aneurysm in a patient after coil embolization. (B) Angiogram following coil embolization and initial PED placement. Note the proximal portion of the PED (white arrowhead) does not fully cover the aneurysm neck (arrow). (C) Native view following second PED deployment with broken lead wire (arrow) in the right posterior cerebral artery. (D) Post-deployment angiogram demonstrating extralumenal position of the broken lead wire (arrow). Also, thrombus (white arrowhead) is present within the PED and bilateral superior cerebellar artery origins which was treated successfully with abciximab. Used with permission from Barrow Neurological Institute.
Delayed complications
Four patients experienced transient ischemic attacks or a CVA following the procedure not related to device occlusion. Three patients went on to make a complete recovery while one patient had a significant CVA approximately 1 month after the procedure. This patient was admitted to an outside hospital and died there; we were unable to obtain the medical records from that hospital admission. Of the other three patients who made complete recoveries following their neurological complication, one was noted to have a thrombus within the PED requiring thromboaspiration. One patient had a CVA 2 days after PED deployment and was treated at an outside institution. Upon transfer to our institution, a follow-up angiogram demonstrated patency of the PED and all distal vessels. The final individual had no angiographic evidence of PED complications.
Six additional patients were noted to have complete occlusion of the PED and parent artery on follow-up studies (figure 3). Two of these patients had devastating neurological deficits and died as a result. An additional four individuals with occlusion of the device had no neurological sequelae. In one of the patients one PED was used to treat a supraclinoid ICA aneurysm and another PED was used to treat an iatrogenic cervical ICA dissection. On a short interval follow-up angiogram 2 days later the cervical ICA was noted to be completely occluded.
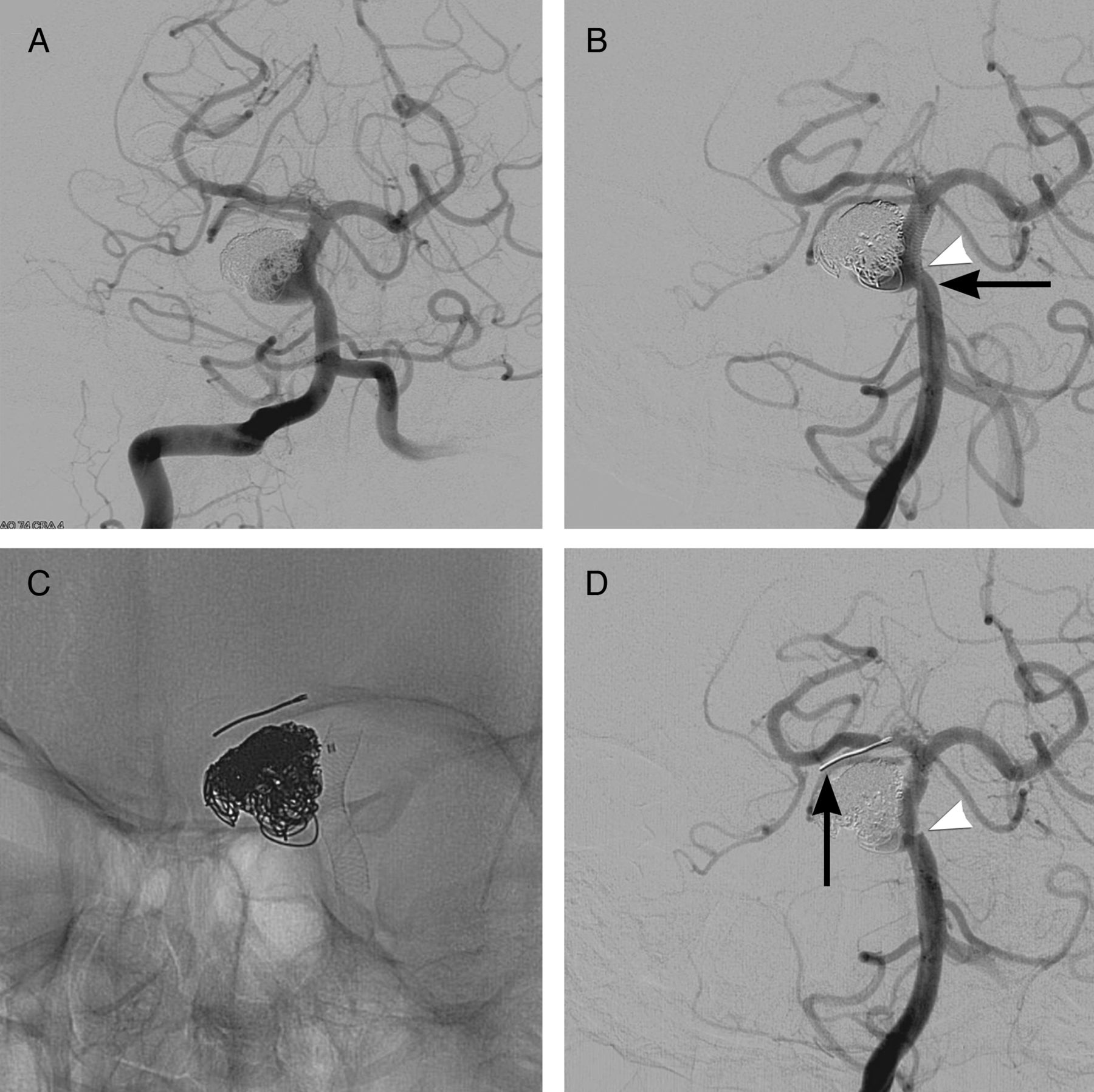
Delayed Pipeline embolization device (PED) occlusion. (A) Working angle projection of a right ophthalmic segment aneurysm in a septuagenarian patient. (B) Native projection following deployment of two PEDs. (C) Final angiogram following placement of two PEDs. (D) Short interval follow-up angiogram 2 weeks later during attempted treatment of contralateral internal carotid artery aneurysm demonstrating occlusion of previously treated left internal carotid artery (arrow). (E) Left internal carotid artery injection demonstrating collateral filling across anterior communicating artery. Used with permission from Barrow Neurological Institute.
In two instances the PEDs contracted, leaving a portion of the aneurysm neck uncovered (figure 4). This required additional treatment to cover the exposed portion of the aneurysm properly.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Pipeline embolization device (PED) contraction. (A) Initial working angle projection of a recurrent posterior communicating artery aneurysm following clipping. (B) Native view following placement of two telescoping PEDs; note proximal and distal positions of the stent (arrows). (C) Immediate post-placement angiogram demonstrating continued aneurysm filling and patent PED. (D) Native view 6 months after initial procedure demonstrating distal stent contraction (arrow). (E) Final native view after additional PED placement (arrow). (F) Nine-month follow-up angiogram demonstrating complete occlusion of aneurysm. Used with permission from Barrow Neurological Institute.
Three patients developed gastrointestinal bleeding complications related to the use of dual antiplatelet medications. One patient treated with a PED for a traumatic carotid cave/cavernous ICA pseudoaneurysm developed a direct carotid-cavernous fistula on short-term follow-up studies. This individual was successfully treated with transvenous coil embolization of the fistula.
Discussion
Complications associated with the use of the PED have been widely documented in the literature (table 2). A recent systematic review of 10 publications involving PED use in 414 patients with 448 cerebral aneurysms identified an overall procedural complication rate of 10.3% (46/447), with an intracranial vascular complication rate of 6.3% and procedural mortality of 2.2% (9/413).18 When eliminating ruptured cerebral aneurysms from their series, there was a major intracranial vascular complication rate of 6.8% and 0.8% mortality in 394 patients.18 A larger meta-analysis of 29 studies performed by Brinjikji et al2 including 1451 patients with 1654 aneurysms noted a procedure-related morbidity of 5% and mortality of 4%. The overall complication rate in the PUFs trial, defined as major ipsilateral stroke or neurological death, was 5.6% (6/107).3 The PED for the Intracranial Treatment of Aneurysms (PITA) trial reported two major periprocedural strokes in 31 patients with no delayed neurological deterioration on clinical follow-up at 180 days.5 Similarly, Fargen et al19 reported a mortality rate of 1.3% and major complication rate of 5.3% in their review of complications associated with the PED.
Complications
Vascular injury
While these complications can occur in any neurointerventional procedure, there are certain aspects unique to this device which may predispose to vessel or aneurysm injury. Because of the unique design of the PED, deployment of the device often requires a stiffer triaxial support platform than other neurointerventional treatments for aneurysms.20 The PED can be deployed through a Marksman microcatheter (eV3/Covidien; 2.8 F outer diameter, 0.027 inch inner diameter) or a microcatheter of similar size.
During deployment the PED is alternately unsheathed with a ‘left to right’ hand motion withdrawing the catheter over the PED, ‘packed’ to increase the density of the lumenal coverage at the neck of the aneurysm with a ‘right to left’ motion, and ‘wagged’ by advancing and withdrawing the delivery wire and microcatheter together to allow for deployment of the device around arterial curvatures. While the lead wire is designed to be as atraumatic as possible, there is still considerable movement of the wire during the deployment process. We described one case in particular where the lead wire of a second PED was retained within the posterior cerebral artery during treatment of a recurrent mid-basilar artery aneurysm (figure 2). Following initial balloon-assisted coiling of the recurrent aneurysm, the first PED was deployed in the basilar artery. However, the device did not fully cover the neck of the aneurysm and the decision was made to add a second device. During the course of deploying the second PED the lead wire was noted to travel in an extralumenal position. Because the PED is not retrievable, the decision was made to continue with deployment of the PED and address the complication afterwards. There was no contrast extravasation noted on immediate post-deployment angiography. After unsuccessful attempts to remove the wire, the distal portion of the wire was fractured off by torquing the delivery wire and left in place. Thrombus was also noted within the origins of the superior cerebellar arteries and treated with intra-arterial abciximab infusion. Immediate post-procedure CT of the head did not demonstrate any evidence of contrast extravasation, subarachnoid hemorrhage, or infarcts. We suspect that the lead wire became trapped and stuck within a perforator rather than perforating through the posterior cerebral artery, given the lack of contrast extravasation or subarachnoid hemorrhage. The patient remained neurologically intact following the procedure and was discharged home several days later.
The use of a triaxial catheter system and/or the stiffness of the PED may contribute to the increased rate of vessel injury which we encountered in our series. Particularly with more tortuous anatomy, the navigation of the device to the target lesion becomes increasingly more difficult and may result in treatment failures.7 In the PITA series the authors describe six instances where they were unable to deliver the initial device through the microcatheter due to excessive friction.5 However, in all six cases the procedure was ultimately successful with subsequent attempts.
Thromboembolic events and device occlusion
There are several unique attributes of the PED which may play a role in the increased occurrence of complications in our series. The bimetallic cobalt chromium and platinum tungsten PED provides 30–35% wall coverage using a novel 48-strand braided construction. The microcell architecture provides increased wall coverage and is essential for its function as a FDS. However, the increased amount of metallic surface of the stent may increase the thrombogenicity of the device.
We identified device thrombosis in both an acute and delayed fashion in our cohort. Very late device occlusions 23 months after initial treatment have also been described in the literature.21 The use of coils with the PED may also increase the thrombogenicity of the ultimate construct. Siddiqui et al22 hypothesized that extensive packing of aneurysms with coils may have affected the delayed PED occlusion in their case report.
As with all intracranial stents, it is imperative that the patient is on dual antiplatelet coverage for the procedure.23–25 Patient compliance with the drug regimen plays an integral role in the ultimate success of the procedure because, as in our series, early termination of the dual antiplatelet medications or discontinuation of chronic aspirin therapy can have significant deleterious effects.
Tan et al24 reported thromboembolic complications in 5/74 patients (6.8%) treated with the PED for on-label and off-label indications. They noted that patients who responded to dual antiplatelet therapy with P2Y12 reaction unit (PRU) values >208 were more likely to have thromboembolic complications (12.8%, 5/39) than those with PRU values <208 (0%, 0/35). However, this difference did not reach statistical significance (p=0.06) in their series. Similarly, Delgado Almandoz et al23 identified low or high PRU values (<60 or >240) as the only independent risk factor in multivariate analysis of all and major complications in their series of 48 PED procedures in 44 patients. The only major thromboembolic complication occurred in one of two procedures where the last recorded PRU was >240. Interestingly, their one instance of delayed asymptomatic PED occlusion occurred in an individual within the safe therapeutic PRU range.
Another possible source for thrombosis of the PED involves the increasing recognition of resistance to clopidogrel in certain patients.25 ,26 Despite the real risk of thromboembolic complications, there is no uniform consensus on antiplatelet medication use or monitoring among centers and practitioners following neuroendovascular procedures.27 Faught et al27 noted that less than half (46.8%) of responders to an email study used point of care testing for antiplatelet response during their procedures. Furthermore, the extent of antiplatelet response necessary for risk mitigation is still a matter of some controversy without a uniform definition across all centers.
Whether or not device occlusion results in significant neurological morbidity is solely related to the extent of collateral circulation. Although four of our patients who developed delayed device occlusion while on proper antiplatelet coverage remained clinically asymptomatic, this will certainly not be the case for every individual.
Contralateral intracranial hemorrhages
While the phenomenon of delayed ipsilateral intracranial hemorrhage after the use of the PED has been described in the literature, in our series there was only one instance of delayed intracranial hemorrhage following PED use on the contralateral side of treatment.8 ,28 Our patient initially experienced a contralateral CVA following the procedure with delayed hemorrhagic conversion probably influenced by the need for dual antiplatelet medications. Unfortunately, there was no identifiable cause for the contralateral CVA in this individual.
Chitale et al8 described two patients who experienced contralateral hemorrhages following PED placement. One patient in their series was noted to have an occult contralateral cervical ICA dissection which was not observed on previous studies. Their second patient had no known explanation for the contralateral intraparenchymal hemorrhage. Unfortunately, these events represent a particularly challenging diagnostic and management dilemma since there is no clear etiology for this potentially devastating complication, as noted by Chitale et al.8 Certainly, use of dual antiplatelet medications in the setting of an intracranial hemorrhage will only exacerbate an already difficult situation.
Perforator/side branch occlusion
We encountered two instances of perforator or side vessel occlusion at the time of treatment. In one patient a basilar trunk aneurysm was treated with two PEDs and coil embolization. A large mid-basilar perforator was occluded by the PED, but flow was re-established following the administration of intra-arterial abciximab. A second patient developed occlusion of an A1 vessel after placement of a single PED for treatment of an ICA blister aneurysm. Flow was re-established following aspiration of the thrombus using the Penumbra thromboaspiration system (Penumbra, Alameda, California, USA) and administration of intra-arterial abciximab. Fortunately, in both cases there were no untoward long-term neurological deficits. Similarly, Lall et al29 reported three cases of acute side branch/perforator occlusion following placement of a PED for treatment of two giant posterior circulation aneurysms and one previously clipped and coiled middle cerebral artery aneurysm in patients with an adequate preprocedural response to dual antiplatelet therapy. In all three instances vessel patency was restored following intra-arterial administration of abciximab without neurological sequelae.
In one of our cases an ophthalmic artery occluded in a delayed fashion following treatment of an ophthalmic artery aneurysm without incident.30 Similarly, Puffer et al31 described four delayed occlusions of the ophthalmic artery in 19 patients treated with the PED. They theorized that side branches with distal collateral flow (ie, ophthalmic artery) may be more predisposed to occlusion than side branches which are end arteries (ie, anterior choroidal or lenticulostriate arteries). Szikora et al7 described one acute ophthalmic artery occlusion resulting in a small visual field deficit and two delayed occlusions without clinical sequelae.
In other instances in the literature, monocular visual loss following PED use was not associated with ophthalmic artery occlusion. Chitale et al8 described one patient who presented with delayed monocular blindness 29 days following treatment and 8 days after a follow-up angiogram demonstrated patency of the ophthalmic artery. Fortunately, the vision was recovered to baseline within 6 months. Likewise, Sise et al32 described delayed monocular visual loss with distal retinal artery branch occlusion on ophthalmological examination with fluoroscein angiography following use of two telescoping PEDs for a small supraclinoid ICA aneurysm. A follow-up cerebral angiogram noted patency of the ophthalmic artery with preserved retinal blush and the patient's vision returned to baseline. The authors suggest that emboli may have formed on the PED as a result of the procedure with migration and occlusion of distal branches.
Other complications
Certainly the overall percentage of complications (31.7%) appears much higher than that reported in the medical literature. However, our series differs from other previously described series in its inclusion of all complications experienced by our patients following the initial procedure, rather than limiting complications solely to neurological events.2 ,4 ,6 ,8 ,18 In one of the few studies to look at non-neurological complications Lylyk et al9 cites minor complications in six of 53 patients (11%), five of whom had groin site hematomas.
We also identified three patients with significant gastrointestinal bleeds following institution of dual antiplatelet therapy. This is of particular concern given the risk of thrombosis of the PED without proper pharmacological coverage and presents a management dilemma should the bleeding be of sufficient concern. There were also three groin hematomas, two urinary tract infections, and one significant urethral trauma during Foley catheter insertion requiring placement of a suprapubic catheter in our series. These complications, while not directly related to the use of the PED, may be encountered in any neurointerventional procedure. If we eliminate all minor non-neurological complications from our series, the overall complication rate would decrease by half, bringing it in line with reported complications in other series.8 ,9 Even though it may seem somewhat trivial to include these types of complications in our series, it will probably become more important to identify these issues in the changing healthcare landscape of accountability and outcomes.
Conclusion
While the PED represents a significant addition to the armamentarium of neurointerventionalists, it does come at some increased cost, as evidenced by our high overall complication rate. Even though the rate of permanent morbidity and mortality was low in our series, there were other significant device complications (ie, acute and delayed occlusion of the PED) and procedural complications (loss of side branch/perforators) which, in other patients, may have ended with disastrous results. Knowledge of the complication rates associated with the use of new technology is necessary in order to make the best decisions possible when counseling our patients. Thus, it has been our practice to limit the use of FDS to those cases in which other more established neurointerventional treatments are not well suited. Given our initial data, it is clear that additional research into this complex issue is necessary before definitive conclusions can be drawn.
References
Footnotes
Contributors All authors made substantial contributions to the conception or design of the work; or the acquisition, analysis, or interpretation of data for the work; and drafted the work or revised it critically for important intellectual content; and provided final approval of the version to be published; and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Competing interests None.
Ethics approval Ethics approval including a waiver of informed consent was obtained for this study (Institutional Review Board of St Joseph's Hospital and Medical Center, Phoenix, Arizona).
Provenance and peer review Not commissioned; externally peer reviewed.