Article Text

Abstract
Subarachnoidal release of inflammatory cytokines (interleukin (IL)-1β, IL-6, and tumour necrosis factor (TNF)-α) was characterised in 35 patients with subarachnoid haemorrhage (SAH) and control subjects and compared with development of complicating haemodynamic abnormalities in basal cerebral arteries and clinical outcome. Serial analysis allowed the observation of a subacute response profile of these key mediators of inflammation in the subarachnoidal space. This compartmentalised inflammatory host response was closely associated in time and extent with development of increased blood flow velocities in the basal cerebral vessels as recorded by transcranial Doppler sonography. Moreover, intrathecal secretion of inflammatory cytokines was significantly increased in patients with poor clinical outcome. Together, these findings suggest a role of excessive compartmentalised inflammatory host response in pathogenesis of cerebrovascular complications after SAH.
- subarachnoid haemorrhage
- inflammatory cytokines
- cerebral blood flow
- vasospasm
- cerebral ischaemia
Statistics from Altmetric.com
Subarachnoid haemorrhage (SAH) most commonly occurs when an aneurysm in a basal cerebral artery ruptures. Among patients who survive this event, the leading cause of death and disability is subsequent constriction of the large cerebral arteries causing delayed cerebral ischaemia, the “second stroke”.1 2 Monitoring of cerebral blood flow velocities (CBFVs) in the large pial arteries identifies patients with SAH with raised risk for ischaemic complications.3-6 In SAH, it has been shown in multiple studies that CBFVs on transcranial Doppler sonography are inversely related to vessel diameters on angiography.3-6 The non-invasive character of this technique enables serial investigations of developing haemodynamic abnormalities in an individual patient.
Earlier studies described inflammatory changes in SAH—that is, subarachnoidal and perivascular leucocytic infiltrates in the subarachnoidal space7-9 in relation to development of cerebral vasospasms.8 9 Moreover, the proinflammatory cytokines interleukin (IL)-1β, IL-6, and tumour necrosis factor (TNF)-α that orchestrate the cascade of inflammatory host response to infection and tissue damage10 11 have been detected in the CSF of patients with SAH.12-16
These earlier findings suggest an inflammatory pathogenesis of vasospasms in SAH. In this study, we tested the hypothesis that the extent and pattern of secretion of key mediators of inflammation IL-1β, IL-6, and TNF-α are associated with development of haemodynamic abnormalities in basal cerebral arteries and with clinical outcome.
Patients and methods
PATIENTS AND CONTROL SUBJECTS
Thirty five patients (21 women and 14 men), aged between 23 and 76 (median 56) years with SAH caused by aneurysmal rupture and presenting within 48 hours after onset of first symptoms were studied. Hunt and Hess scores to classify disease severity were 1 in 9%, 2 in 11%, 3 in 32%, 4 in 29%, and 5 in 18% of the patients. Extent and location of haemorrhage according to the Fisher scale were grade 2 in 12%, 3 in 85%, and 4 in 3%. All except four patients underwent surgical obliteration of the aneurysm earlier than 72 hours after the onset of symptoms. Patients were mechanically ventilated when signs and symptoms of increased intracerebral pressure were present. Ventilation was necessary in 66% of the patients. Therapy consisted of combined induction of hypervolaemia, hypertension, and haemodilution (triple H therapy) alone in 49%, combined with nimodipine in 20%, with angiographically administered papaverin in 6%, and with nimodipine alone in 6% of the patients. In all 35 patients, release of proinflammatory cytokines in CSF and peripheral blood and cerebral blood flow velocities in the basal cerebral arteries were assessed at day 5. In addition, in 20 of the patients, all of these haemodynamic and biochemical variables were longitudinally investigated at days 1, 2, 3, 5, 7, 9, and 11 after SAH.
Further, we included 20 control subjects (12 women and eight men), aged between 23 and 80 (median 40) years. These had lumbar puncture for initially suspected haemorrhage or meningitis, which was excluded by extensive clinical, neuroradiological, and laboratory investigation including CSF analysis.
MONITORING OF CBFVs AND ASSESSMENT OF CLINICAL OUTCOME
Abnormalities of CBFVs were monitored by non-invasive transcranial Doppler sonography using a DWL Multidop X TCD device (DWL Sipplingen, FRG). Systolic CBFV values were recorded transtemporally in the proximal segments of the anterior, middle, posterior, and basilar cerebral arteries as described before.17 All patients had follow up CT at least twice to assess possible delayed cerebral ischaemia. In each patient, the score of the Glasgow outcome scale (GOS) was determined. This study was approved by the ethics committee of the Mannheim Clinic, University of Heidelberg.
MEASUREMENT OF PROINFLAMMATORY CYTOKINES
Plasma concentrations of proinflammatory cytokines (IL-1β, IL-6, and TNF-α) were quantified with sandwich immunoassays (R and D Systems, Minneapolis, MN, USA) as described before.18Briefly, a monoclonal antibody specific for the antigen of interest was coated onto a 96 well microtitre plate. In a single step reaction, samples were then incubated in the microtitre plate together with a second horseradish peroxidase linked monoclonal antibody specific for a different epitope. After washing, the bound enzyme-antibody conjugate was measured enzymatically with tetramethylbenzidine as the substrate. Adsorbence was measured at 450 nm on an MR 4100 spectrophotometer (Dynatech, Burlington, MA, USA) using 630 nm as the reference wavelength. The lower limits of detection for IL-1β, IL-6, and TNF-α were 0.3 pg/ml, 0.3 pg/ml, and 4.4 pg/ml, respectively.
STATISTICAL ANALYSIS
Results are expressed as means (SEM). Statistical analysis involved a Mann-Whitney U test and calculation of Spearman‘s correlation coefficient.
Results
CHARACTERISATION OF INTRATHECAL RELEASE OF PROINFLAMMATORY CYTOKINES IN SAH
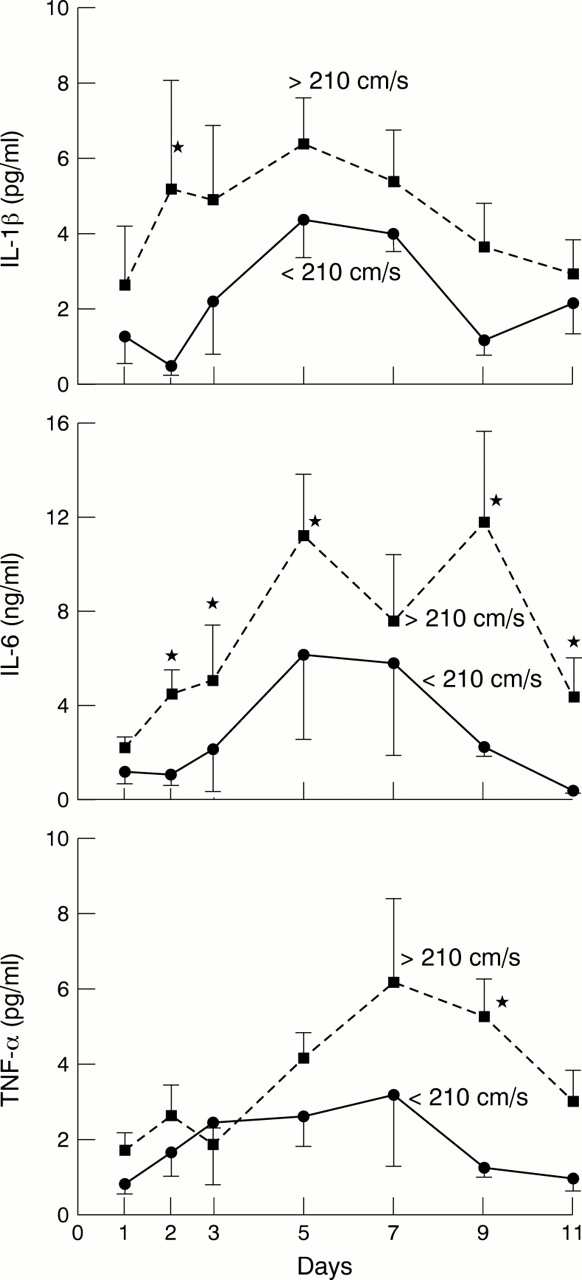
Concentrations of IL-1β, IL-6, and TNF-α in the CSF of control subjects were 0.00 (0.00) pg/ml, 0.0004 (0.0001) ng/ml, and 0.18 (0.16) pg, respectively. Compared with these normal values, CSF concentrations of proinflammatory cytokines in patients with SAH were massively increased in SAH (fig 1)—for example, CSF concentrations of IL-6 were increased up to 10 000-fold. Longitudinal analysis showed a subacute response pattern for these cytokines, peaking between days 5 and 9 and declining thereafter (fig 1). In SAH, concentrations of IL-1β and IL-6 were significantly lower in plasma than in CSF, showing the intrathecal origin of these mediators. Plasma and CSF concentrations of IL-1β and IL-6 at day 5 were 2.21 (0.70) v5.78 (0.83) pg/ml (p<0.001) and 0.01 (0.04)v 9.15 (2.26) ng/ml (p<0.0001), respectively. By contrast, serum and CSF concentrations of TNF-α did not differ significantly (3.72 (0.73) v 3.62 (0.50) pg/ml; p=0.69). Samples of CSF obtained from extraventricular drainage (EVD) in 77% of the patients and by lumbar puncture in 23% did not differ in cytokine concentrations (data not shown).

CSF concentrations (mean values (SEM)) of IL-1β, TNF-α, and IL-6, in patients with SAH exhibiting cerebral blood flow velocities of <or ⩾210 cm/s. Reference cytokine concentrations detected in 20 control subjects were 0.00 (0.00) pg/ml (IL-1β), 0.0004 (0.0001) ng/ml (IL-6), and 0.18 (0.16) pg (TNF-α). * p<0.05.
ALTERATIONS OF CBFVS AND ASSOCIATION WITH SUBARACHNOID CYTOKINE SECRETION
Mean systolic CBFV subacutely increased during the study period of 11 days, peaking between days 7 and 11 when values reached a plateau (fig 2). Abnormalities were most pronounced in the middle cerebral arteries. Interestingly, changes in CBFVs paralleled those of CSF concentrations of inflammatory cytokines (figs 1 and 2). The response in the CSF, however, slightly preceded those of the haemodynamic abnormalities, peaking between days 5 and 9. We subdivided patients into two subpopulations with higher (⩾210 cm/s, defined as the cut off value to diagnose highly increased CBF cytokines17) or lower CBFVs (<210 cm/s). Development of CBFVs⩾210 cm/s (n=22) was associated with significantly increased CSF concentrations of IL-1β, IL-6, and TNF-α compared with presence of CBFV<210 cm/s (n=13, fig1).

Kinetics of changes in CBFV (mean (SEM)) in intracranial basal arteries as determined by transcranial Doppler sonography (n=20). Reference values as derived from our earlier readings in 50 normal volunteers were 94.5 (1.9) cm/s (middle cerebral artery, MCA), 76.4 (2.4) cm/s (anterior cerebral artery, ACA), 53.2 (1.6) cm/s (posterior cerebral artery, PCA), and 34.4 (1.7) cm/s (basilar artery, BA).17
CLINICAL OUTCOME AND ASSOCIATION WITH SUBARACHNOID CYTOKINE SECRETION
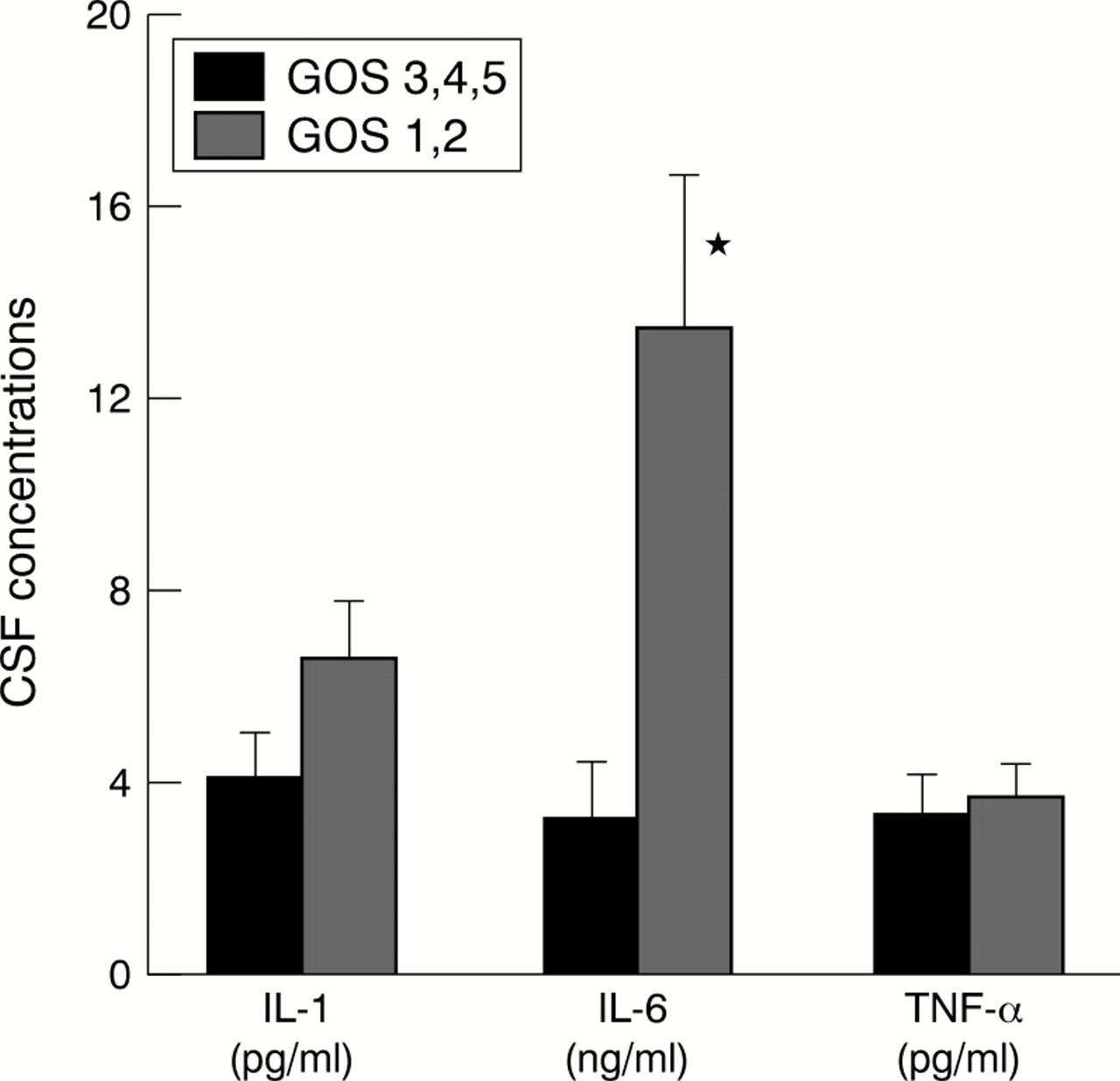
The GOS scores were 1 in 33%, 2 in 27%, 3 in 9%, 4 in 6%, and 5 in 24% of the patients. Concentrations of IL-6 at day 5 were significantly increased in patients with poor (GOS 1–2) compared with those with moderate or good (GOS 3–5) outcome, whereas concentrations of IL-1β and TNF-α exhibited a non-significant trend towards increased concentrations in the subpopulation with poor outcome (fig3). Follow up CT showed signs of newly developed cerebral ischaemic injury in 46% of the patients with SAH. These patients exhibited a non-significant trend towards increased CSF concentrations of IL-6 at day 5 (12.11 (3.51) ng/ml v 6.51 (2.25) ng/ml, p=0.08).
{kind=link}
{kind=link}
{kind=link}
CSF concentrations (mean (SEM)) of IL-1β, TNF-α, and IL-6 at day 5 in patients with better (GOS 3–5) or worse (GOS 1, 2) clinical outcome of SAH. * p<0.05.
Concentrations of IL-1β (r=0.87, NS), IL-6 (r= 0.19, NS), and TNF-α (r=−0.16, NS) did not correlate with Hunt and Hess scores. Hunt and Hess scores were not significantly different in patients with higher or lower CBFVs (3.42 (0.25) v 3.33 (0.36), p=0.87). As expected, the scores, however, correlated with GOS (r=−0.59, p<0.005). Interestingly, GOS scores were not significantly different in patients with lower or higher CBFVs (2.73 (0.52) v 2.43 (0.33), NS) in this study. Neither sex nor age were significantly associated with CSF cytokine concentrations. Thus, age did not correlate with concentrations of IL-1β (r=0.40, NS), IL-6 (r=0.23, NS), or TNF-α (r=0.14, NS). Similarly, concentrations of IL-1β (0.95 (1.45) v 5.03 (0.98) pg/ml, NS), IL-6 (11 763.85 (3134) v 8291.33 (2983) pg/ml, NS) or TNF-α (3.85 (0.87) v 3.48 (0.62) pg/ml, NS) were not significantly different in male or female patients. Moreover, age was not significantly increased in patients with higher CBFVs compared with those with lower CBFVs (57.33 (2.10)v 57.83 (5.04), NS) and mean CBFVs in the middle cerebral artery were not significantly different in male or femal patients (186.08 (16.31) v 325.00 (13.61) cm/s, NS). Finally, age did not correlate with GOS scores (r=−0.32, NS) and these scores were not significantly different in male or female patients (2.31 (0.46)v 2.80 (0.35), NS).
Discussion
Vasospasms and secondary cerebral ischaemia are the most important complications of SAH. This study showed that the release of IL-1β, IL-6, and TNF-α in the subarachnoidal space of patients with SAH is associated with development of increased CBFVs in basal cerebral arteries suggesting a pathophysiological role of excessive subarachnoidal inflammatory host response in haemodynamic complications after SAH.
Secretion of these inflammatory cytokines gradually increased, reaching peak concentrations at days 5–9. Peak concentrations were up to 10 000-fold increased, in the range previously detected in bacterial meningitis.18 Interestingly, the haemodynamic abnormalities in recorded basal cerebral arteries of patients with SAH were characterised by a similar subacute temporal profile, only slightly lagging behind the response of the inflammatory cytokines. Release of inflammatory cytokines in the subarachnoidal space was significantly increased in the subpopulation of patients with SAH with higher CBFVs. These findings are consistent with a recent report of higher IL-6 concentrations in five patients with clinical signs of vasospasms after SAH.16 Interestingly, CSF concentrations of IL-6 were significantly increased in patients with SAH with poor clinical outcome, further delineating the clinical relevance of intrathecal cytokine secretion in SAH.
Such pathophysiological importance of compartmentalised cytokine release for development of cerebrovascular complications after SAH could also explain the earlier observations of severe vasospasms in experimental subarachnoidal inflammation19 or in bacterial meningitis.18 Both conditions are characterised by massive cytokine release18 but by an obvious absence of erythrocytes or platelets that are generally considered as key cells in pathophysiology of vasospasms after SAH.
The triggers for the pronounced inflammatory host response in the subarachnoidal space of patients with SAH are unknown. One mechanism could be complement activation, a strong inflammatory stimulus, by osmotically induced disruption of erythrocytes. This is suggested by in vitro findings of a complement mediated haemolysis of erythrocytes in subarachnoid blood clot20 or by raised CSF concentrations of complement factors in SAH.21 22
Subarachnoidal release of inflammatory cytokines could contribute to cerebral vasospasms in several ways: Once released in the subarachnoidal space, these mediators (17–26 kD) could easily access the smooth muscle cells of contiguous basal arteries from their adventitial side as even much larger molecules (for example, horseradish peroxidase, MW 40 kD) pass from the cysterna magna through the vessel wall to the basal membrane within minutes.23This is possible because the surface of the pial cerebral arteries is, exceptionally, not confined by collagen or fibroblasts but is in direct contact with the nourishing CSF.23 At the smooth vessels, these mediators could directly cause vasospasms although the effects of inflammatory cytokines on vessel tone are still controversial. Whereas some of these mediators (for example, IL-1β) can act as vasodilators and increase endothelial permeability24-26 the cytokine IL-6 which exhibited the strongest response of all cytokines studied in this study, is strongly vasoconstrictive in vitro.16 Cytokines may also modulate vessel tone in an indirect manner—for example, by induction of synthesis of vasoconstrictiors such as ET-127 28 or by induction of adhesion molecule expression responsible for focal leucocyte recruitment.29 It has, however, to be noted that further factors may play a part in pathophysiology of cerebral artery narrowing after SAH and multiple therapeutic approaches to cerebrovascular complications after SAH are currently explored.2 30
Although we did not find different cytokine concentrations in CSF derived from EVD or by lumbar puncture, effects of the different origin of CSF on these measurements cannot be excluded.
In conclusion, although the clinical and laboratory correlations found cannot prove causal relations, this study supports the hypothesis that an overwhelming inflammatory host response in the subarachnoidal space of patients with SAH plays a central part in pathogenesis of vasospasms and subsequent cerebral ischaemia. As a therapeutic consequence of these findings, we speculate that early subarachnoidal administration of anti-inflammatory or anticytokine strategies could prevent haemodynamic complications after SAH.
Acknowledgments
We are grateful to Mrs M Garcia-Knapp for her secretarial assistance in the preparation of the manuscript.