Article Text

Abstract
Background and purpose The purpose of this study was to identify the risk factors predisposing to aneurysm rupture and to provide a reliable estimation for likelihood of rupture in unruptured intracranial aneurysms.
Methods The authors performed a nested case-control study of 290 aneurysms (123 unruptured aneurysms and 167 ruptured aneurysms) occurring during a prospective cohort study in 1493 consecutive patients with newly diagnosed intracranial aneurysm and were treated in a single institute between January 1995 and December 2006. Controls were matched for age, treatment group, number of lesion, sex, region and study period in which the incidence of ruptured and unruptured intracranial aneurysm was equivalently balanced. The authors assessed the predictive risk factors associated with aneurysmal rupture based on the clinical and angiographic findings reported in the patients' medical records.
Results Between January 1997 and December 2002, 167 patients with ruptured intracranial aneurysms were assigned to group 1, and 123 patients with unruptured intracranial aneurysms during the same period were assigned to group 2. Aspect ratio (OR 3.76), maximum diameter of neck (Nmax) ≤3 mm (OR 2.56) and family history of cerebrovascular disease (OR 5.63) were strongly correlated with aneurysm rupture (p<0.05).
Conclusions There are differences between the clinical and intrinsic characteristics of patients with unruptured and ruptured intracranial aneurysm. It will be helpful to make rational decisions regarding the optimal therapeutic strategy for unruptured intracranial aneurysm.
- Cerebrovascular disease
- stroke
Statistics from Altmetric.com
Many investigators have been attempting to identify the risk factors for intracranial aneurysm rupture for years.1–13 Although the International Study of Unruptured Intracranial Aneurysms (ISUIA) suggested that the majority of patients with incidentally detected intracranial aneurysm had a benign course,14 identification of the subset of patients who would develop problems if left untreated remains an important issue in the field of neurosurgery. For unruptured intracranial aneurysm found incidentally, the physician's primary concern usually depends on the patient's age, life expectancy, the size and location of the aneurysm and the patient's anxiety level. Thus, a more reliable estimation for a later rupture risk will be required for making rational decisions regarding the optimal therapeutic strategy for unruptured intracranial aneurysm.
Recent advances in novel technologies, such as digital subtraction angiography, magnetic resonance angiography and three-dimensional (3D) CT, have increased the likelihood of detecting an unruptured intracranial aneurysm and allowed for accurate measurement of the shape and size of the aneurysm, which are well-recognised risk factors for aneurysmal rupture. Other morphological indices include undulation index, aspect ratio, non-sphericity index, conicity parameter, bottleneck factor, ellipticity factor and so on.15–21 Several retrospective studies have attempted to reach a decisive conclusion regarding the predictive factors for ruptured intracranial aneurysm14–22; however, they failed to draw any firm conclusions because of the limitation of internal or external control in the study cohort. Furthermore, many authors only focused on evaluating the role of geometric indices associated with dynamic blood flow, regardless of the control of several clinical variables.14 16 18 23
Therefore, it is crucial to consider personal or familial factors and several modifiable factors including cigarette smoking and alcohol drinking as well as geometric indices when evaluating the risk factors of rupture. This report describes a nested case-control study that was conducted to determine the risk of rupture.
Methods
Study design and objectives
This nested case-control study was based on data from medical records of patients with a newly diagnosed intracranial aneurysm who were treated by surgical or endovascular techniques. The objective of this study was to identify the risk factors attributable to aneurysm rupture and to clarify the treatment indications for unruptured intracranial aneurysm.
Identification and recruitment of patients
We searched the database registry at the Department of Neurosurgery to identify patients with newly diagnosed intracranial aneurysm who had been treated at Samsung Medical Center, which is a tertiary referral hospital, between January 1995 and December 2006, and we identified 1493 consecutive patients with intracranial aneurysm. We screened these 1493 patients to identify the study group with an equivalent incidence of ruptured and unruptured intracranial aneurysm in an effort to minimise the selection bias (figure 1). Periodically, the incidence of ruptured intracranial aneurysm was higher than that of unruptured intracranial aneurysm until the early 1990s; however, the incidence of unruptured intracranial aneurysm has tremendously increased because of recent advances in diagnostic procedures. The base population for the case-control study comprised all those who had ruptured intracranial aneurysm and unruptured intracranial aneurysm between January 1997 to December 2002. By standard methodology for nested case-control studies, each case was randomly matched to control group. Matching variables were age, sex, treatment allocation, number of lesion, region and time period of qualifying event.
Annual trends in incidence of ruptured and unruptured intracranial aneurysms.
Patient eligibility
Patients were eligible for enrolment in this study if they had single intracranial aneurysm, including berry aneurysms in the vessels of the circle of Willis. Patients with traumatic or mycotic aneurysms were not eligible for this study. Additionally, patients with aneurysm that was less than 2 mm in maximum diameter, as measured using a standard measurement device, were excluded. By medical personnel's judgement, patients with unruptured intracranial aneurysm who would be observed without further treatment were excluded in this study. All patients were treated with direct aneurysmal clipping or coil embolisation at the time of diagnosis.
Angiographic assessment
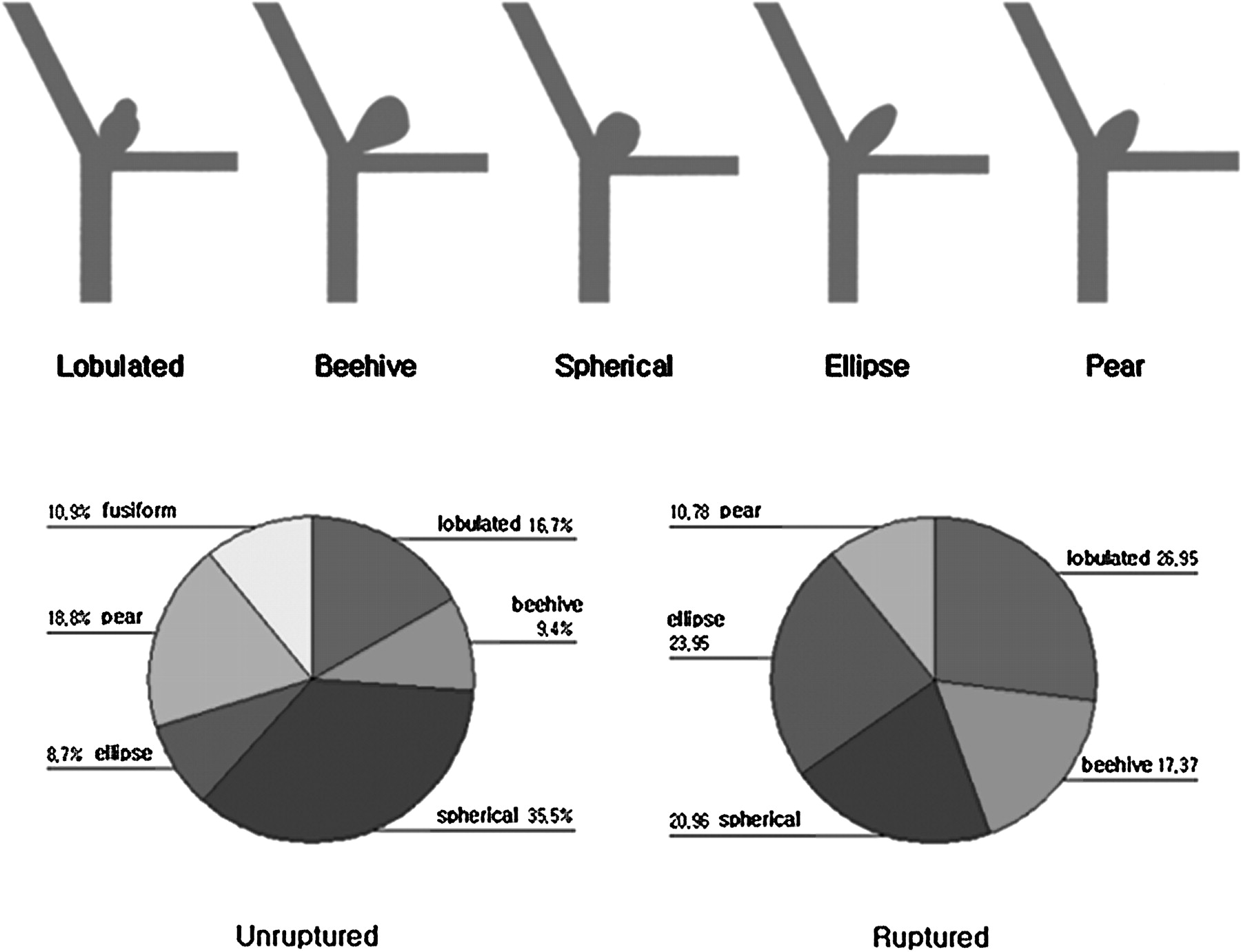
A total of 109 patients with aneurysms were assessed using two-dimensional digital subtraction angiography, and the remaining patients received three-dimensional digital subtraction angiography. The locations of the aneurysms were variable and included the anterior communicating artery (ACoA), anterior cerebral artery, with the exception of the ACoA, posterior communicating artery, internal carotid artery, with the exception of the posterior communicating artery, middle cerebral artery (MCA) and vertebrobasilar artery. Accurate estimation of the aneurysmal size and shape was possible using digital subtraction angiography. The aneurysms were divided into two groups according to shape: simple lobed (pear-shaped, spherical, ellipse, beehive) and bi-lobulated or tri-lobulated (figure 2). To measure the size of the aneurysm, the depths and necks of the aneurysms were measured to the nearest millimeter based on the best angiographic projections reflecting the bottleneck factor (Dmax/Nmax)19 and aspect ratio (AR=Depth/Nmax), which were calculated using the equation described by Ujiie et al.17 24

Morphological classification of saccular aneurysms and difference in shape distribution between unruptured and ruptured aneurysms.
Statistical analysis
Receiver operating characteristic (ROC) curve analyses were performed for the Dmax, Dneck, depth, aspect ratio and bottleneck factors in order to quantify the predictability of each index and identify the optimal threshold. Univariate and multivariate logistic regression analyses were performed to identify the predictors of rupture events. Rupture events were used as the dependent variable in this model. The multivariate logistic regression model included covariates found to have a marginal association with poor outcome in the univariate analysis (defined as p<0.20). The odds ratio (OR) and 95% CI were calculated. A p value of less than 0.05 was considered significant. In addition, several determinant factors were compared using a χ2 test to evaluate the distribution of the characteristics of the patients in the ruptured and unruptured intracranial aneurysm groups.
Results
In this nested case-control study, there were 167 cases with ruptured intracranial aneurysm and 123 controls with unruptured intracranial aneurysm. Table 1 summarizes Table 2 and 3 the baseline demographic data and shows risk factor data according to whether the subject became a case or not between January 1997 and December 2002. Out of the 290 patients, 190 (65.5%) were women and 100 (34.5%) were men. The mean age of the patients was 55.2 (12.2) years (range 22–83 years). A total of 122 (42.1%) patients had hypertension and 42 (14.5%) had a family history of hypertension or cerebrovascular disease. A history of cigarette smoking was found in 71 (23.9%) patients.
Patient characteristics with ruptured and unruptured aneurysms and their angiographic findings
Univariate logistic regression model for prediction of aneurysm rupture
Multivariate logistic regression model for prediction of aneurysm rupture
Distribution and size of aneurysms on ROC curves
The ACoA and MCA were the most common locations of aneurysm involvement. The shapes of the aneurysms were quite variable and included 68 bi-lobulated or tri-lobulated, 42 beehive-shaped, 84 spherical-shaped and 15 fusiform-shaped. The mean dome/neck ratio was 1.8 (0.8) and the mean height/neck ratio was 2.1 (1.1). ROC curves, which are representative of the predictive capability of a particular index, were generated for all indices. The sensitivity and specificity of all indices were considered in the ROC curve analysis. The shape of the ROC curve may be used to compare the predictive capabilities of different indices under the same condition. The ROC curves generated for the selection of size and shape indices are shown in figure 3.
Graph of receiver operating characteristic (ROC) curves for predictability of aneurysm rupture showing a comparison of each risk factor. The reference line means zero predictive capability. Bottleneck factor and aspect ratio have a positive predictability, whereas Nmax has a reverse predictability. Maximum diameter of dome and depth are quite close to the reference line.
Univariate and multivariate analyses
In an attempt to determine the risk factors predisposing to aneurysm rupture, 14 independent variables were analysed in the univariate logistic regression model. The independent variables analysed included family history (cerebrovascular disease, diabetes and hypertension) or personal history (cigarette smoking, alcohol drinking, hypertension and diabetes) and geometric parameters including maximum diameter of dome (Dmax), maximum diameter of neck (Nmax), depth, bottleneck factor (Dmax/Nmax), aspect ratio (depth/Nmax) (figure 4), aneurysm shape and lobulation (figure 1). Of these variables, five independent variables were significant predictors of aneurysm rupture. These included maximum diameter of neck (Nmax) ≤3 mm (OR 2.54, 95% CI 1.57 to 4.09, p<0.001), aspect ratio >1.6 (OR 4.45, 95% CI 2.69 to 7.37, p<0.001), bottleneck factor >1.7 (OR 2.12, 95% CI 1.29 to 3.47, p=003), personal history of hypertension (OR 1.94, 95% CI 1.18 to 3.19, p=0.009) and family history of cerebrovascular disease (OR 5.44, 95% CI 2.51 to 11.79, p<0.001). Other variables, such as location of aneurysm, diabetes, smoking or alcohol drinking, and Dmax, depth and family history of hypertension or diabetes, were not predictive by themselves (p>0.05). These variables, which were regarded as predictive factors of aneurysm rupture, were entered in the forward stepwise multivariate logistic regression model. Among these variables, the multivariable logistic regression model revealed that aspect ratio (OR 3.76), Nmax ≤3 mm (OR 2.56) and family history of cerebrovascular disease (OR 5.63) strongly affected the risk of aneurysm rupture (p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
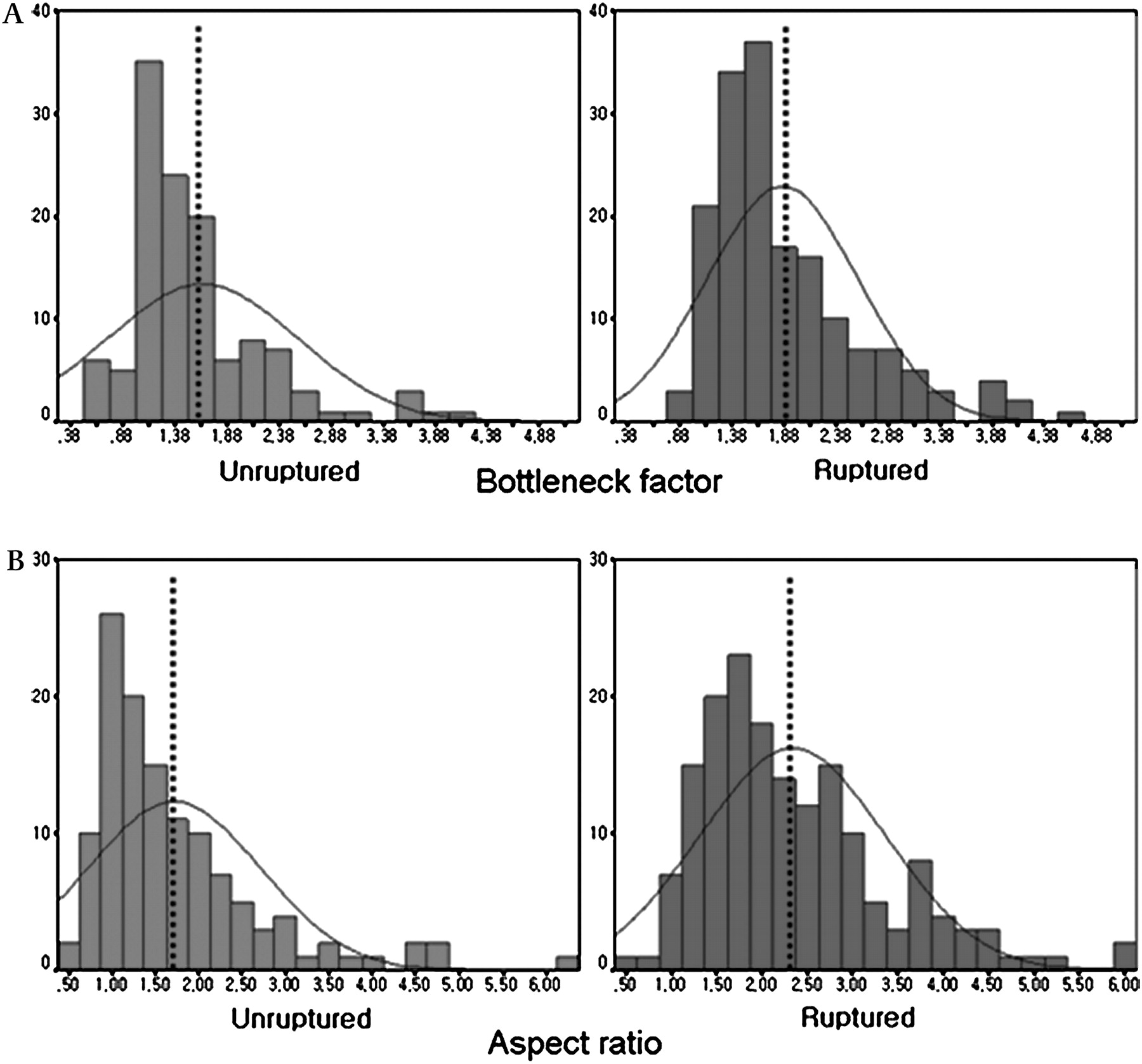
Difference in bottleneck factor (A) and aspect ratio (B) between unruptured and ruptured aneurysms.
Discussion
In the recent literature, several studies regarding unruptured intracranial aneurysm have focused on the risk factors of aneurysm rupture.14 16–19 23–26 These studies were performed based on the assumption that unruptured intracranial aneurysm was a precedent condition of ruptured intracranial aneurysm. However, previous conceptions about the natural history, particularly the risk of rupture of certain aneurysms, have been challenged.12 21 22 24–32 To date, multicentre prospective studies from the International Study of Unruptured Intracranial Aneurysms suggested that small unruptured intracranial aneurysm could be regarded as having little chance of rupture, and treatment should seldom be recommended for such small unruptured intracranial aneurysms.21 29 30 However, another interesting but contradictory fact is that aneurysms may develop more quickly than expected33 and rupture in the early period during their expansion phase, even though they are quite small in diameter.
It is generally known that the majority of unruptured intracranial aneurysm are located in the MCA and internal carotid artery, whereas the most frequent site of ruptured intracranial aneurysm is the AcoA.2 3 10 33 34 In addition to locational difference, we attempted to find other distinctive features on ruptured and unruptured aneurysms. This study has some differential characteristics, compared with previous other studies. Despite the limitation of retrospective analysis, this study concerned demographic features such as age distribution, sex, period of qualifying event, personal habit, family history and morphological characteristics of aneurysm. By stratifying age, sex and period of qualifying event, we could minimise the bias induced by exposure related to the hospitalisation. As a result, we found that patients with ruptured intracranial aneurysm had distinctive demographic characteristics, such as a history of hypertension and family history of cerebrovascular diseases.
This study had critical drawbacks because the control group with unruptured intracranial aneurysm included patients with aneurysms that would rupture at some point in the future. In other words, patients with very small (<2 mm) unruptured intracranial aneurysm during the same period were excluded. Consequently, the comparison of these two groups would be less distinct than the actual situation. Furthermore, there has been no available information regarding a decisive factor of aneurysm rupture. As another important limitation, the likelihood of size change during aneurysmal rupture could not be completely excluded in this study. Generally, a larger-sized aneurysm has a higher risk of aneurysmal rupture; however, after the rupture event of aneurysm, the size of aneurysm may be rather decreased because of deflating effect of balloon.
The interpretation of geometric indices, such as bottleneck factor or aspect ratio, remains controversial.15 16 19 23 24 33 35 Higher values of these indices in ruptured intracranial aneurysm indicate that they are rather elliptical, while unruptured intracranial aneurysm tend to be round in shape. Although there is a possibility that the shape of the aneurysms can also change after rupture, the exact phenomenon can be explained by a biophysical consequence, which is beyond the context of this cerebrovascular disease discussion. To assess the risks and benefits of treatment in a patient who is found to have an unruptured intracranial aneurysm, the treatment decision should be individualised, considering multiple factors including lifetime risk, treatment morbidities and the patient's own wishes. Therefore, we propose that further investigations are needed to define the correct concept of unruptured intracranial aneurysm because conclusive results from numerous data have not been established for the risk of rupture in incidental unruptured aneurysms.
In conclusion, we suggest that decisions regarding the optimal therapeutic strategy for unruptured intracranial aneurysm should be made based on the consideration of clinical and intrinsic characteristics of patients with unruptured intracranial aneurysm.
References
Footnotes
↵* Contributed equally to this work.
Competing interests None.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed.