Article Text

Abstract
Background and purpose: Cervical dissection is an important cause of stroke in the young. This paper presents a systematic review and a meta-analysis to assess the effectiveness of different treatment approaches: antithrombotic drugs, thrombolysis and stenting.
Methods: Medline and PubMed were searched from 1966 to 8 April 2007. Reference lists were reviewed. Separate searches were performed for treatment with anticoagulation and antiplatelet therapy during the acute phase (within 1 month of symptoms), thrombolysis and stenting.
Results: There were only sufficient data for meta-analysis for the comparison of antiplatelet versus anticoagulation therapy. No randomised trials were identified. 34 non-randomised studies included 762 patients. There was no significant difference in risk of death (antiplatelet 5/268 (1.8%), anticoagulation 9/494 (1.8%), p = 0.88); stroke (antiplatelet 5/268 (1.9%), anticoagulant 10/494 (2.0%), p = 0.66), or stroke and death. Four non-randomised studies of thrombolysis provided insufficient data for assessment of efficacy but complication rates were no greater than thrombolysis for other ischaemic stroke. Six studies included 96 patients undergoing stenting for both acute dissection and chronic complications, providing insufficient data for assessment of efficacy, although complication rates appeared similar to those published for carotid atherosclerosic stenosis.
Conclusions: There are no data to support the therapeutic superiority of anticoagulants over antiplatelet agents. Thrombolysis in dissection appears safe but more data on efficacy are required. Stenting is technically possible but there are no data to demonstrate efficacy. There is little evidence to support current treatment approaches in cervical dissection. Randomised controlled prospective trials, particularly assessing anticoagulation versus antiplatelet agents, are required.
Statistics from Altmetric.com
Cervical artery dissection is an important cause of stroke in younger individuals. Potential stroke mechanisms include both haemodynamic compromise secondary to stenosis and embolism. Evidence from brain imaging, angiography and detection of asymptomatic Doppler embolic signals1 suggest that embolism is the more important cause. Dissection may also result in local compressive symptoms with cranial nerve palsies and Horner’s syndrome. Natural history data indicate a high risk of early recurrent stroke, largely within the first month.2 3
This recurrent stroke risk has led to the use of antithrombotic treatment. Many physicians give anticoagulants assuming that this prevents embolism from thrombus at the dissection site more effectively than antiplatelet agents.4 Thrombolysis is increasingly used in patients with acute stroke due to dissection, in spite of concerns that it could result in extension of the intraluminal thrombus.5 Stents have also been used both acutely for arterial stenosis and more chronically to occlude dissecting aneurysms (DA), also referred to as pseudoaneurysms.6 7 However, natural history studies demonstrate that stenosis frequently resolves, and the risk of embolism from DA is low.8
Despite the frequency of cervical dissection, there are limited data on optimal treatment approaches. A Cochrane review in 2003,9 restricted to carotid dissection, found few high quality studies and no randomised prospective trials of antithrombotic therapy. A number of further studies have been published since then. We performed a systematic review to assess not only the effectiveness of anticoagulant versus antiplatelet agents but also the safety and efficacy of thrombolysis and stenting. We included data on both vertebral and carotid dissection.
METHODS
Separate searches and systematic reviews were performed for the three treatment areas. For each review we searched Medline and PubMed from 1966 to 8 April 2007.
Search terms used
Anticoagulation versus antiplatelet therapy
((Carotid artery OR vertebral artery OR cervical artery OR anterior circulation OR posterior circulation OR extra cranial carotid artery) AND dissection) AND (antiplatelet OR anticoagulant OR thrombolysis OR stenting).
Carotid artery dissection treatment.
Vertebral artery dissection treatment.
Cochrane review July 2003.9
Studies were included if they contained outcome data allowing comparison of patients on the two therapies. Only studies including acute treatment (within 1 month of symptom onset) were evaluated
Thrombolysis in cervical dissection
Thrombolysis (AND) vertebral (AND) artery (AND) dissection.
Thrombolysis (AND) carotid (AND) artery (AND) dissection.
Studies with both intra-arterial and intravenous thrombolysis treatment were included.
Stenting in cervical dissection
Stenting (AND) vertebral (AND) artery (AND) dissection
Stenting (AND) carotid (AND) artery (AND) dissection
Stenting (AND) cervical (AND) artery (AND) dissection
Both prospective and retrospective studies were included. Studies with less than four patients, those with primary intracranial or intracranial extension of extracranial dissection and those which did not clearly specify treatment groups were excluded. Abstracts were screened to identify studies meeting inclusion criteria. Reference lists of each full text publication were also hand searched. Articles meeting inclusion criteria were reviewed by two independent reviewers; for any divergent analysis consensus was achieved.
For comparison of antithrombotic therapies, the end points evaluated were death from any cause, ipsilateral stroke, ipsilateral transient ischaemic attack (TIA) and stroke, death and stroke. Patients who were treated with both antiplatelets and anticoagulants simultaneously were not included. For thrombolysis the end points evaluated were death from any cause, ipsilateral stroke, any stroke and death, intracerebral haemorrhage (ICH) and worsening of local signs. For stenting, end points evaluated were death from any cause, ipsilateral stroke, ipsilateral TIA and stroke, death, stroke and death, and re-stenosis rates.
Statistical analysis
There were sufficient data for meta-analysis only for the comparison of antiplatelet versus anticoagulation therapy. This was performed using Review Manager V.4.2 (http://www.cc-ims.net/RevMan). A risk difference with fixed effects model was used. A positive risk difference favours the anticoagulant group.
RESULTS
Anticoagulation versus antiplatelet therapy
The search resulted in 2944 citations: 186 abstracts were identified, and 34 met the inclusion criteria.1 2 10–41 Twenty-two abstracts related to carotid dissection, three to vertebral and nine to both.
These included 762 patients: 268 treated with antiplatelets and 494 with anticoagulation. Only one study was prospective (although not randomised)2 and included 23 patients on antiplatelet agents and 71 on anticoagulants. One large retrospective study4 of 459 patients was not included as it excluded patients in the first 1 month during the initial high risk period.
There were 14 deaths, 5/268 (1.8%) in the antiplatelet group and 9/494 (1.8%) in the anticoagulant group. The risk difference was not significant (0% (−4% to 5%); p = 0.88). There were 15 strokes (four ipsilateral, others not mentioned), 5/268 (1.9%) in the antiplatelet group and 10/494 (2.0%) in the anticoagulant group. The risk difference was not significant (−1% (−6% to 4%); p = 0.66). Forrest plots are shown in fig 1.

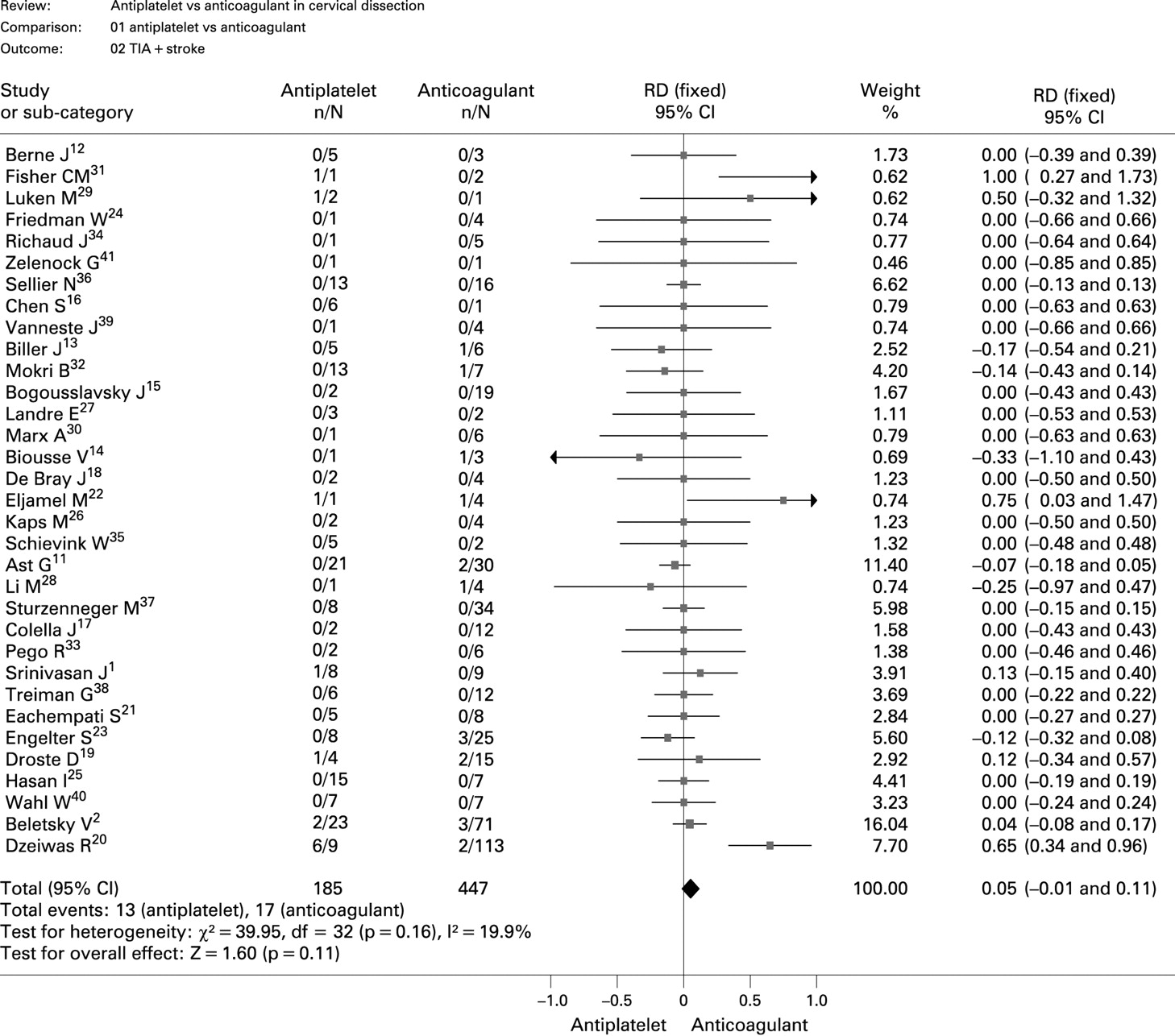
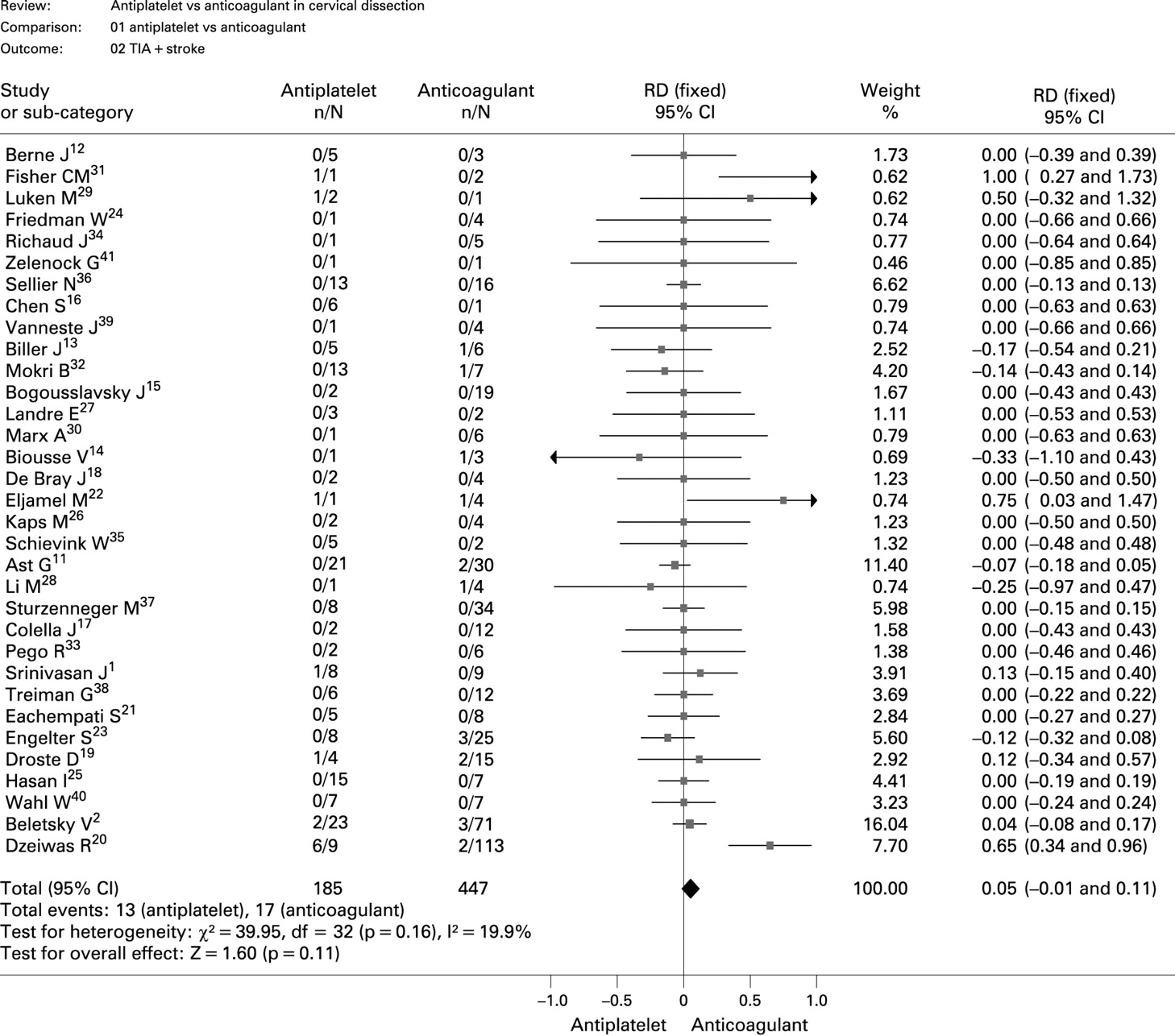
For analysis of the combined end point of TIA and stroke, one study3 was omitted as it included data on stroke alone; 13/185 (7.0%) in the antiplatelet group and 17/447 (3.8%) in the anticoagulant group suffered TIA or stroke. This difference was not significant (5% (−1% to 11%); p = 0.11). Forrest plots are shown in fig 2.
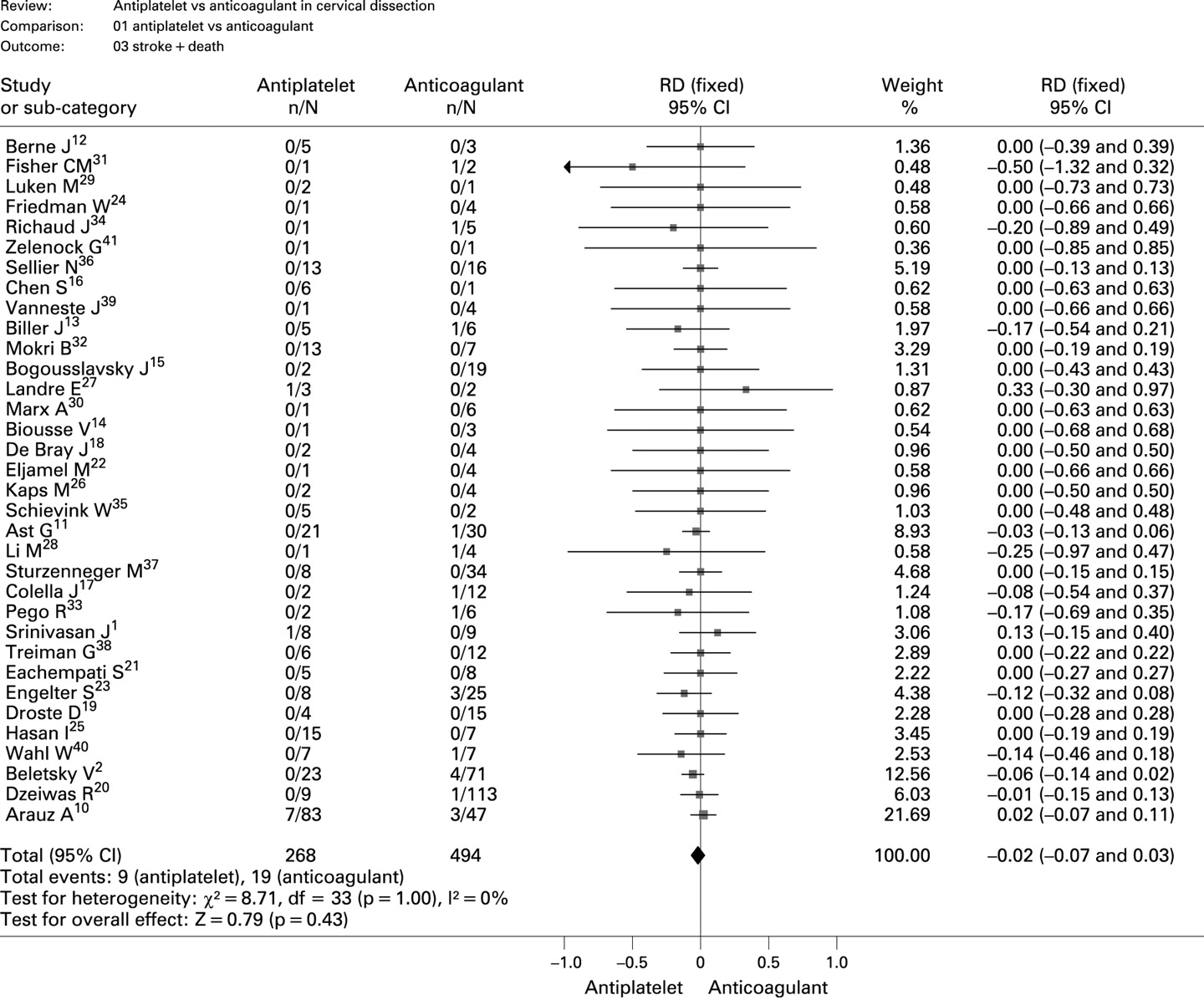
Nine of 268 (3.4%) patients in the antiplatelet group and 19/494 (3.8%) in the anticoagulant group suffered stroke or death. The difference was not significant (−2% (−7% to 3%); p = 0.43). Forrest plots are shown in fig 3.
{kind=link}
{kind=link}
{kind=link}
Thrombolysis in cervical artery dissection
There were no randomised controlled trials and all four identified studies were retrospective.4 42–44 These included 59 patients, all with carotid dissections. Seven were treated with intra-arterial thrombolysis, all urokinase,42 and 52 with intravenous thrombolysis (all tissue plasminogen activator (tPA)). In all but one study,44 almost all patients were treated within 3 h of stroke onset. One patient developed hemiplegia and aphasia 40 min after the start of tPA infusion caused by recurrent cerebral infarction and died 3 days later.4 There was one symptomatic ICH. All but one study performed CT imaging the day after treatment, and in the 46 patients scanned there were no additional ICHs. No worsening of local signs was reported. Four patients died, one due to stroke during thrombolysis as described above and the others for reasons unrelated to thrombolysis.
The complication rate was compared with that from the SITS-MOST45 registry in 6483 patients receiving intravenous thrombolysis within 3 h of stroke onset. The rate of symptomatic ICH, and any ICH, in SITS-MOST was 1.7% and 7.9%, respectively, compared with 1.9% and 1.9%, respectively, in the dissection cases.
Angioplasty and stenting in cervical artery dissection
The search resulted in 145 citations of which six met the selection criteria.5 6 46–49 Hand search identified two further studies.50 51 All studies were non-randomised, retrospective and included 97 procedures in 93 patients. Stenting was performed for a variety of indications, including traumatic and non-traumatic dissection, acutely for tight stenosis or later for DA. There was a high technical success rate with only five (5.2%) technical failures, most often because of vessel tortuosity and difficulty accessing the lesion, and in one case following creation of an intimal flap. There were few perioperative complications; three TIAs (3.1%) and no strokes. Excluding perioperative events during the first 30 days of follow-up there was one death due to myocardial infarction but no recurrent strokes. Follow-up after 30 days was of variable duration, and there were three TIAs and two contralateral strokes but no ipsilateral strokes. Angiographic results were good with resolution of stenosis, where present, in almost all cases, and only two re-stenoses on follow-up imaging.
DISCUSSION
Our systematic review showed no evidence of a therapeutic benefit favouring either antiplatelet or anticoagulant treatment in preventing stroke, TIA or death in cervical dissection. This included data from a number of studies published since the 2003 Cochrane review9 and included both carotid and vertebral dissection, resulting in twice the number of patients in the Cochrane review.
Anticoagulant therapy is often preferred to antiplatelet agents on the assumption that it better prevents recurrent embolism from thrombus at the site of dissection. However, it has potential complications. It could theoretically result in the expansion of the local haematoma resulting in worsening of local signs and, more importantly, increased stenosis and haemodynamic compromise. Delayed occlusion with haemodynamic compromise was reported in five of 20 carotid dissection cases treated with heparin, one of whom developed a watershed infarct, and the risk may increase with intensity of anticoagulation.52 We found no evidence of increased complications or death in patients treated with anticoagulation, but also no evidence of any reduction in stroke risk.
Power calculations have suggested that a sample size of at least 1400 patients in each treatment arm would be required in order to detect a 5% difference in the proportion of patients dead or disabled from 24% to 19% with a power of 90%.9 The risk of recurrent stroke following cervical dissection occurs primarily in the first month, and is probably highest in the first week,2 3 10 so any therapeutic trial would need to rapidly identify and randomise patients in this acute stage. Our systematic review indicates that many ischaemic events occurred prior to recruitment to the studies and even within the first few hours. Whether patient identification and initiation of treatment, and establishment of treatment efficacy, can be obtained within this short time remains to be determined. A recent review of this subject came to similar conclusions.53 The feasibility phase of one such trial, CADISS (Cervical Artery Dissection in Stroke Study), has now started and is randomising patients within 1 week of symptom onset to either heparin followed by warfarin or antiplatelet therapy (www.dissection.co.uk).
Thrombolysis is a standard treatment for patients with acute ischaemic stroke. However, there are potential hazards in dissection, including extension of the intramural haematoma, dislocation of luminal thrombus leading to thromboembolism, subarachnoid haemorrhage and even DA formation. We identified only four studies, which included 59 patients. All were retrospective and uncontrolled and therefore open to significant selection bias, providing insufficient data to draw conclusions on efficacy. However, some information can be obtained on safety and potential complications. The complication rate appeared low, and was at or below the level reported in the recent SITS-MOST registry. In particular, no worsening of local signs, which could occur following extension of local haematoma, was reported. One patient developed recurrent stroke during thrombolysis; the authors postulated that this was due to dislodgement of thrombus at the site of dissection secondary to thrombolysis.4 There were no other deaths related to thrombolytic therapy. This suggests that thrombolysis is likely to be relatively safe in patients with carotid dissection, but further data are required.
Studies of stenting in dissection were all retrospective and non-randomised. Stents were inserted for a number of different indications; in the acute setting to open a stenosis or seal an intimal flap, and chronically to occlude a DA. Many studies included stents inserted for a combination of indications, making results difficult to interpret. A relatively high technical success level was reported with a failure rate of only 5% and there were few perioperative complications. However, the efficacy of stenting, and whether it is even necessary in many cases, is uncertain. Many stenotic lesions following dissection spontaneously recanalise. Furthermore, many stents were inserted for DAs on the assumption that these are associated with increased risk of recurrent stroke due to embolisation from the site of aneurysm. Recent studies have suggested that the risk of recurrent embolisation from DAs is low.8 Therefore, before the more widespread use of stenting in dissection, its efficacy needs to be evaluated in randomised trials which should be planned to stratify stent insertion according to indication, separating treatment of acute lesions from chronic DAs.
In conclusion this systematic review in over 700 patients showed no evidence of a difference in efficacy or complications between antiplatelet and anticoagulant therapy. However, there were no data from randomised trials and much of the data were of poor quality, making it impossible to draw definite conclusions on efficacy. Our systematic review indicates that at present there is insufficient evidence to comment on the roles of thrombolysis and stenting in dissection.
REFERENCES
Footnotes
Funding: This study was funded by the Stroke Association.
Competing interests: None.