Article Text

Abstract
Background Data on the implementation of prehospital large vessel occlusion (LVO) scales to identify and triage patients with acute ischemic stroke (AIS) in the field are limited, with the majority of studies occurring outside the USA.
Objective To report our long-term experience of a US countywide emergency medical services (EMS) acute stroke triage protocol using the Rapid Arterial oCclusion Evaluation (RACE) score.
Methods Our prospective database was used to identify all consecutive patients triaged within Lucas County, Ohio by the EMS with (1) a RACE score ≥5, taken directly to an endovascular capable center (ECC) as RACE-alerts (RA) and (2) a RACE score <5, taken to the nearest hospital as stroke-alerts (SA). Baseline demographics, RACE score, time metrics, final diagnosis, treatments, and clinical and angiographic outcomes were captured. The sensitivity and specificity for patients with a RACE score ≥5 with LVO, eligible for mechanical thrombectomy (MT), were calculated.
Results Between July 2015 and June 2018, 492 RA and 1147 SA were triaged within our five-hospital network. Of the RA, 37% had AIS secondary to LVOs. Of the 492 RA and 1147 SA, 125 (25.4%) and 38 (3.3%), respectively, underwent MT (OR=9.9; 95% CI 6.8 to 14.6; p<0.0001). Median times from onset-to-ECC arrival (74 vs 167 min, p=0.03) and dispatch-to-ECC arrival (31 vs 46 min, p=0.0002) were shorter in the RA-MT than in the SA-MT cohort. A RACE cut-off point ≥5 showed a sensitivity and specificity of 0.77 and 0.75 for detection of patients with LVO eligible for MT, respectively.
Conclusions We have demonstrated the long-term feasibility of a countywide EMS-based prehospital triage protocol using the RACE Scale within our hospital network.
- stroke
- intervention
- thrombectomy
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Mechanical thrombectomy (MT) decreases disability in patients with acute ischemic stroke (AIS) with large vessel occlusion (LVO) when performed within 24 hours from symptoms onset.1–7 Significant delays in onset-to-reperfusion times have been reported in interhospital transfer of patients with AIS,8 9 with one in three patients becoming ineligible for MT owing to unfavorable brain CT changes following transfer.10 Optimal prehospital triage presents a major challenge for regional systems of care, especially in areas where multiple stroke centers of variable capabilities exist. As recent MT trials have highlighted the importance of timely treatment in improving patient outcomes,11 12 efforts to identify patients with AIS with LVO at the prehospital level are critical in order to expedite transport to endovascular capable centers (ECCs).
Prehospital stroke severity scales may aid in identifying patients with AIS with suspected LVOs13; however, there is a paucity of data on the long-term implementation of prehospital LVO scales in a ’real-world' setting.14 15 The Rapid Arterial oCclusion Evaluation (RACE) Scale is one of the few prehospital scales that have been prospectively validated in the field, and has been recently revalidated in a large cohort in Catalonia.16 17 To date, there have been limited, real-world, prospective US experiences of emergency medical services (EMS) triage of patients with AIS using prehospital LVO scales.18 19
Here, we report our long-term experience of a US county-based EMS AIS triage protocol using the prehospital RACE Scale.
Methods
Setting
Lucas County, located in northwestern Ohio, is a 596 square mile area with an estimated population of 430 887 (figure 1A). It is served by one EMS agency and eight hospitals, five of which comprise our hospital network: two ECCs (one comprehensive stroke center and one primary stroke center with interventional capabilities) and three PSCs without interventional capabilities. All county zip codes are within a 30 min drive from an ECC.

RACE study setting and population. (A) Map of Lucas County and hospitals. Network includes five hospitals, two endovascular capable centers (ECCs) and three primary stroke centers (PSCs). Non-network hospitals include one ECC, one PSC, and one free-standing emergency department (ED). (B) Study flow chart. The pie chart depicts the final diagnoses of the RACE population. AIS, acute ischemic stroke; ICH, intracerebral hemorrhage; LVO, large vessel occlusion; MT, mechanical thrombectomy; TIA, transient ischemic attack.
RACE protocol
Previously, we reported the initial implementation of a county-based bypass protocol using the EMS administered RACE Scale,18 the details of which are included in the online supplementary methods. The RACE-alert protocol is outlined in online supplemental figure I. Patients testing positive for suspected stroke on the Cincinnati Stroke Scale are subsequently assessed by EMS using the RACE Scale (scored 0–9). Patients with a RACE score ≥5 and last seen normal within 24 hours or time of onset unknown are triaged as RACE-alerts (RA) and sent to the nearest ECC. Patients with a RACE score <5 are triaged as stroke-alerts (SA) and transported to the nearest hospital. Once a RACE-alert is declared, the ECC emergency department protocol is activated (see online supplementary methods). Stroke-alert patients received CT angiography (CTA) imaging if baseline National Institutes of Health Stroke Scale (NIHSS) score was >4. All RA received CT and CTA, unless cancelled by the ER physician. Our MT selection criteria did not change during the study period. Patients who were last seen normal between 6 and 24 hours underwent CT perfusion imaging.
Supplemental material
EMS training
All 435 currently active Lucas County EMS personnel participated in a 4-hour training module on the stroke and the RACE Scale. Training is required for new EMS personnel, who thereafter have a yearly refresher course. All EMS personnel are advanced life support certified and licensed as paramedics by the state of Ohio.
Data collection
Data were recorded prospectively in an institutional review board approved observational RACE Registry. Data included baseline characteristics, time metrics, treatments, final diagnosis, and angiographic and clinical outcomes. Ninety-day clinical outcomes were assessed using the modified Rankin Scale (mRS) score. Favorable clinical outcome was defined as a mRS score <2.
Statistical analysis
Statistical analysis was performed using software ‘R: a language and environment for statistical computing; EZR version 1.32’. Overall RACE population characteristics are presented. Baseline characteristics, time metrics, and outcomes were compared between the RA and SA MT cohorts. Mann-Whitney or Student t-tests were used for comparison of continuous variables and Fisher exact tests for categorical variables. Variables with a p value of <0.10 and clinically relevant factors on univariate analysis were entered into a multivariate stepwise logistic regression model to determine predictors of clinical outcome in the MT cohort. The predictive values of RACE ≥5 for patients with LVO eligible for MT were calculated.
Results
Overall RACE cohort
Between July 2015 and June 2018, 2635 consecutive patients were evaluated by Lucas County EMS using the RACE Scale. Of these, 686 RA were transferred to the nearest ECC and 1949 SA were transferred to the closest hospital (figure 1B). Of the SAs, 62% and 38% were transported to an ECC or non-ECC, respectively. A total of 1147 SA and 492 RA were admitted to our five-hospital network and included in this analysis. During the study period, there was 100% compliance with RACE score documentation by the EMS.
RACE-alerts
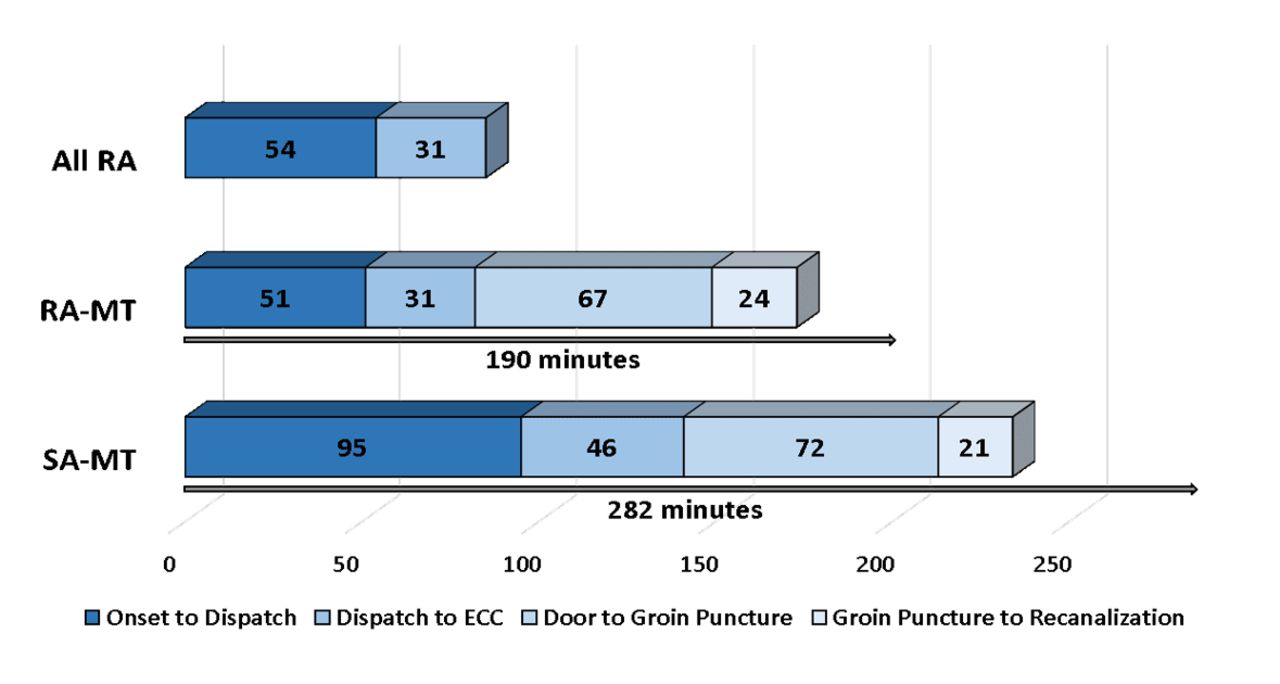
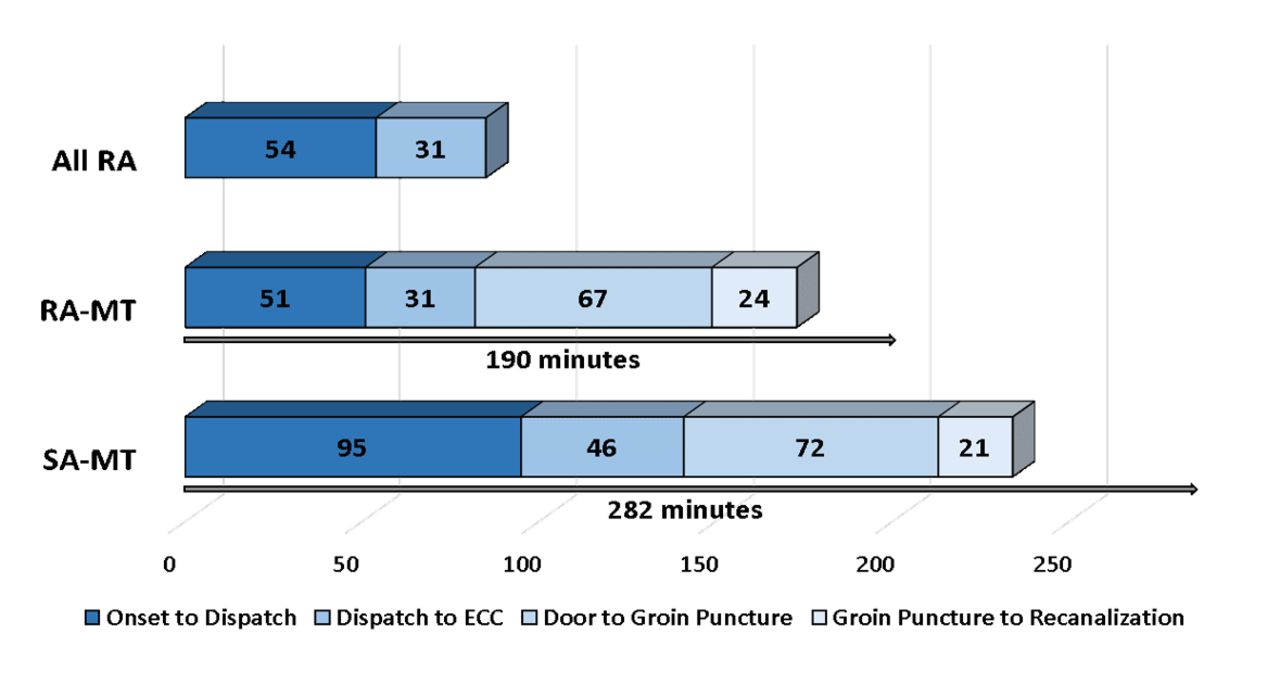
The RA population was consistent across the study period (online supplemental table 1). Of the 492 RA, 27.9% were stroke mimics, 13.8% had intracerebral hemorrhage (ICH), 6.5% a transient ischemic attack (TIA), and 51.8% ischemic stroke (figure 1B, table 1). The median RACE score was 7 across most diagnoses, with the exception of ischemic stroke without LVO. The median time intervals for RAs from dispatch-to-ECC arrival and onset-to-arrival was 31 (IQR 26–36) and 85 (IQR 46–300) min, respectively (figure 2). Discharge to a neuro-intensive care unit (ICU) occurred in 72% of RAs, of which 100% of patients with AIS with LVO and ICH required ICU admission.
Characteristics of the RACE-alert population.
{kind=link}
{kind=link}
Time metrics (median) of overall RACE and RACE-alert and stroke-alert mechanical thrombectomy cohorts. Grey arrows indicate median time from onset to recanalization. ECC, endovascular capable center; MT, mechganical thrombectomy; RA, RACE-alerts; SA, stroke-alerts.
Ischemic stroke
Of the 255 RAs with AIS, 182 (71.4%) had LVOs on CTA. Median baseline NIHSS score was higher in patients with AIS with LVO than in those with TIA and stroke mimics (table 1). Intravenous tissue plasminogen activator was administered in 42.4% of patients with AIS. Median times from door-to-CT imaging and door-to-needle were 10 (IQR 7–15) and 33 (IQR 24–47) min in the AIS cohort, respectively.
RACE and MT
Of the 492 RA and 1147 SA, 125 (25.4%) and 38 (3.3%) underwent MT (OR=9.9; 95% CI 6.8 to 14.6; p=<0.0001), respectively. Baseline characteristics of the RA-MT and SA-MT cohorts were balanced with the exception of median baseline NIHSS score, which was significantly higher in the RA-MT group (16 vs 9, p=<0.0001) (table 2). A trend towards more IV tissue plasminogen activator (tPA) administration was observed (50.4% vs 34.2%, p=0.10) in the RA-MT group. The majority of occlusions were middle cerebral artery-M1 in both groups; however, more basilar occlusions were present in the SA-MT cohort (10.5% vs 2.4%, p=0.054).
Time metrics
Intervals for median time from onset-to-ECC arrival (74 vs 167 min, p=0.03) and dispatch-to-ECC arrival (31 vs 46 min, p=0.0002) were shorter in the RA-MT than the SA-MT cohorts (figure 2, table 2). Median ECC door-to-groin puncture times were similar between the groups (72 vs 67 min, p=0.21).
Characteristics of the RACE alert (RACE ≥5) versus stroke alert (RACE <5) mechanical thrombectomy cohorts
Angiographic and clinical outcomes
No difference was seen in the rates of successful revascularization between the RA-MT and SA-MT cohorts (84.0 vs 78.9%, p=0.47) (Table 2). Ninety-day favorable functional outcome was numerically higher in the SA-MT group, but did not reach statistical significance (63.2% vs 46.4%, p=0.10). The rate of mortality was similar between the cohorts (15.8% vs 24.8%, p=0.37).
After adjusting for baseline NIHSS score, baseline Alberta Stroke Program Early CT Score (ASPECTS), age (continuous), and time from door-to-groin puncture, independent predictors of good clinical outcome were baseline NIHSS score (OR=0.92, CI 0.86 to 0.98; p=0.008) and age (OR 0.96, 95% CI 0.93 to 0.98; p=0.007) in the MT cohort.
Predictive value of RACE ≥5 for patients with LVO eligible for MT
A RACE cut-off point of ≥5 demonstrated a sensitivity, specificity, negative predictive value, and positive predictive value of 0.77, 0.75, 0.97, 0.25, respectively, for patients with LVO eligible for MT. The accuracy of this cut-off point was 75.3% (95% CI 73.1% to 77.4%).
Discussion
Several stroke LVO scales have been validated1 14–16 20 21; however, few have been prospectively applied by the EMS in a prehospital setting within the USA.18 19 Our 3-year experience demonstrates the long-term feasibility of implementing a countywide EMS-based prehospital AIS triage protocol using the RACE Scale. Implementation of the RA protocol in our five network-hospital system demonstrated that ~1 in 3 RA patients will harbor LVOs, and ~1 in 4 RA patients and ~1 in 30 SA patients will be eligible for MT. Importantly, in our population, a RACE cut-off point ≥5 was able to identify 77% of patients with AIS who were eligible for MT.
The population of patients identified with a RACE cut-off point of ≥5 remained consistent across our 3-year experience, with 51.8% of patients presenting with AIS, 6.5% with a TIA, 13.8% with ICH, and 27.9% as stroke mimics, which is similar to the results of our initial pilot study (52.3% AIS, 6.4% TIA, 11% ICH, 31% stroke mimics).18 In a recent revalidation study of the RACE Scale, Carrera et al reported that the majority of false-positive patients in their RACE ≥5 cohort had ICH (29%) followed by AIS with no LVO (25%), TIA (3%), and stroke mimics (8%).17 Although the proportion of false-positive results in our study differed from those found in the revalidation study (lower ICH and higher stroke mimics rates), the proportion of RACE ≥5 patients with AIS with LVOs was nearly identical between the studies (37% vs 35%). These results differ from a recent prehospital RACE study in Texas, where the authors report a lower LVO rate of 28.8% in their RACE ≥5 patients.19 The lower rate found by Dickson et al in their population might be attributed to the lack of imaging data to confirm LVO and location status. Importantly, similar to the results of Carrera et al, our study demonstrated that a RACE cut-off point of ≥5 detected 77% (versus 75%) of patients with AIS LVO eligible for MT. These findings suggest that RACE, in addition to detecting LVOs in a prehospital population of patients with suspected stroke, may also be beneficial in identifying patients who are eligible for MT. Interestingly, there was a trend towards a lower rate of detection of basilar artery syndromes in our cohort; this may be due to focus on laterality in the RACE score which may not be a reliable finding in posterior circulation strokes.
Introducing and monitoring the RA protocol on a countywide-level required a high level of collaboration between the local stroke providers and EMS leadership, but this coordination of efforts has led to the ‘RACE halo effect’, with streamlined efficiencies at the prehospital level and within the ECCs as well. As part of the RA protocol, we implemented ER protocols at our two ECCs, which included EMS prearrival notification of RA to ECC, preregistration in the electronic medical record system, and expedited assessment and CT/CTA imaging. Since our initial implementation of the RA protocol, we have been able to consistently increase our rates of IV tPA administration and reduce our median door-to needle and groin puncture times.
Implementation of the RACE Scale in our county was feasible owing to the coordination of the Lucas County EMS leadership, which formed a partnership with vascular neurologists to design, implement, and monitor the RACE training of EMS personnel. As funding and training time can be a limiting factor, countywide or regional application of a prehospital stroke scale may not be a realistic goal for some geographic areas with restricted resources. Recent data from Carrera et al showed that patients with RACE ≥5 who arrive first at an outside hospital are 2.5 times less likely to receive MT and are treated 2 hours later than similar patients who present directly to an ECC. These data support the need for further research into the benefit of direct transfer to an ECC, which is under investigation in the ongoing, “Direct Transfer to an Endovascular Center Compared to Transfer to the Closest Stroke Center in Acute Stroke Patients with Suspected Large Vessel Occlusion’ (RACECAT) trial (NCT02795962).
Future directions
With the success of our countywide RACE triage protocol, we recently modified and expanded our protocol to rural areas in northwest Ohio. The Triage of Acute Strokes Using a RACE Protocol in Urban and Rural Communities (TRACER) Registry will include eight rural hospitals and will enable study of the generalizability of our model to rural areas that have less access to ECCs (online supplemental figure II).
Limitations
This study has several limitations. As all five hospitals in our network are within 20 min of each other, the generalizability of our approach to larger geographic areas or areas with multiple EMS providers may vary. Our unified EMS structure includes only paramedics who are licensed by the state of Ohio and employed full time by the county. All paramedics undergo yearly training in stroke and RACE Scale administration. The accuracy of stroke severity-based triage may not be generalizable to EMS agencies that rely on volunteers or may not have similar rigorous training and feedback processes. As our EMS personnel are trained only on the RACE scale, we were unable to prospectively compare other prehospital LVO scales, such as vision, aphasia, and neglect (VAN) and the Los Angeles Motor Scale (LAMS), in our current study.15 22 Physician involvement via tele-stroke technology may reduce the number of stroke mimics, which accounted for 27.8% in our RACE cohort. We were able to modestly reduce our stroke mimic rate from 31% in our initial 6- months to 27.9% by further instructing EMS personnel not to triage patients with documented seizure as RAs. As our region is served by another hospital system, it is possible that selection bias may have occurred. The SAs in our five-hospital network did not all receive CTA imaging and, therefore, it was not possible to discern the true population of LVO in this population.
Conclusions
We have demonstrated the long-term feasibility of implementing a countywide EMS-based prehospital AIS triage protocol using the RACE Scale. Large, prospective studies are needed to compare LVO scales for prehospital triage of AIS.
References
Footnotes
Contributors All authors participated in the study design, collection of data, and/or drafting and editing of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement All data are contained in the manuscript.
Patient consent for publication Not required.