Article Text

Abstract
Background The Pipeline Vantage Embolization Device with Shield Technology is a next generation flow diverter developed to improve aneurysm occlusion and implant endothelialization in addition to lowering thrombogenicity. We report here the in vivo biocompatibility and in vitro hemocompatibility performance of the Pipeline Vantage Embolization Device with Shield Technology (Vantage) compared with the Pipeline Flex Embolization Device (Flex).
Methods Biocompatibility (via histology), aneurysm occlusion and vessel patency (via angiography), and endothelial coverage (via scanning electron microscopy (SEM)) for the Vantage and Flex devices were assessed in the rabbit elastase aneurysm model at 90 days (n=29) and 180 days (n=27). In vitro thrombogenicity for Flex and Vantage (n=16) was assessed using a human blood flow loop model at low heparin concentration (0.6 U/mL) with thrombin generation, platelet activation and thrombus visualization as outputs.
Results Raymond Roy Occlusion Classification grade 1 was higher for Vantage (61%) compared with Flex (46%), but was not statistically significant (p>0.05). All branch vessels were patent. Histological measures for both devices were similar (p>0.05). Endothelial coverage of the implant was significantly better for Vantage compared with Flex (p<0.05). In vitro measurements of thrombin generation (thrombin-antithrombin complex (µg/mL): Vantage 0.49±0.45; Flex 10.57±9.84) and platelet activation (β-thromboglobulin (IU/µl): Vantage 0.41±0.19; Flex 4.14±2.38) were both statistically lower (p<0.05) for Vantage compared with Flex. High resolution microscopy showed less accumulation of thrombus on Vantage as compared with Flex.
Conclusion Vantage improved aneurysm occlusion and implant endothelialization and had significantly lower thrombogenicity as compared with Flex, while preserving the biocompatibility safety profile of Flex.
- aneurysm
- flow diverter
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Flow diversion has emerged as a disruptive technology for the treatment of intracranial aneurysms.1 Several flow diverters have recently been approved and clinical data2 support improved progressive aneurysm occlusion with low recurrence rates compared with traditional coiling and stent- assisted coiling. However, thromboembolic events due to the large metal coverage area are also documented and are not entirely mitigated, even with antiplatelet therapy.3 The ideal characteristics of a flow diverter include optimal pore density and good wall apposition to achieve flow stagnation in the aneurysm,4 lower overall implant thickness profile to improve endothelial coverage (scaffolding of the parent vessel and aneurysm neck), and low thrombogenic profile to mitigate thrombogenic complications, among other attributes.5 6 The Pipeline Embolization Device has demonstrated progressive and complete aneurysm occlusion in several large clinical trials including Pipeline for Uncoilable or Failed Aneurysms (PUFs)7 8 and more recently the Prospective Study on Embolization of Intracranial Aneurysms with the Pipeline Device (PREMIER).9 Phosphorylcholine surface modification of the Pipeline device resulted in similar clinical performance in aneurysm occlusion10–12 while improving the safety profile by reducing material thrombogenicity of the implant.10 13 Shield Technology has been shown to reduce thrombus formation in vitro,14 15 ex vivo,16 and in vivo,17 and promotes early neointimal growth and endothelial coverage in vivo.18
The Pipeline Vantage Embolization Device with Shield Technology (Vantage, CE marked) consists of either 48 or 64 cobalt chromium wires with platinum on the inside of each wire (drawn filled tube configuration). The wires are smaller in diameter than Pipeline Flex, which provides a lower overall thickness profile of the implant that would potentially favor endothelial growth. Additionally, the Vantage implant leverages phosphorylcholine surface treatment, which results in a lower thrombogenic profile to the device and potentially encourages early neointimal coverage. The Vantage implant has a higher pore density (64 wire implants) than Flex in the same diameter range (>4 mm labeled implant diameter), but comparable metal coverage. This feature may potentially improve aneurysm occlusion rates due to reduced inflow and improved flow stagnation in the aneurysm.
The rabbit elastase aneurysm model is a well-established technique for assessing the biocompatibility and aneurysm occlusion of flow diversion devices.19 20 Aneurysm occlusion can be assessed angiographically and vascular safety can be assessed histologically for foreign body response (inflammation, thrombus formation, intimal damage, among other metrics) and healing (endothelial coverage). Additionally, the rabbit aorta has smaller diameter branch vessels that can still be visualized angiographically.21 22 One concern with flow diverters is the occlusion of intracranial perforator vessels. Overlapping devices deployed in the rabbit aorta across the ostia of such vessels could therefore provide an assessment of intermediate-large diameter perforator vessel occlusion.
In vitro closed loop human blood pulsatile flow models have been used to measure thrombogenicity of intraluminal devices such as flow diverters.15 23 Within this model, the combined effects of material and flow-induced thrombogenicity can be assessed at physiological intracranial flow rates. Thrombin generation, platelet activation and deposition of thrombus on the intraluminal surfaces of the devices can be measured as clinically relevant thrombogenicity end points.
In this study we compared the Vantage and Flex devices in an in vivo rabbit elastase aneurysm model for differences in aneurysm occlusion, vascular safety, and endothelial coverage. We additionally compared the two devices deployed in overlapped configurations in the rabbit aorta for branch vessel patency (perforator vessel occlusion). An in vitro closed loop human blood flow loop model was used to assess the thrombogenic profile of the Vantage device compared with the Flex device.
Materials and methods
Rabbit elastase in vivo studies
Devices
The following flow diversion devices were evaluated: (a) Pipeline Vantage Embolization Device with Shield Technology (Vantage, n=112, Medtronic); (b) Pipeline Flex Embolization Device (Flex, n=112, Medtronic). The devices were sized based on the target parent vessel (right subclavian artery (RSC) or descending aorta (DA)) diameters and lengths.
Rabbit elastase model and experimental procedure
Two studies were conducted in the rabbit elastase aneurysm model. Aneurysms were created using elastase in the right common carotid artery, as described previously.19 For the first study, 27 animals with aneurysms were implanted with either the Flex (n=13) or Vantage (n=14) device in the RSC covering the aneurysm neck and three each of either the Flex (n=39) or Vantage (n=42) devices in the DA across the ostia of segmental arteries in a telescoping configuration. The animals underwent aneurysm model creation procedures approximately 43–83 days before implant. The animals were euthanized at 180±2 days postoperatively. For the second study, 29 animals with aneurysms were implanted with either the Flex (n=15) or Vantage (n=14) device in the RSC across the aneurysm neck and three each of either the Flex (n=45) or Vantage (n=42) devices in the DA across the ostia of segmental arteries in a telescoping configuration. The animals underwent aneurysm model creation procedures approximately 21–48 days before implant. The animals were euthanized at 90±2 days postoperatively. Device sizing was based on the parent vessel characteristics (diameter and length) and ranged between 3–5 mm in diameter and 8–12 mm in length. Therefore, in both studies a single device was deployed in the RSC across the aneurysm neck and three overlapping (telescoping) devices were deployed in the DA across at least one branch artery. The aneurysm, RSC, and aorta dimensions for each study are shown in the online supplementary data (A1). All animals were administered aspirin (40.5 mg) and clopidogrel (37.5 mg) 1 day before the aneurysm creation procedure and up to termination.
Supplemental material
Angiographic assessment for aneurysm occlusion and parent vessel patency was performed before treatment, immediately after treatment, and before termination. Aneurysm occlusion was graded according to the Raymond Roy Occlusion Classification (RROC) blinded to device. Patency of branch vessels in the DA was also evaluated angiographically pre-treatment, immediately post-treatment and before termination.
Histopathological analysis was performed for all treated vessels from both studies with devices deployed in the RSC and the DA. For each implanted vessel, five sections per vessel were stained with hematoxylin and eosin and Movat’s pentachrome and graded by an independent pathologist for: (a) luminal thrombus; (b) endothelial cell coverage; (c) inflammation; (d) fibrin; (e) medial smooth muscle cell loss; (f) disruption of the internal elastic lamina (IEL) and external elastic lamina (EEL); and (g) disruption of adventitia. The grading scale is shown in the online supplementary data (A2).
Scanning electron microscopy (SEM) was performed on the intraluminal surfaces of the devices for Flex (control, n=3) and Vantage (test, n=3) animals in the 90 day group post-termination. Tissue coverage on the intraluminal surface was qualitatively assessed by an independent pathologist and quantitatively assessed with image analysis (Image J) for a region of interest (ROI) in each image. The ROI was defined as the area of implant for each device not including the edge artifacts from the SEM processing. Briefly, each image was converted to grayscale and a threshold was established to distinguish the area covered by exposed braid and the total vessel surface area where the device was implanted. The ratio (% area) of exposed braid to total vessel surface area was calculated for each device in both the aorta and RSC locations.
Human blood flow loop in vitro model and experiment
Devices
The following devices were evaluated: (a) Pipeline Vantage Embolization Device with Shield Technology (Vantage, n=8, 5 mm × 30 mm, Medtronic); (b) Pipeline Flex Embolization Device (Flex, n=8, 5 mm × 30 mm, Medtronic); and (c) empty loop (no device, n=8). The devices were deployed in medical grade polyvinyl chloride (PVC) tubing (4.76 mm internal diameter, Medtronic). All devices tested were final sterilized products.
Experiment and post-analysis
The model and measurement output have been described previously.15 23 Briefly, each closed loop system (approximate volume 6.4 mL) consisted of a hollow torus-shaped assembly of plastic tubing containing two blood injection and withdrawal ports and a single one-way check valve. The test devices were placed into the lumen of the plastic tubing. Each loop was prefilled with a clinically representative concentration of heparin such that the final desired heparin blood concentration was 0.6 U/mL (by volume; 80% whole blood and 20% heparin and PlasmaLyte A (Baxter)). Institutional Review Board approved protocols were established for this method and blood was collected from healthy adult human volunteers after informed consent. The loops were mounted on a rotary drum and the motion prescribed by a stepper motor connected to the drum—this motion corresponds to the pulsatile flow (pulse rate of 60 beats/min) profile of the blood inside the loop with an average flow rate of 100 mL/min. The whole system was placed inside a 37°C chamber for 60±2 min.
A total of six loops were used per experiment (n=2 Flex, n=2 Vantage, n=2 negative control—empty loop), for a total of four experiments performed on different days with four different blood donors. After each experiment, blood was withdrawn from each loop into syringes pre-filled with CTAD (citrate, theophylline, adenosine, and dipyridamole) solution (1/10th by volume) and put on ice. This blood was then centrifuged (2500 g for 20 min) and the supernatant plasma frozen at −80°C until analysis with a commercial ELISA kits for thrombin-antithrombin (TAT) complex generation (Ezygnost TAT micro, Siemens) and platelet activation (β-thromboglobulin (βTG), Asserachrom). Each loop was rinsed with PlasmaLyte A to remove non-adherent blood, photographed for gross thrombus, and then filled with Karnovsky’s fixative for SEM analysis at 30–1000 × magnification for the middle 1 cm length of the intraluminal surface of each flow diverter.
Statistical analysis
Differences in aneurysm and parent artery dimensions between Flex and Vantage groups and between 90 and 180 day cohorts were assessed with analysis of variance (ANOVA).
Differences in Raymond-Roy occlusion between Flex and Vantage were assessed with the Fisher’s exact test independently for the 90 day and 180 day study and for the combined cohort.
Differences in the histological metrics for non-zero measures between Flex and Vantage were assessed with the Kruskal-Wallis non-parametric test independently for the 90 day and 180 day study and for the combined cohort.
ANOVA was performed for the percent ratio of exposed braid area normalized to total vessel implant area for the Vantage (n=6 treated vessels, 12 surfaces) and Flex (n=6 treated vessels, 12 surfaces).
ANOVA was performed for platelet activation (βTG) and thrombin generation (TAT) measurements for the six samples per experimental run (n=2 Flex, n=2 Vantage, n=2 negative control) and for four experimental runs.
Post-hoc Fisher’s least square difference was used to identify differences between the groups with a significance value of 0.05. For non-normal datasets, a Box-Cox transformation was performed to normalize the data and statistics were performed and reported on the transformed data.
Results
Rabbit elastase aneurysm in vivo studies
All reported measures are mean±SD unless otherwise noted. Aneurysm and parent artery dimensions are shown in online supplementary data (A1). There was no significant difference in aneurysm and parent artery dimensions between Vantage and Flex groups (p<0.05). However, there was a statistical difference between the 90 and 180 day cohorts for the aneurysm height, width, and the aorta parent artery dimensions (p<0.05).
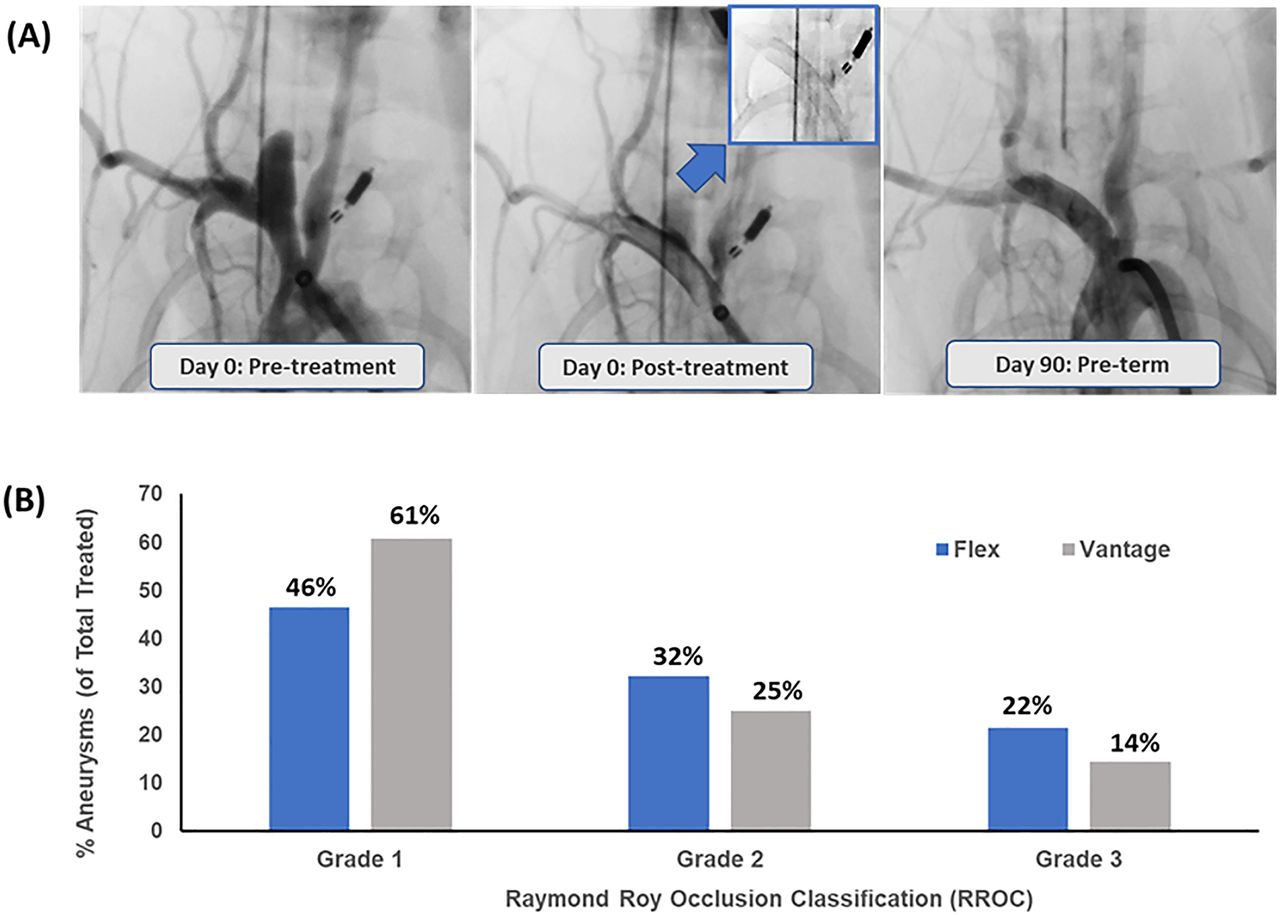
Representative angiographic images for pre-treatment, immediately post-treatment and pre-termination with the Vantage device are shown in figure 1A. The combined angiographic occlusion results for both studies (90 and 180 day) are shown in figure 1B. RROC grade 1 angiographic occlusion with Vantage (61%) was higher than Flex (46%) on average. Correspondingly, RROC grade 2 and 3 (incomplete occlusion) was higher with Flex compared with Vantage. The trend of the results is consistent with improved occlusion with Vantage relative to Flex; however, the data were not statistically significant for the 90 day, 180 day or the combined cohort, although occlusion rates were higher at 90 and 180 days in the Vantage cohort. Results of the individual cohorts (90 day and 180 day) are shown in the online supplementary data (A3).

(A) Representative angiographic images showing parent vessel patency and aneurysm occlusion: aneurysm filling pre-implant, slow aneurysm filling immediately post-implant (with inset showing a radiographic image of Vantage), and complete aneurysm occlusion pre-termination (90 day), for the Vantage device. (B) Raymond Roy Occlusion Classification for the combined 90 day and 180 day cohort for Flex and Vantage. Note: higher RROC grade 1 for Vantage compared with Flex.
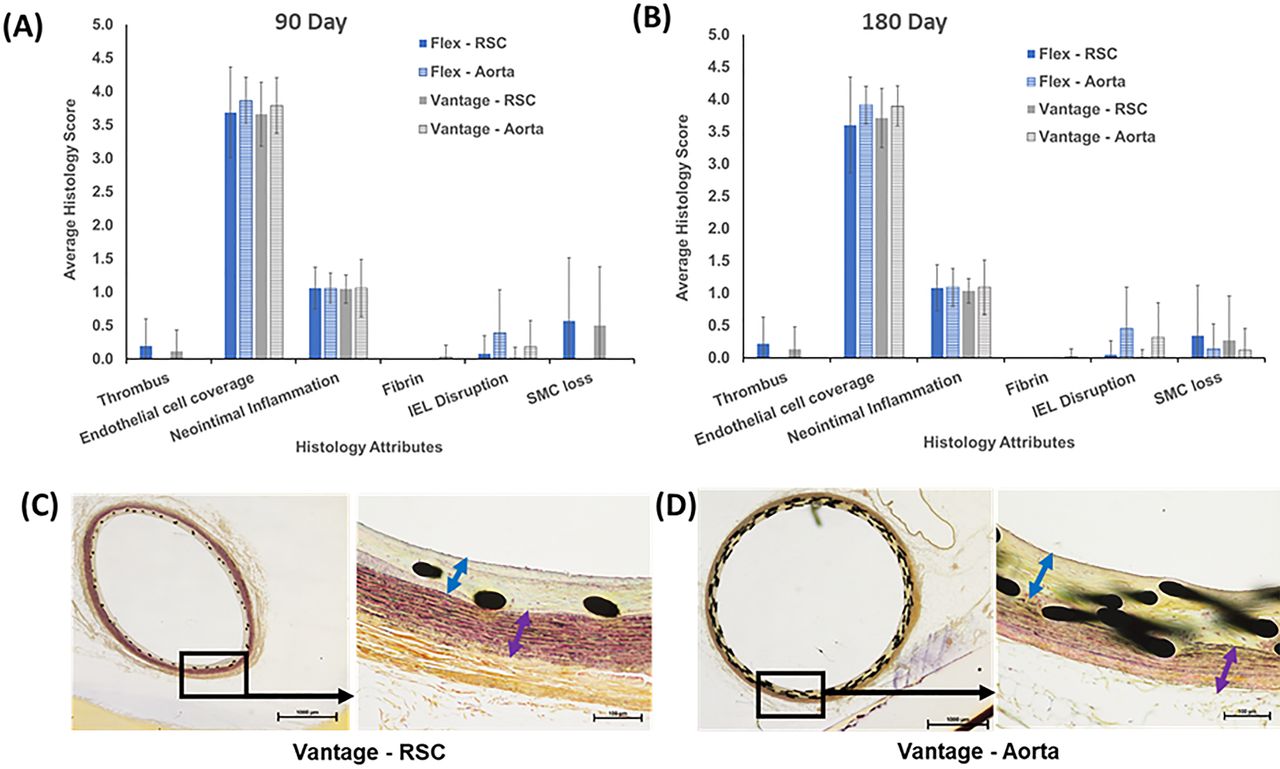
The histopathology scoring results for Flex and Vantage for the 90 day and the 180 day cohorts are shown in figure 2A and B, respectively. Only non-zero attributes are shown in the figures. There was no statistically significant difference in any of the graded histopathology attributes (thrombus, endothelial coverage, neointimal inflammation, fibrin, disruption of the IEL, EEL and adventitia, medial inflammation, and smooth muscle loss) between Flex and Vantage. The overall trends for histological measures were similar for devices deployed in both the RSC and aorta (figure 2A and B). Representative pentachrome stained sections for Vantage both from the RSC (180 day cohort, figure 2C) and aorta sections (180 day cohort, figure 2D) showed minimal inflammation, thin neointima (blue arrow) and well-preserved media (purple arrow), and coverage of the braid with tissue (endothelial coverage). Therefore, the safety biocompatibility profile of Vantage is comparable to Flex.

(A) Average 90 day and (B) 180 day cohort histology score for various parameters for Flex and Vantage devices (deployed in both RSC and aorta; mean±SD). (C) Representative Movat’s pentachrome stained section for Vantage deployed in RSC. (D) Representative Movat’s pentachrome stained section for Vantage deployed in the aorta. Blue arrows highlight thin neointima and purple arrows highlight well-preserved media. Note: Non-inferior safety biocompatibility profile of Vantage compared with Flex. IEL, internal elastic lamina; RSC, right subclavian artery; SMC, smooth muscle cell.
SEM images of intraluminal sections of Vantage and Flex from the 90 day cohort of rabbits is shown in figure 3A. Both RSC and aorta vessels were imaged from three Flex and three Vantage treated animals and show higher and more consistent endothelial coverage on the Vantage compared with the Flex. An ROI analysis (figure 3B) for the area of braid exposed relative to the area of the implanted vessel surface was performed for both Flex and Vantage images. Quantification of the exposed braid area relative to the overall vessel surface area shows that Vantage has significantly less exposed braid compared with Flex (% braid area exposed: Vantage 0.86±1.01, Flex 3.64±3.22; p<0.05) (figure 3C), and the difference is attributed to the test group (p<0.05) and not the implant location (p>0.05). Therefore, the Vantage device shows significantly improved endothelial coverage as compared with Flex.
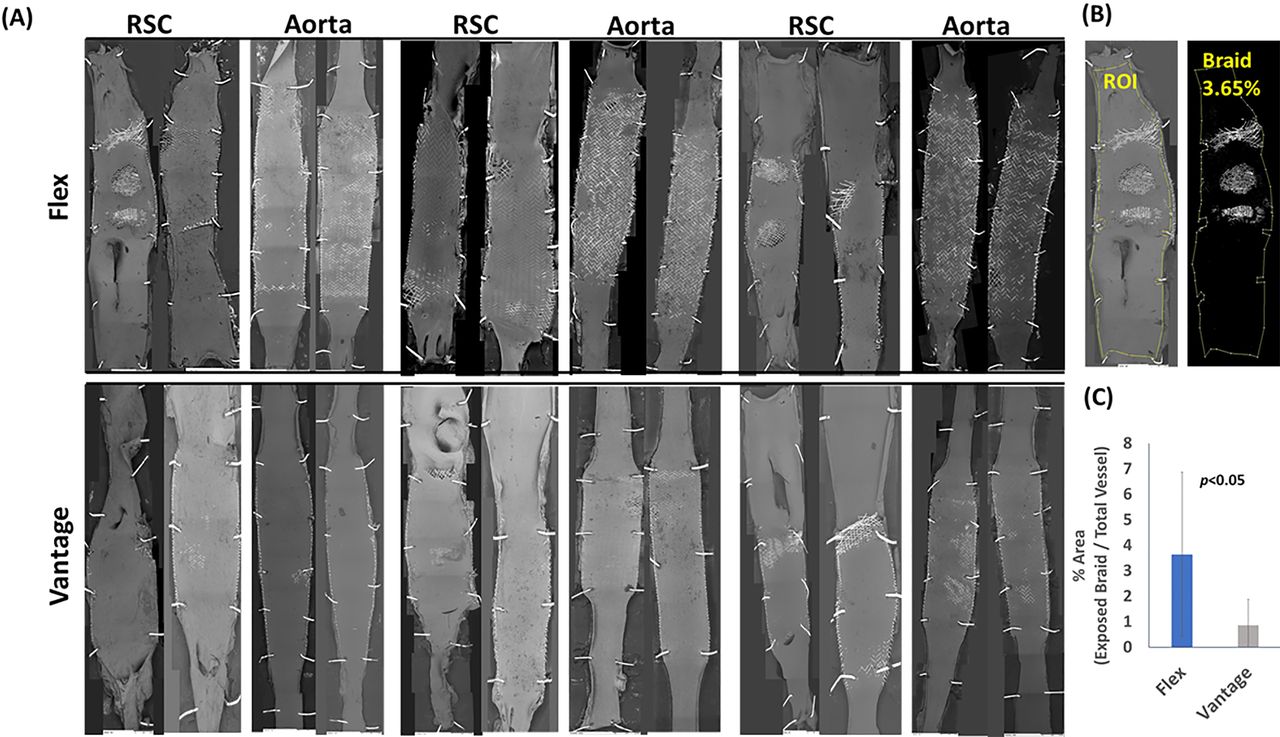
(A) Scanning electron microscopy images of tissue coverage on the intraluminal surface of Vantage and Flex (90 day cohort) in both RSC and aorta. (B) Representative image demonstrating selection of region of interest (ROI) for estimation of % exposed intraluminal implant area. (C) % Area (implant exposed area/total implanted vessel area; mean±SD) for Vantage and Flex. Note: significantly higher endothelial coverage of Vantage compared with Flex. RSC, right subclavian artery.
Human blood flow loop in vitro thrombogenicity study
Human blood flow loop experiments performed with Vantage and Flex show significantly lower thrombin generation (figure 4A, TAT: Vantage=0.49±0.45 µg/mL; Flex=10.57±9.84 µg/mL; p<0.05) and platelet activation (figure 4B, βTG: Vantage=0.41±0.19 IU/µL; Flex=4.14±2.38 IU/µL; p<0.05) with the Vantage devices. This is also confirmed by visual observation of the flow loop post-experiment and the SEM images of the inner surface of the implants showing minimal accumulation of thrombus on the Vantage braid compared with the Flex braid (figure 4C, images captured at 30×, 100×, 300× and 1000× magnification). Therefore, the thrombogenicity of Vantage is significantly lower than Flex due to the presence of Shield Technology on the former device.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) Thrombin-antithrombin complex (TAT, mean±SD, µg/mL, n=8) for Vantage, Flex, and negative control (no device). (B) β-thromboglobulin (βTG, mean±SD, IU/µL, n=8) for Vantage, Flex and negative control (no device). (C) Gross loop images post-experiment (top) and scanning electron microscopy images of devices’ intraluminal surfaces at 30x, 100x, 300x and 1000 x magnification. Note: significantly lower thrombogenicity of Vantage compared with Flex.
Discussion
In the present preclinical study, we have illustrated some key functional benefits of a novel flow diverter—Pipeline Vantage Embolization Device with Shield Technology—over the prior generation Pipeline Flex Embolization Device. Vantage demonstrated: (a) improved aneurysm occlusion at two different time points; (b) higher endothelial coverage (less exposed braid) by 90 day post-treatment; and (c) lower thrombogenicity in an in vitro human blood flow loop model (due to the presence of Shield Technology on Vantage).
As previously mentioned, optimal pore density, good wall apposition, lower implant thickness profile, and low thrombogenic profile are the desired characteristics of a flow diverter. Vantage was developed with thinner wires to have a lower implant profile and with the drawn filled tube technology (platinum filled inside the Co-Cr braid wires) for uniform fluoroscopic visibility. Additionally, Vantage (4 mm or greater labeled diameter) has a higher pore density (64 wire implants) but comparable metal coverage to the Flex. The lower implant profile and likely better wall apposition reflects in the higher tissue coverage of Vantage compared with the Flex, as observed in the SEM images from the rabbit elastase aneurysm study.
Previously, a reduction in thrombogenicity as well as early neointimal coverage of the implant was shown for the Pipeline Shield device in several preclinical models.15–18 With the incorporation of Shield Technology, these functional benefits have translated to the Vantage device. In the human blood loop study, significant reductions in thrombin generation and platelet activation together with less deposition of thrombus was observed on the intraluminal surfaces of the Vantage device—confirming the low thrombogenicity benefit. In the rabbit elastase aneurysm in vivo study, higher tissue coverage was observed on the intraluminal surfaces of the Vantage devices compared with Flex, regardless of device overlap and location of the vessel.
Thromboembolic complications remain a concern with flow diverters and may be partially addressed with surface modifications of the flow diverter. Growing efforts in this area besides the Pipeline Shield include the P48 and P64 hydrophilic polymer-coated devices with early preclinical data.24 25 Early endothelial coverage of flow diverters could also mitigate thromboembolic complications if adequate wall apposition of the device with the parent artery is achieved. Optimization of pore density of flow diverters is important to achieve adequate stagnation inside the aneurysm, improve occlusion and thereby scaffolding at the neck of the aneurysm.5 The Vantage device (>4 mm labeled diameter) has a higher pore density than the Flex but comparable metal coverage, and this should theoretically translate into improved flow diversion and higher RROC grade 1 occlusions and preserve perforator and branch vessel patency, as was observed in this study.
There are several limitations to this study. The angiographic outcomes have a similar trend for Vantage compared with Flex, both in the 90 day and 180 day rabbit cohort. However, to achieve a statistical significance would require a larger number of animals but would likely not impact the overall outcome of higher RROC grade 1 observed with Vantage compared with Flex. The 180 day cohort has lower values for RROC grade 1 results for both Vantage and Flex (online supplementary data A3). This could be attributed to differences in time between aneurysm creation and implant procedure for the 90 and 180 day cohorts and the subsequent anatomical variations (aneurysm height and width) between the two cohorts of animals. Higher endothelial coverage of the Vantage device relative to the Flex was observed in the SEM analysis. However, histological analysis showed equivalency in endothelial coverage. The histological evaluation was based on five sections per device and this may have limited complete identification of areas where endothelial coverage was not adequate with Flex. Finally, preclinical results are not representative of clinical performance and do not cover all attributes related to the device’s technical and clinical success.
In summary, Vantage achieved the theoretically desired characteristics of an idealized flow diverter and was found to have a functional benefit over Flex in the current study—using both the in vivo rabbit elastase aneurysm and the in vitro human blood flow loop. Further preclinical studies (compared with other commercially available flow diverters) in addition to clinical data are warranted to establish the value proposition of Vantage for intracranial aneurysm treatment.
References
Footnotes
Twitter @Starke_neurosurgery
Contributors Designed the study (RMS, GG, MFW, JMW), conducted the experiments (RMS, AP, AC, RJ, GG, MFW, JMW), analyzed the data (GG, MFW, RMS, AP), wrote the manuscript (GG, RMS, JT)
Funding The study was funded by Medtronic and outcome measures were independently assessed by the physician and the lab pathologist (blinded to device type). The independent physicians are also funded by the National Institute of Health.
Competing interests RMS and JT are employees of University of Miami. AP, RJ, GG, JMW, MFW, AC are employees of Medtronic. RMS research is supported by the NREF, Joe Niekro Foundation, Brain Aneurysm Foundation, Bee Foundation, and by the National Institute of Health (R01NS111119-01A1) and (UL1TR002736, KL2TR002737) through the Miami Clinical and Translational Science Institute, from the National Center for Advancing Translational Sciences and the National Institute on Minority Health and Health Disparities. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. RMS has consulting and teaching agreements with Penumbra, Abbott, Medtronic, InNeuroCo and Cerenovus.
Patient consent for publication Not required.
Ethics approval All animal studies were conducted in accordance with a local IACUC approved protocol. All human subject studies involving blood draws were conducted in accordance with an IRB approved protocol after informed consent.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data relevant to the study are included in the article and in the online supplementary information.