Article Text

Abstract
Background Implantable brain–computer interfaces (BCIs), functioning as motor neuroprostheses, have the potential to restore voluntary motor impulses to control digital devices and improve functional independence in patients with severe paralysis due to brain, spinal cord, peripheral nerve or muscle dysfunction. However, reports to date have had limited clinical translation.
Methods Two participants with amyotrophic lateral sclerosis (ALS) underwent implant in a single-arm, open-label, prospective, early feasibility study. Using a minimally invasive neurointervention procedure, a novel endovascular Stentrode BCI was implanted in the superior sagittal sinus adjacent to primary motor cortex. The participants undertook machine-learning-assisted training to use wirelessly transmitted electrocorticography signal associated with attempted movements to control multiple mouse-click actions, including zoom and left-click. Used in combination with an eye-tracker for cursor navigation, participants achieved Windows 10 operating system control to conduct instrumental activities of daily living (IADL) tasks.
Results Unsupervised home use commenced from day 86 onwards for participant 1, and day 71 for participant 2. Participant 1 achieved a typing task average click selection accuracy of 92.63% (100.00%, 87.50%–100.00%) (trial mean (median, Q1–Q3)) at a rate of 13.81 (13.44, 10.96–16.09) correct characters per minute (CCPM) with predictive text disabled. Participant 2 achieved an average click selection accuracy of 93.18% (100.00%, 88.19%–100.00%) at 20.10 (17.73, 12.27–26.50) CCPM. Completion of IADL tasks including text messaging, online shopping and managing finances independently was demonstrated in both participants.
Conclusion We describe the first-in-human experience of a minimally invasive, fully implanted, wireless, ambulatory motor neuroprosthesis using an endovascular stent-electrode array to transmit electrocorticography signals from the motor cortex for multiple command control of digital devices in two participants with flaccid upper limb paralysis.
- technology
- vein
- intervention
- device
- brain
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Severe paralysis and impaired voluntary motor function can result from a variety of conditions affecting brain, spinal cord, peripheral nerve or muscle function, and contribute to a large global burden of disease.1 People with impaired voluntary motor function often lose the ability to perform instrumental activities of daily living (IADL) tasks,2 including communication, shopping and financial management, and have an increased need for nursing home care.3 IADL disability occurs in almost all patients with amyotrophic lateral sclerosis (ALS), with 75% of patients living at home requiring assistance with finances, remote communication and shopping, leading to dependence on a caregiver.4 However, in a significant proportion of patients, the motor cortex remains functionally intact.
Brain–computer interfaces (BCIs) hold promise to restore voluntary motor control of digitally enabled devices in paralyzed individuals. Scalp electroencephalogram (EEG)-based and near infrared spectroscopy BCIs have demonstrated the capacity to translate signals into device control-commands5 6 and binary output (yes/no) communication in locked-in syndrome;7 however, complex daily system setup by caregivers or expert technicians has limited clinical translation.8 Implanted BCIs utilizing penetrating arrays9 or subdural arrays10 have demonstrated capacity for high-fidelity device control but require burr hole craniotomy for implantation. Penetrating array systems in particular have shown promise for high performance, including control of robotic limbs11 and personal computers.12 13 The high-performance power and data transmission requirements associated with penetrating arrays have created yet-to-be-overcome technical barriers for human implantation of a wireless and ambulatory system. The only report of an unsupervised, ambulatory implantable BCI utilized a subdural array and was limited to a single binary switch output for digital communication.14 We previously reported preclinical data demonstrating the potential for a permanently implanted endovascular Stentrode array to achieve comparable electrocorticography spectral content and bandwidth to epidural and subdural arrays.15
We now describe the first in-human experience of a minimally invasive, fully implanted, wireless, ambulatory motor neuroprosthesis using an endovascular stent-electrode array to transmit electrocorticography signals from the motor cortex for digital device control in two participants with flaccid upper limb paralysis.
Methods
Study design
The study design was a single-arm, open-label, prospective early feasibility trial with exploratory efficacy outcomes, conducted consistent with Food and Drug Administration (FDA) guidance of Early Feasibility Studies (EFS) of implantable BCIs.16 The protocol was approved by the St Vincent’s Hospital Melbourne Human Research Ethics Committee, Australia in November 2018 (Clinicaltrials.gov NCT03834857). The study objectives included exploratory efficacy outcomes, including signal fidelity, control of multiple motor impulse commands with training, and the use of the commands to control digitally enabled devices to conduct tasks that improve capacity for IADLs. Inclusion and exclusion criteria are listed in table 1 (online supplemental appendix 1). Dual antiplatelet therapy with aspirin and clopidogrel was commenced 14 days prior to the procedure and continued for at least 3 months. Single-agent aspirin therapy was continued for at least 12 months. Participant 1 underwent neurointervention implantation in mid-2019 and participant 2 in early 2020.
Supplemental material
Device components
The endovascular motor neuroprosthesis contained a self-expanding monolithic thin-film stent-electrode array (Stentrode, Synchron, CA, USA) designed for intracranial delivery using catheter venography neurointervention.17 Sixteen sensors were positioned circumferentially on an 8 mm × 40 mm nitinol scaffold, connected to a 50 cm flexible transvascular lead and inserted into an inductively powered internal telemetry unit (ITU, Synchron, CA, USA) (online supplemental figure S1). Vascular electrocorticographic signal (0.125 µV/bit, 2 kHz sampling rate) was transmitted wirelessly to an external telemetry unit (ETU) using infrared light, which relayed the signal to a tablet (Windows Surface Book 2, Microsoft, WA, USA) via a mobile signal control unit (figure 1).
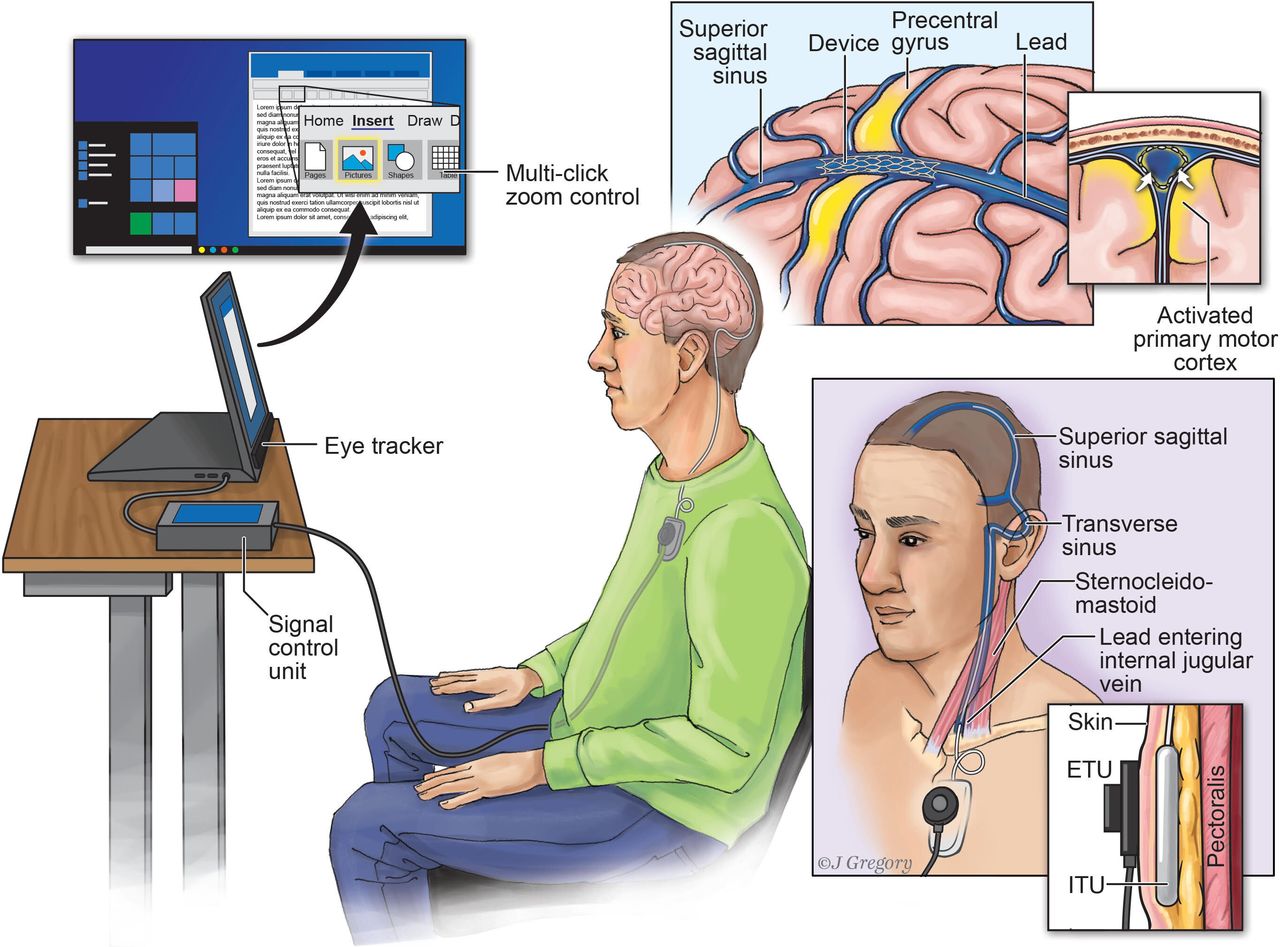
Endovascular motor neuroprosthesis system. The internal and external system components in a participant with flaccid upper limb paralysis due to motor neurone disease are demonstrated. The device was implanted within the superior sagittal sinus, immediately adjacent to the precentral gyrus. The highlighted yellow region in the brain depicts the activation of primary motor cortex that occurs with attempted limb movement. The transmission lead, exiting the internal jugular vein between the heads of sternocleidomastoid, was tunneled subcutaneously and connected to the internal telemetry unit (ITU) placed within a subclavicular pocket. The external telemetry unit (ETU) inductively powers the ITU and receives the electrocorticography signal via infrared light transmission. The signal is sent to a tablet computer via a signal control unit and translated into multiple-click actions by the custom decoder, including a zoom function and single-click command. Multiple command control was combined with eye-tracking to enable general operation of Windows 10.
Neurointervention
Under general anesthesia and guided by 3D digital subtraction angiography, co-registered to presurgical magnietic resonance imaging (MRI) marked with motor cortex deployment targets, a guide catheter was advanced into the superior sagittal sinus via the left jugular vein in participant 1 and right jugular vein in participant 2 (online supplemental appendix 1). The neuroprosthesis was implanted immediately adjacent to the precentral gyrus (figure 2D). The lead was tunneled and connected to the ITU, which was inserted in a subcutaneous pocket in the chest on the left side in participant 1 and right side in participant 2. The participant was extubated in the angiography suite and subsequently discharged home (participant 1, day 4; participant 2, day 2).

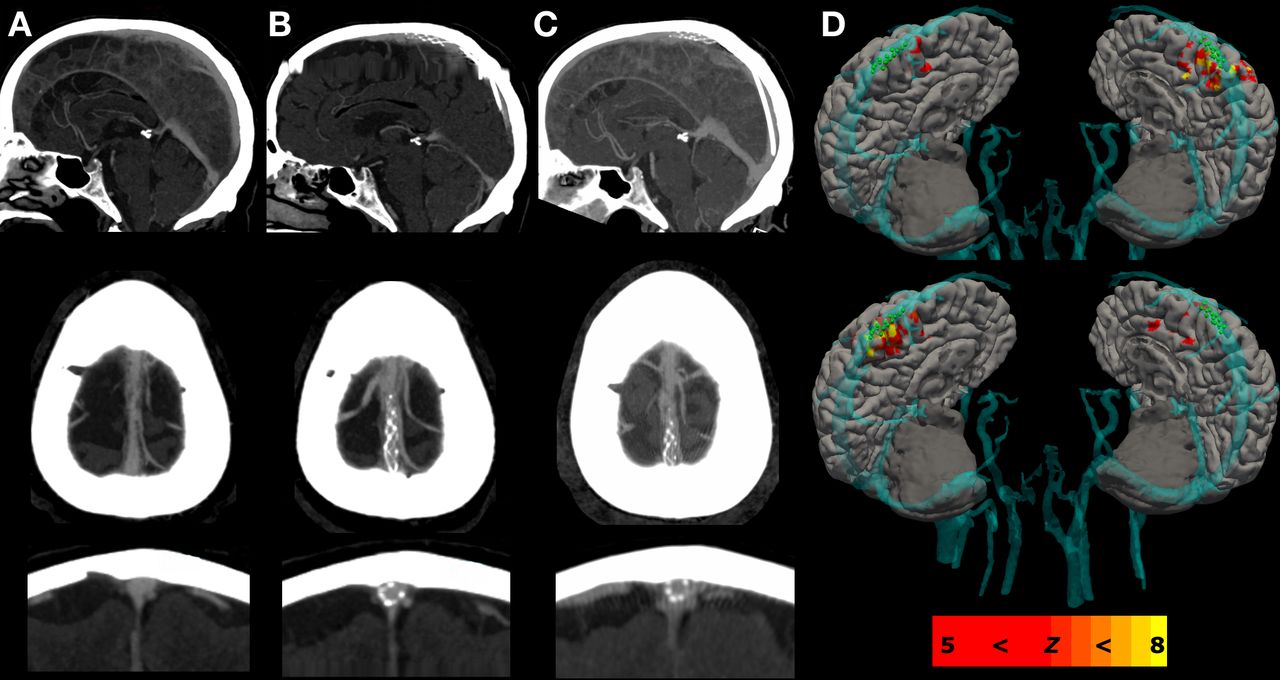
Pre- and post-neurointervention imaging. Panel A displays the baseline computed tomography venography study of the superior sagittal sinus in sagittal, axial and coronal views for participant 1. Panel B panel displays the repeat study at 3 months, and Panel C at 12 months following implantation of the Stentrode in the superior sagittal sinus, which revealed no evidence of thrombosis, stenosis or device migration. Panel D shows the regions of lower limb blood-oxygen-level-dependent (BOLD) activation relative to cortical and vascular structures derived from a preoperative magnetic resonance imaging study, co-registered to the superior sagittal sinus on intra-operative 3D digital subtraction angiography image.
Timeline
An interim period between neurointervention and training was required for wound recovery and optimization of radio communication between the telemetry units for data flow. The training period began when chest bruising was completely resolved, and a reliable infrared communication could be established. Training consisted of two planned sessions per week, conducted between days 50 and 92 post-neurointervention (across 13 sessions) for participant 1, and between day 42 and 53 post-neurointervention (across three sessions) for participant 2 (figure 3). Performance testing was conducted between days 93 and 238 post-neurointervention across six sessions for participant 1, and between days 53 and 106 post-neurointervention across five sessions for participant 2. Unsupervised home use began on days 86 and day 71 post-neurointervention for participant 1 and 2, respectively, without the need for subsequent expert decoder recalibration.

Training and testing timeline. The timeline depicts specific training and testing events that occurred following neurointervention. The number of runs performed for a given task is provided when tests were performed, presented in the order that the tasks were conducted.
Training
Training was conducted in the home with a single neuroscientist (PY) either physically or remotely present using custom training software (Synchron). Participants engaged in initial motor mapping task sessions, where a battery of movements were attempted. The battery of movement-attempts included bilateral fist clenching, foot tapping and knee extension (quadriceps contraction). If the participants had residual muscle function associated with specific movement-attempts, they were instructed to only generate effort up to, but not more than, that required to generate an explicit contraction. Alternating periods of predefined attempted movements and rest (eg, ‘push down left ankle like on a brake pedal’ or ‘clench right fist’) were performed for 2–10 s each, guided by on-screen cues. There were between 4 and 12 trials per run. Motor mapping sessions typically lasted 2 hours and were limited by what the participant could comfortably tolerate. Spectral features were optimized based on the motor mapping data and a custom machine-learning decoder was designed for each participant (online supplemental appendix 1). The decoder generated one of three potential commands every 100 ms: ‘no click’, ‘short click’ or ‘long click’. The participants used their eye-movements to control the cursor with an eye-tracker (Tobii Dynavox, PA, USA) and made click selections using the motor neuroprosthesis. Short clicks were used for typing (keyboard selections) and for single-click events. Long clicks were used for typing and to zoom/magnify the screen while searching or locking onto a target for fine-scale selections in the Windows 10 environment (online supplemental appendix video). The training period ended when an average click selection accuracy ≥90% was achieved14 across at least one run of a typing task (10 words; see Performance testing section for description of the click selection accuracy and typing task). At this point, the decoder design was fixed, and performance testing began. The participants were free to use the system unsupervised at home for control of Windows 10 with the available decoder at any given time. System setup was performed by the caregiver with no expert knowledge, which involved attaching the receiver (ETU) to the chest with medical adhesive and launching the decoding software on Windows 10.
Decoder
The custom decoder had a preprocessing, classification and click-logic layer. The preprocessing layer calculated normalized spectral power as features from the raw data. The classification layer predicted whether the features corresponded to rest or movement-attempts. The click-logic layer generated a short click when the classification layer predicted 3–9 consecutive movement-attempts (ie, 300–900 ms) immediately followed by a rest prediction. A long click command was initiated and maintained from the tenth consecutive movement-attempt prediction (ie, 1000 ms) until a subsequent rest prediction was made. This feature allowed the participants to toggle the screen magnification function for fine-scale selections.
For participant 1, the features were normalized power of 1 Hz bins between 4 and 30 Hz. A support vector machine (SVM) model was used for the classification layer, which classified neural signals into either movement-attempts or rest. The binary SVM was trained on the right quadriceps movement-attempt data because it yielded the highest offline classification accuracy. Accuracy was defined as the proportion of movement-attempts and rest that were classified correctly (online supplemental appendix 1). Decoder settings were fixed on the thirteenth training session (day 92 post-neurointervention) and required no further recalibration. For participant 2, the features were normalized average power of 5 Hz bins between 12 and 70 Hz during left ankle movement-attempts. A threshold classifier was used for the classification layer, which predicted movement-attempts if the feature crossed a given threshold level of normalized power. Low and high threshold levels were manually tuned, with the lower being easier to reach than the higher (ie, set closer to 0). The decoder defaulted to the high threshold level but automatically changed to the low level when the participant was typing by monitoring keystrokes. The decoder design was fixed on the third training session (day 53 post-neurointervention). The feature normalization constants were recalibrated at the beginning of each session, which took 30 s.
Performance testing
A typing task performed at various time points was used to assess system control performance (figure 3). The task involved the participant observing a displayed word for 2 s, typing the letters, then pressing the enter key using an on-screen keyboard. The list of possible words was derived from the 25 most frequently used nouns, verbs and adjectives as defined by the Oxford English Corpus (accessed from https://en.oxforddictionaries.com). The participant was presented with approximately 10 random words at a time. Several metrics were calculated per trial (ie, per word) and descriptive statistics were calculated across trials. Metrics included click selection accuracy, correct characters per minute and information transfer rate (online supplemental appendix 1).
The capacity of participants to perform IADL tasks were tested qualitatively. Key tasks were identified from a highly validated, generalizable IADL scale,2 including smart device (telephone) communication (texting, emailing, browsing) as well as shopping and financial management (online supplemental appendix 1). The tasks were arbitrarily designed for the participants’ needs, thereby utilising a pragmatic approach that identified the minimal level of functionality that would represent capacity for task independence.
Results
Participant 1
A patient in their 70s living at home with their partner, presenting initially with left upper limb weakness in 2016, was subsequently diagnosed with cervical onset ALS (flail limb variant) on electromyographic testing in 2018. During screening, dementia was excluded by a neurologist (SL) and respiratory assessment revealed a forced vital capacity (FVC) of 3.25 (81%). At enrolment in mid-2019, assessment by the principal investigator (BC) revealed Medical Research Council (MRC) muscle power scores of 2/5 in the distal upper limbs (fingers, wrist, elbow) and 4/5 power in the proximal shoulder, declining further to 2/5 immediately pre-implant. Lower limb assessment revealed 4/5 power bilaterally. Functionally, the loss of ability to use a personal computer or smartphone for the purposes of remote communication, including messaging, emailing and browsing, made the participant dependent on the immediate presence of their caregiver to attend to their needs in relation to technology utilization. Bulbar assessment revealed hypophonia and was subjectively declining. A trial of eye-tracking as an assistive technology failed, attributable to the participant’s poor tolerance to the lag-click function due to fatigue. Voice activation technology was also attempted without success due to soft voice.
Participant 2
A patient in their 60s, working part time, living at home with their partner and children presented initially with left biceps fasciculation in 2013, followed by diagnoses of cervical-onset ALS in 2015. Symptoms progressed with lower motor neurone weakness in upper limbs, mild dysarthria and wasting of the tongue. Screening revealed an FVC of 3.9 L (68%) and dementia was ruled out. Medication included riluzole 50 mg twice daily. Baseline neurological examination demonstrated 3/5 power in the fingers and wrist bilaterally and 4/5 in the elbow and shoulder bilaterally. Functional impairment involved inhibited use of the personal computer and digital devices for communication, adversely affecting work-related activity and independent activities at home. Lower limb assessment revealed 4/5 power bilaterally.
Preliminary safety reporting
All adverse event reporting was conducted according to Common Terminology Criteria for Adverse Events (CTCAE) V4.03 and reviewed by an independent medical monitor (RN). Data are reported for a period of 12 months post-neurointervention for participant 1 and 3 months post-neurointervention for participant 2. There were no serious adverse events for either participant. There were no device-related adverse events, including headache or infection. On day 1, participant 1e had a post-procedural-related adverse event involving an episode of syncope associated with two sinus pauses of 7.5 s and 6 s in duration, occurring while sitting in a chair. The participant was noted to be pale and unresponsive but still breathing while sitting. There was return of consciousness within 10 s while being repositioned supine. These isolated events were attributed to post-procedural vagal tone following consultation by the electrophysiology cardiologist and required no intervention.
Neurointervention
Contrast-enhanced 3D digital subtraction angiography performed immediately after device deployment demonstrated complete stent-electrode opening and device-wall apposition within the superior sagittal sinus, immediately adjacent to bilateral dorsomedial precentral gyri. Contrast-enhanced head and neck CT venography studies, performed 3 and 12 months post-neurointervention for participant 1, and 3 months post-neurointervention for participant 2, were assessed by a neuroradiologist (PM) and revealed no evidence of device migration from baseline, venous thrombosis or stenosis for both participants (figure 2A–C).
Training
Participant 1 completed training on day 92 post-neurointervention by achieving an average click selection accuracy of 95.48% (100.00%, 89.29%–100.00%) (trial mean (median, Q1–Q3)) from 53 selections made across 10 words (during session 13). Participant 2 completed training on day 53 post-neurointervention by achieving an average click selection accuracy of 93.94% (100.00%, 87.50%–100.00%) from 60 selections made across 10 words (during session 3) (online supplemental appendix 1).
Performance testing
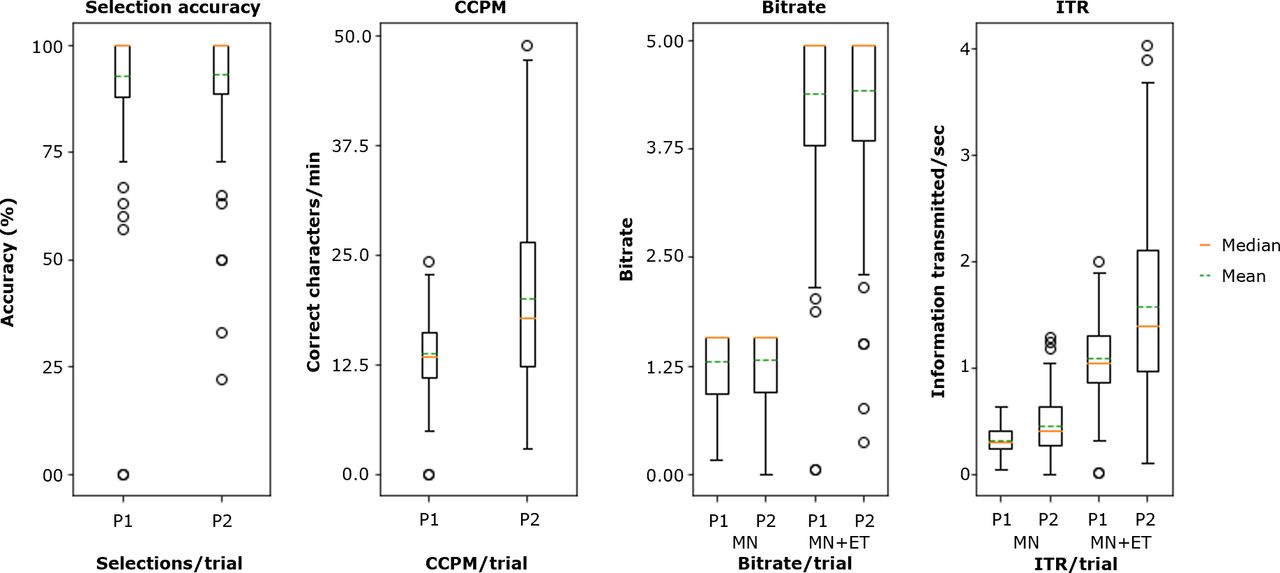
Table 1 summarizes the performance testing results. Metrics for each trial within each session are provided in the (online supplemental appendix 1). On average, participant 1 achieved a click selection accuracy of 92.63% (100.00%, 87.50%–100.00%) (trial mean (median, Q1–Q3)) across 748 selections made over 129 trials, at 13.81 (13.44, 10.96–16.09) correct characters per minute (CCPM) (figure 4). The participant achieved 1.31 (1.58, 0.92–1.58) bits/trial at an information transfer rate (ITR) of 0.32 (0.30, 0.24–0.41) bits s-1 with the motor neuroprosthesis alone, and 4.39 (4.95, 3.80–4.95) bits/trial at an ITR of 1.08 (1.05, 0.86–1.30) bits s-1 with the motor neuroprosthesis + eye-tracker. The participant successfully completed all qualitative everyday tasks (text: n=12, email: n=5, shopping: n=2, finance: n=2).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
System control performance metrics. Boxplots depict the system control performance of participant 1 (P1) and participant 2 (P2). Plots show the mean, median, interquartile range (IQR) and outliers (>±1.5*IQR) per specified performance metric calculated per trial during the typing tasks. Click selection accuracy measures the proportion of correct selections compared to the total selections made. Correct characters per minute (CCPM) measures the typing speed, correcting for errors. Bitrate measures bits transmitted per trial, irrespective of the time taken to make the selection. Information transfer rate (ITR) measures the rate of bits transferred per selection. Bitrate and ITR were calculated for the motor neuroprosthesis + eye-tracking (MN +ET) and motor neuroprosthesis alone (MN).
Participant 2 achieved an average click selection accuracy of 93.18% (100.00%, 88.19%–100.00%) across 569 selections made over 95 trials at 20.10 (17.73, 12.27–26.50) CCPM during the typing task. The participant achieved 1.33 (1.58, 0.94–1.58) bits/trial at an ITR of 0.46 (0.41, 0.28–0.63) bits s-1 with the motor neuroprosthesis alone, and 4.43 (4.95, 3.85–4.95) bits/trial at an ITR of 1.57 (1.40, 0.98–2.11) bits s-1 was transmitted with the motor neuroprosthesis + eye-tracker. The participant successfully completed all qualitative everyday tasks (text: n=5, email: n=1, shopping: n=1, finance: n=1).
Discussion
We report preliminary early feasibility data demonstrating accurate multiple command control using a fully implanted endovascular motor neuroprosthesis delivered with minimally invasive neurointervention. Two participants with flaccid upper limb paralysis due to ALS and dependent on caregivers used the ambulatory motor neuroprosthesis in conjunction with eye-tracking to control Windows 10 and independently conduct remote communication, online shopping and banking tasks.
The rate of information transmission for the motor neuroprosthesis alone was comparable to that reported in the landmark study of a fully implanted BCI.14 Implantation of that system required burr hole craniotomy, 197 days of training prior to unsupervised home use and achieved a single binary click. The current study achieved unsupervised home use of multiple-click actions within 86 days (participant 1) and 71 days (participant 2) of neurointerventional surgery. Fast uptake of the system was achieved using eye-tracking for cursor navigation. We utilised eye-tracking in place of the previously reported raster scanning for cursor navigation14 as eye-movements were preserved in the participants. Multiple command control was achieved by extending the outputs of a binary classifier to three distinct commands based on temporal dynamics of cortical signal features. While scalp EEG systems can achieve single binary click selection,18 the current endovascular approach overcomes the problem of complex daily caregiver-dependent electrode setup. Furthermore, training data showing multiclass decoding with wide-band features (online supplemental appendix figure S5) suggest the potential for future improvements in information transfer rate by increasing the discrete units of motor impulse commands, or switches.
The superior sagittal sinus encompasses the lower limb region of primary motor cortex, which likely explains why the highest quality cortical signal was generated from lower limb movement-attempts. Future applications may make use of lower limb signal for ambulatory device control systems.19 Other devices requiring complex end-effector control may necessitate rapid alternating or concurrently performed movement-attempts to achieve adequate command function. Access to other regions of motor and sensory cortex are potentially provided by superficial veins, particularly the vein of Trolard which tends to run in the central sulcus encompassing the hand knob.15 Neural activity recorded from deep folds in central sulci may be more information-rich than superficial regions20 and potentially accessible via cortical veins.
Loss of capacity to perform IADLs is a predictor of failure to live independently4 or the need for admission to a nursing home.3 The quantitative assessment of modern-day digitally enabled tasks that improve IADLs provides a challenge to the design of future clinical trials assessing efficacy of implantable BCIs. We selected tasks relating to a well-validated IADL scale2 and utilised a pragmatic approach by identifying the minimum performance required by the participants to qualitatively demonstrate independent task performance dependent on their clinical need. A limitation of this approach is that the results may not be generalizable to other patient populations. The population most likely to benefit from this technology include patients with upper limb paralysis, preserved motor cortex and preserved eye-movements. Paralysis occurs due to a highly heterogenous mix of conditions, so design of future clinical trials will require a standardized approach to task performance assessment that is clinically meaningful across a range of conditions.
Other limitations include the low number of participants studied and requirement for larger numbers to make any conclusions on the short- and long-term safety profile. The neuroprosthesis was implanted inside a blood vessel in two participants, with no evidence of thrombosis on 12- month and 3-month CT venography, respectively. Preclinical data indicate that endothelialization of the device occurs within 45 days, reducing both thrombosis risk and improving electrocorticography signal quality.15 21 Pre-existing literature from transverse sinus stent placement using cerebral venography for idiopathic intracranial hypertension suggests a rate of thrombosis or intracranial haemorrhage of less than 0.5%,22 comparing favourably to the reported risk profile of burr hole craniotomy for deep brain stimulation.23 However, further work is required to characterize the safety profile in a larger sample.
Conclusions
These first in-human data demonstrate the potential for an endovascular motor neuroprosthesis to achieve digital device control with multiple commands in people with paralysis and, when combined with eye-tracking, to improve functional independence. Further work is required to characterize the short- and long-term safety profiles as well as establish standardized task performance criteria for meaningful clinical outcomes to inform the design of a pivotal trial.
Acknowledgments
The authors would like to thank personnel who assisted in the manufacture and testing of the Stentrode device: Rodrigo Lima de Miranda, Christoph Bechtold and Christoph Chluba from Acquandas GmbH, Kiel, Germany; Andrew Wilder, Scott Hiatt, Rob Roundy and Brian Croft from Ripple LLC, Utah, USA; Randy Nelson, Cullen Boyd, Steven Scott, Greg Boeshans, Robert Cass, Stephanie Lee, Sheila Justus, Colin Boucher, Michael Hofstad, and Kevin Ward from Heraeus Medical Technologies, Minneapolis, USA; Alan Pelton, Sean Pelton and Srinidhi Nagaraja from G-RAU, California, USA; Zachary Moss and Daryl Woodman from Andersen Scientific; Martin Dieck, Janice Kemp and Amos Meltzer from Synchron, California, USA; personnel who contributed to data analytics and software development: Paul Giurata, Kevin Growney, and Zachery Brown from CatalystUX, California, USA; Robert Cunningham and Sveinar Saeverud from Tobii, Sweden; Michael Schwemmer and Adam Rich from Battelle Memorial Institute, Ohio, USA; Nick F. Ramsay, Marika Vansteensel and Erik J. Aarnoutse, from University Medical Centre, Utrecht, the Netherlands; personnel who contributed to clinical trial screening, recruitment and compliance: Jenny Stephenson, Tina Soulis, Su Cox, Gamze Akyurt from Neuroscience Trials Australia, Parkville, Australia; Dr Jim Howe, Emma Windebank, Linda Rautela, Charmaine Hovey and Adrianne Redolme, Calvary Healthcare Bethlehem, Parkdale, Australia; David Berlowitz, Institute for Breathing and Sleep, Austin Health, Victoria, Australia; personnel involved in assisting with the procedure: Richard Trent and Farah Musson, Department of Radiology, Royal Melbourne Hospital; expert consultants: Victor Rodrigues from Cochlear, NSW, Australia; Mitchell Shein; Erol Harvey, Brian Martin, Olu Ajijola; video documentation by Tim Duncan and Ed Blythe from Doctored Films; and, Jill Gregory for medical illustrations. We thank Professor Raul Nogueira, Emory University School of Medicine, Atlanta, for his role as independent safety monitor.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @tomoxl
TJO, PEY and NLO contributed equally.
Correction notice This article has been corrected since it was published Online First. The competing interest statement was updated.
Contributors Clinical trial screening and recruitment: CB, SL, SM, BC, PM. Neurointervention procedure: PM, AM, DLW, CW, IV. Peri-procedural care: BC, PM, AM, CMSL, DLW, AB, MEH, LI, SW, SMR, KD, PD. Experimental design: TJO, NO, PEY, LH, JM, AM, PM, DLW, SEJ, TD, TO’B, DG, AB, CNM, GR, SRR, VH, RPS. Preclinical data collection: NO, TJO, GR, SRR, PEY, SEJ, PM, AM, FW, CNM. Clinical data collection: PEY, PM, AM, BC, CB, AHB, CMSL, DW, IV. Data analysis: NO, PEY, DF, YW, GR, SMR, TJO, TD, SEJ, DG, AB. Manuscript drafting: PEY, TJO, NO, CB, AB. All authors reviewed and edited the manuscript. Authors TJO, PEY and NO contributed equally to this article.
Funding This work was supported by research grants from US Defense Advanced Projects Agency (DARPA) Microsystems Technology Office contract N6601-12-1-4045; Office of Naval Research (ONR) Global N26909-14-1-N020; USA Department of Defense Office of the Congressionally Directed Medical Research Programs (CDMRP), SC160158; Office of the Assistant Secretary of Defense for Health Affairs, Spinal Cord Injury Award Program W81XWH-17-1-0210; National Health and Medical Research Council of Australia (NHMRC) Grants GNT1161108, GNT1062532, GNT1138110; Australia Research Council (ARC) Linkage Grant LP150100038; Australian Federal Government, Department of Industry, Innovation and Science, GIL73654; Motor Neurone Disease Research Institute of Australia, GIA1844, Global Innovation Linkage Program, Australian Federal Government; and Synchron Inc. contributed to device fabrication.
Competing interests TJO reports stock options from Synchron, during the conduct of the study; in addition, TJO has a patent sensing or stimulating activity of tissue issued, and a patent sensing or stimulating activity of tissue pending. PEY reports stock options from Synchron, during the conduct of the study; in addition, PEY has a patent sensing or stimulating activity of tissue issued, and a patent sensing or stimulating activity of tissue pending. GSR reports stock options from Synchron, during the conduct of the study; in addition, GSR has a patent sensing or stimulating activity of tissue issued, and a patent sensing or stimulating activity of tissue pending. SMR reports stock options from Synchron, during the conduct of the study; in addition, SMR has a patent sensing or stimulating activity of tissue issued, and a patent sensing or stimulating activity of tissue pending. RPS reports stock options from Synchron, during the conduct of the study. VH reports personal fees from Synchron, during the conduct of the study. LRH reports that The Massachusetts General Hospital (MGH) Translational Research Center (TRC) has clinical research support agreements with Synchron, Paradromics and Neuralink, for which LRH provides consultative input. TD reports personal fees from Synchron, during the conduct of the study. JM reports stock options from Synchron, during the conduct of the study. NLO reports stock options from Synchron, during the conduct of the study; in addition, NLO has a patent sensing or stimulating activity of tissue issued, and a patent sensing or stimulating activity of tissue pending.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.