Article Text

Abstract
Background Larger bore aspiration catheters are expected to significantly improve the speed and completeness of acute stroke revascularization.
Objective To evaluate the navigability and clot retrieval performance of a novel 8Fr aspiration catheter, Millipede 088 (Perfuze Ltd), using fresh-frozen cadavers and an in vitro thrombectomy model, respectively.
Methods Cadaveric study: Transfemoral catheterization of the intracranial arteries was performed in six cadavers, allowing evaluation of navigation to 12 middle cerebral arteries (MCAs) and six basilar arteries. Commercially available 6Fr aspiration catheters (SOFIA Plus, Microvention) were used as controls. In vitro study: Three human blood clot phenotypes were created; red blood cell-rich, mixed, and fibrin/platelets-rich. Two clot sizes, resulting in occlusion of the internal carotid artery (ICA) and MCA-M1 were investigated. Endpoints were first-pass effect (FPE), first-pass complete ingestion, and second-pass recanalization.
Results Cadaveric study: Both the Millipede 088 and SOFIA Plus devices reached the distal MCA-M1 and the basilar artery in 10/12 and 2/2 of the navigation attempts, respectively. In the two instances of unsuccessful navigation, neither device was able to cross the ophthalmic artery. In vitro study: In 10 mm long M1 occlusions, Millipede 088 achieved 100% FPE versus 40% for 6Fr devices (p>0.001). In 20 mm long ICA occlusions, Millipede 088 achieved 100% removal success within two passes in each clot phenotype compared with an average of 27% for 6Fr devices (p>0.001).
Conclusions Navigation of the Millipede 088 catheter to the MCA-M1 and basilar artery is feasible in a cadaver model. Millipede 088 demonstrates superiority over 6Fr aspiration catheters for three representative clot phenotypes at the most common sites of occlusion in an in vitro vasculature model.
- navigation
- technique
- thrombectomy
- stroke
- device
Data availability statement
All data are available upon reasonable request to the corresponding author.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Although stentrievers were the most prevalent device used in initial trials that demonstrated the efficacy of endovascular treatment of acute ischemic stroke,1–4 subsequent trials showed that aspiration thrombectomy and stentriever devices had similar efficacy.5–7 Delgado Almandoz et al established catheter size as an independent predictor of successful revascularization (modified Thrombolysis in Cerebral Infarction 2b/3) when using a direct aspiration first-pass thrombectomy (ADAPT) technique.8 Several studies have also demonstrated a trend towards higher rates of successful reperfusion with larger bore catheters and with larger catheter-to-vessel diameter ratio.9 10
Achieving complete revascularization from a single mechanical thrombectomy attempt, termed first-pass effect (FPE), is associated with significantly improved outcomes.11 12 The prevalence of FPE remains low, with rates of 29% reported in the ASTER trial and with no significant difference observed between stentrievers and contact aspiration.13 Accordingly, significant scope remains to improve technical and associated clinical outcomes in thrombectomy.
Several authors have developed sophisticated in vitro test models to allow quantitative measurement of clot retrieval performance under controlled conditions.14–16 Complete clot ingestion has been shown to be associated with higher rates of FPE and a reduction in distal embolization compared with partial clot ingestion in an in vitro model.10 17 The highest rate of complete clot ingestion was achieved with the largest internal diameter (ID) catheter from a range of catheter sizes (0.054–0.088՛՛ ID).17 However, that study focused on a relatively low clot volume within the M1 artery. The in vitro performance of such devices in more challenging situations such as the internal carotid artery (ICA) remains unclear.
Perfuze Ltd (Galway, Ireland) has developed a novel aspiration catheter called Millipede 088, which has an 8Fr outer diameter and an 0.088’’ ID. The Millipede 088 catheter is designed to be navigated using standard interventional techniques to the intracranial vessels, has a hydrophilic coating, and is compatible with currently available 8Fr sheaths, aspiration catheters, microcatheters, and microwires. The purpose of this study was first, to evaluate the navigability of Millipede 088 in a fresh-frozen cadaver model. Second, the clot retrieval performance of the Millipede 088 was compared with industry standard 6Fr aspiration catheters (ACE 068, Penumbra, and SOFIA Plus, Microvention) in an in vitro model using ADAPT. In this study, we also present the first in vitro clot retrieval testing using human blood clot analogs.
Methods
Navigation in a cadaver model
Testing was conducted using a fresh-frozen cadaver at the Medical Education and Research Institute (MERI) (Memphis, Tennessee, USA). A single plane Siemens Artis Pheno was used for imaging. In total six cadavers were investigated using a standard transfemoral approach, allowing evaluation of navigation to 12 middle cerebral arteries (MCAs) and six basilar arteries. The commercially available SOFIA Plus (Microvention) 6F aspiration catheter was used as the control device for baseline comparison with the test device (Millipede 088, Perfuze Ltd) as it was considered by the authors to be the industry standard for navigation at the time of cadaveric testing (2019).
Access to the common carotid and subclavian arteries was obtained using a Neuron Select SIM-V catheter (Penumbra, Alameda, California, USA) and an exchange length glidewire (Microvention). Continuous infusion using hot water was used throughout the procedure. Siphon geometries were classified as C, U, V, and S according to Zhang et al, 2013.18 Aortic arch geometry was classified as bovine, type I, II, or III as described in Demertzis et al, 2010.19 Cervical tortuosity was classified as straight, curved, kinked, or coiled according to Paulsen et al, 2000.20
Control device
A Penumbra Neuron Max (ID 0.088’’) was placed at the petrous segment of the ICA. The 6F aspiration catheter was navigated through the Neuron Max over a microcatheter and microwire toward the target vessel. Initially, 2.1F microcatheters and 0.014’’ microwires were used for support. Where additional support was required, a small aspiration catheter (3Max, Penumbra) and/or 0.016’’ microwire was used.
Test device
An 80 cm long 8Fr Super Arrow-Flex (Teleflex, ID 0.113’’) or a 90 cm long 8Fr Flexor Shuttle (Cook, ID 0.113’’) sheath was placed in the proximal ICA. Various combinations of internal support were investigated: 1) 2.1F microcatheters and 0.014’’ microwires; (2) SOFIA Plus aspiration catheter. Where extra support was required to cross the ophthalmic artery, a Penumbra 3Max and/or 0.016’’ microwire was used.
Navigation performance assessment
The primary target vessels were the M1 segments of both MCAs in each cadaver as this is the most common site of occlusion in patients with acute ischemic stroke. Additionally, navigation through the posterior circulation to the basilar artery was attempted in two cadavers (1 and 5). The terminal point of navigation was recorded for each device. Where extra support was required, this was also recorded, and the associated obstacle was noted.
Human clot analogue creation
Following approval from the National University of Ireland Galway research ethics committee and in accordance with the ethical standards of the Declaration of Helsinki, human whole blood and platelet donations were obtained from the Irish blood transfusion service. Three clot analog phenotypes representative of clots retrieved from patients were created: red blood cell-rich, mixed, and fibrin/platelet-rich, as previously described.21 Histopathological analysis of clot analog composition was performed using Martius Scarlet Blue, and Orbit Image Analysis (www.Orbit.bio) was used for quantification as described previously.22 All clots were created in 2.5 cc syringes (9.5 mm ID). Following maturation of the clot analogs, clot diameters were measured to calculate the volume of clot burden being inserted into the in vitro model.
In vitro human vasculature model
The in vitro model comprised a peristaltic pump (Verderflex Economy EV3000, Castleford, UK), a modified 3D printed aortic arch, and a circle of Willis (Vascular Simulations Inc, Stony Brook, New York, USA). Pulse rate (72 bpm), flow rate (750 mL/min), and temperature (37°C) were controlled to replicate in vivo conditions. The test fluid was a 1:4 glycerol:water mixture with the addition of surfactant (Johnson & Johnson baby shampoo) to increase lubricity (10 mL/L). Clot analogs were inserted into the proximal ICA via a clot insertion port in the absence of flow and once inserted the flow rate was increased to 750 mL/min and the clot analog traveled distally and lodged under dynamic flow conditions.
Clot volume was optimized to mimic the clinical scenario; 10 mm long clots lodged in the M1 (distal M1 + MCA bifurcation), and 20 mm long clots lodged in the ICA (terminus of ICA + proximal M1 occlusion) covering both the posterior communicating artery and anterior cerebral artery. Once within the target vessel, the clots were allowed to settle for 1–2 min before an attempt was made to retrieve them. The average pressure gradient across the occlusive clot was 89 mm Hg for ICA occlusions and 112 mm Hg for M1 occlusions. A filter with 900 µm pore size was placed in the outflow to capture distal emboli.
Recanalization and degree of ingestion
The ADAPT technique was used for clot retrieval, and two thrombectomy attempts were allowed for each experiment if required. An 80 cm Super Arrow-Flex (Teleflex, ID 0.113’’) long sheath was placed in the proximal ICA. Guidewires and microcatheters were not used to cross the occlusive clot in this study. Two 6Fr catheters were employed for in vitro testing: Microvention SOFIA Plus with 070’’ ID (n=3 replicates) and Penumbra ACE 068 with 068’’ ID (n=2 replicates). The results were combined for comparison with the Millipede 088.
6Fr setup
SOFIA Plus or ACE 068 were advanced to the target artery with a Millipede 088 positioned proximal to the petrous bend of the ICA for external support.
Millipede 088 setup
The Millipede 088 was advanced to the target artery with the 80 cm sheath positioned proximal to the petrous bend of the ICA for external support.
Once the catheter was in position touching the proximal face of the clot, a 60 cc VacLok syringe (Merit Medical, Utah, USA) was used to supply a static vacuum for each aspiration attempt. Aspiration was applied through the aspiration catheter only. If the clot corked in the catheter, a timer was started for 2 min. At the end of the 2 min, the catheter was withdrawn under aspiration with the clot corked at the catheter tip. In 6Fr device testing, the corked catheter was retracted into the Millipede 088. In Millipede 088 testing, the corked catheter was retracted into the 80 cm sheath. Five replicates of each in vitro test were performed, totaling 60 tests for the study.
Endpoints were FPE, first-pass complete ingestion, and second-pass recanalization success. FPE was defined as complete removal of the clot from the target artery in the first pass. First-pass complete ingestion was defined as complete ingestion of the clot within the catheter at the site of occlusion under vacuum from the 60 cc VacLok syringe in the first pass. Second-pass recanalization success was defined as complete removal of the clot from the target artery within two passes. The occurrence of distal embolization, defined as the distal migration of clot fragments from the target arteries, was noted at the time of testing.
Statistical analysis
All statistical correlations were assessed and graphs were generated using GraphPad Prism 8. The independent t-test was used to compare the means of two independent groups.
Results
Navigation in a cadaver model
A summary of the anatomy and clinical details of the specimens and success in navigating to the anterior circulation is given in table 1. It was noted by the interventionist that the navigation characteristics of the devices in the cadaver were similar to those observed in the clinical situation. Navigation to the distal M1 was possible in 83% of vessels (10 of 12) for both the test and control devices using standard thrombectomy techniques. In 20% of cases (2 of 10) in which Millipede 088 successfully navigated to the distal M1 over SOFIA Plus (test), additional support (3MAX or Fathom 16) was required. In 10% of the successful cases (1 of 10) in which SOFIA Plus was used as a control device, additional support was required. In three of eight cases in which Millipede 088 was navigated over a 2.1F microcatheter and 014 microwire, additional support using a SOFIA Plus catheter or 3MAX was required to navigate to the distal M1. In all instances in which the M1 could not be reached or additional support was required, snagging occurred at the ophthalmic artery. The additional support of the SOFIA Plus and 3Max provides an advantage at the ostium of the ophthalmic artery and reduces the gap between the outer diameter of the microcatheter and large ID of the Millipede 088 aspiration catheter (figure 1).
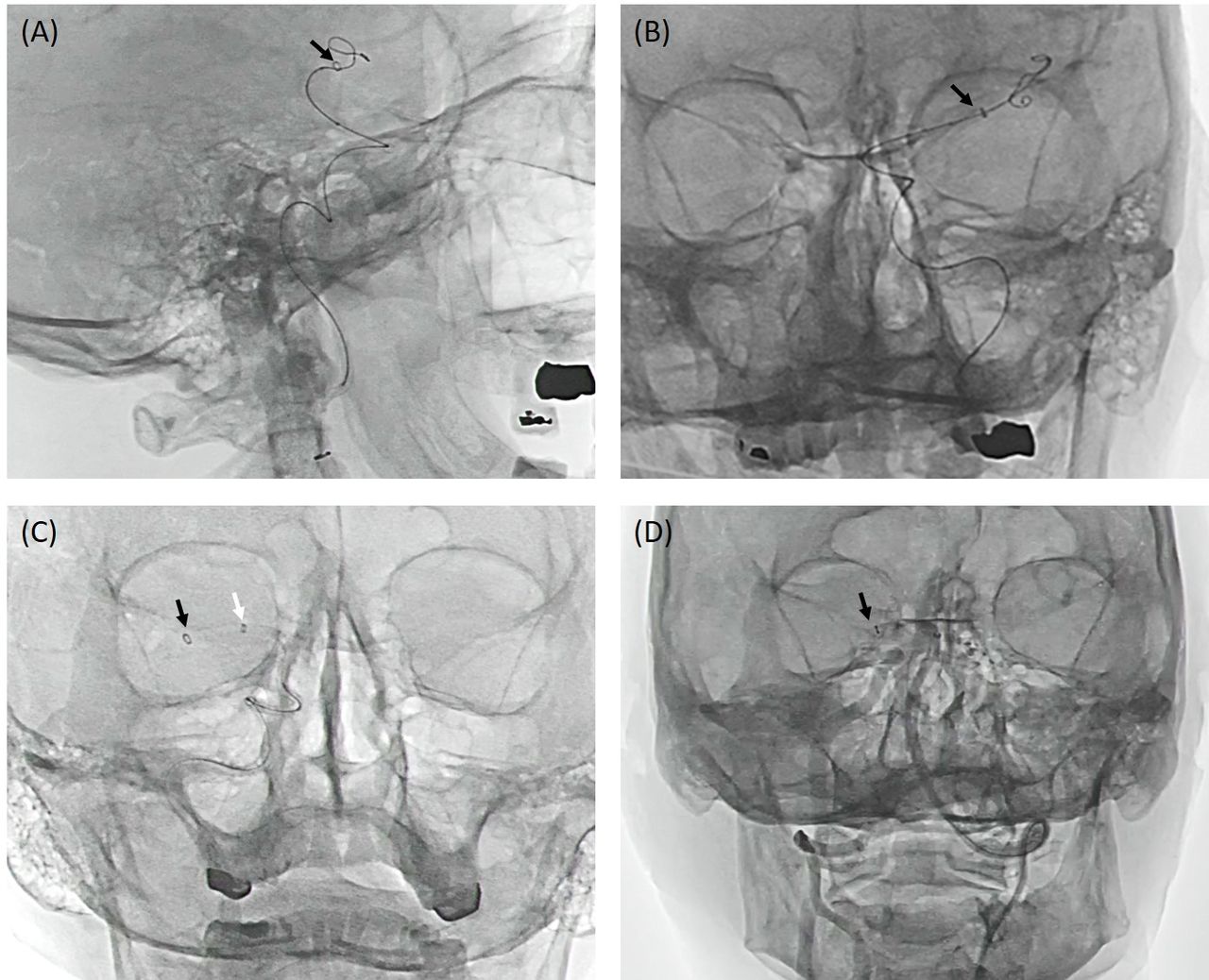
Lateral and anteroposterior views of Millipede 088 successfully tracked to the distal middle cerebral artery M1. (A) Millipede 088 navigated to M1 over 0.021'' microcatheter and 0.014'' microwire in lateral view and (B) anteroposterior view. (C) Millipede 088 navigated to M1 over a SOFIA Plus in anteroposterior view. (D) Millipede 088 navigated to the posterior cerebral artery over 0.021'' microcatheter and 0.014'' microwire in anteroposterior view. Black arrows: Millipede 088, white arrow: SOFIA Plus.
Description of anatomy and clinical details of the specimens in the cadaveric study, and terminal catheter locations for the test and control devices
Both Millipede 088 and SOFIA Plus were successfully navigated to the basilar artery in specimen 1 and 5 without difficulty (figure 1). No other maneuvers were performed in the posterior circulation.
Histological composition and volume of clot analogue phenotypes
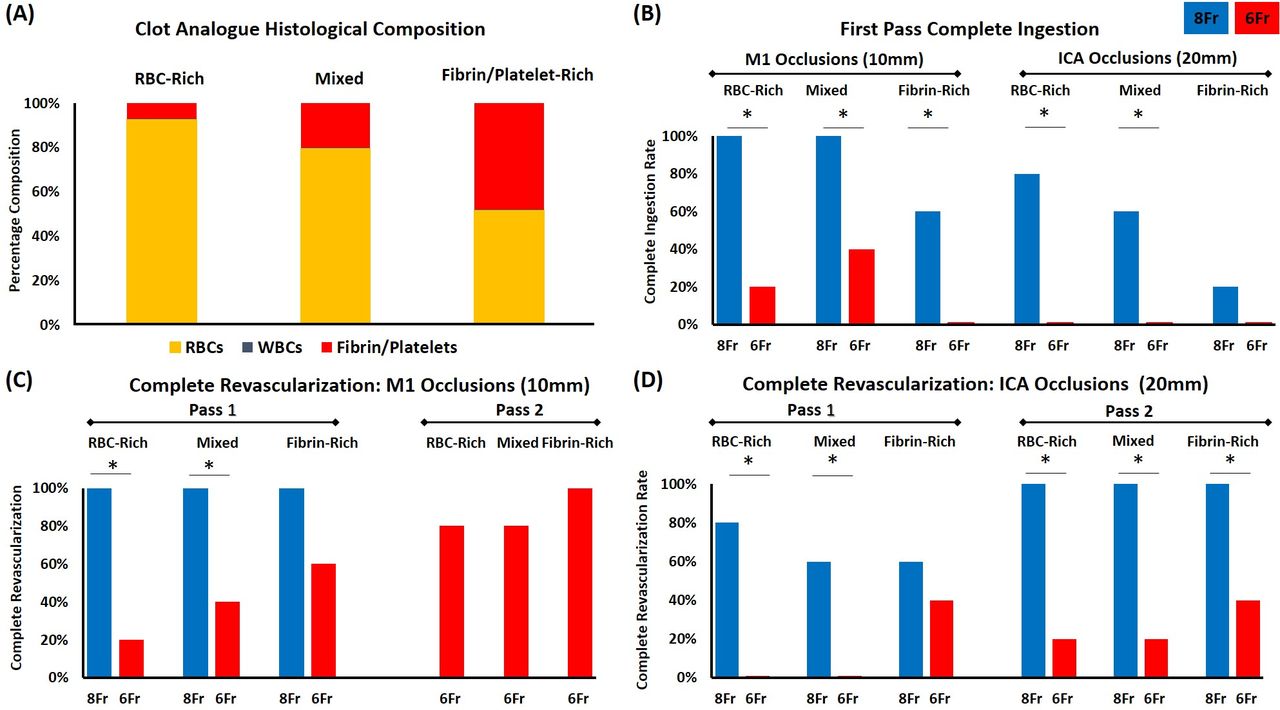
The histological composition (Figure 2A) confirmed three distinct phenotypes of clot analogues: red blood cell (RBC)-rich (RBCs: 92.9%, white blood cells (WBCs): 0.1%, fibrin/platelets: 7.0%), mixed (RBCs: 79.7%, WBCs: 0.3%, fibrin/platelets: 20.1%), and fibrin/platelets-rich (RBCs: 51.8%, WBCs: 0.3%, fibrin/platelets: 47.9%). Although the length of clot inserted was kept constant, the volume of clot for each phenotype varied owing to a variation in clot diameter resulting from increased contraction with increasing fibrin/platelets content, as previously reported.23 The average volume for 10 mm clots was RBC-rich = 50.3 mm3, mixed = 33.2 mm3, and fibrin/platelets-rich = 28.3 mm3. The average volume for 20 mm clots was RBC-rich = 100.5 mm3, mixed = 66.4 mm3, and fibrin/platelets-rich = 56.6 mm3.
Revascularization success in the in vitro model
Each device was successfully deployed to the target vessel (ICA or MCA-M1) of the in vitro vascular model in all experiments. Figure 2 shows that the Millipede 088 catheter performed better for clot retrieval for all clot phenotypes (RBC-rich, mixed, and fibrin/platelets-rich) and at both occlusion locations (ICA terminus and M1) than the 6Fr devices.
{kind=link}
{kind=link}
Histological measurement of clot analogs and comparison of 6Fr and 8Fr catheters in the in vitro model. (A) The histological composition of the three human clot analog phenotypes (RBC-rich, mixed, and fibrin/platelets-rich) used in the study was assessed and quantified using the MSB stain, (n=3 replicates for each clot phenotype). (B) Comparison of the first-pass complete ingestion of Millipede 088 (8Fr) versus 6Fr catheters in M1 and ICA occlusions. (C) Comparison of the first-pass and second-pass revascularization success rates of Millipede 088 (8Fr) versus 6Fr catheters in M1 (10 mm) occlusions. (D) Comparison of the first-pass and second-pass revascularization success rates of Millipede 088 (8Fr) versus 6Fr catheters in ICA (20 mm) occlusions. n=5 replicates in all in vitro tests. ICA, internal carotid artery; MSB, Martius Scarlet Blue; RBCs, red blood cells; WBCs, white blood cells.
M1 occlusions (10 mm)
The Millipede 088 demonstrated superior clot retrieval compared with the 6Fr devices for all three clot types. In M1 occlusions (10 mm) the Millipede 088 achieved 100% FPE in all three clot phenotypes compared with 20% in RBC-rich clots (p=0.002), 40% in mixed clots (p=0.020), and 60% in fibrin/platelets-rich clots (p=0.071) for the 6Fr devices (figure 2C). After two passes of the 6Fr devices, complete revascularization was still not achieved in 20% of RBC-rich and mixed clots (figure 2C). Failure to achieve FPE with 6Fr devices was due to the clot remaining in the target artery in 67% of tests and distal embolization from the target artery in the remaining 33%.
The Millipede 088 achieved first-pass complete ingestion in 100% of both RBC-rich and mixed clots compared with 20% of RBC-rich clots (p=0.002*) and 40% of mixed clots (p=0.020*) by the 6Fr devices (figure 2B). For fibrin/platelets-rich clots the Millipede 088 achieved first-pass complete ingestion in 60% of attempts compared with 0% for the 6Fr devices (p=0.020; figure 2B).
ICA occlusions (20 mm)
In ICA occlusions (20 mm) the Millipede 088 achieved 80% FPE in RBC-rich clots compared with 0% for the 6Fr devices (p=0.002; figure 2D). In mixed clots, the Millipede 088 achieved FPE in 60% of attempts compared with 0% for the 6Fr devices (p=0.020; figure 2D). For fibrin/platelets-rich clots the Millipede 088 achieved FPE in 60% of attempts compared with 40% for the 6Fr devices (p=0.289; figure 2D). After two passes, the Millipede 088 achieved complete revascularization for all three clot phenotypes compared with 20% of RBC-rich clots (p=0.002*), 20% of mixed clots (p=0.002*), and 40% of fibrin/platelets-rich clots (p=0.020*) for the 6Fr devices (figure 2D). Failure to achieve second-pass recanalization success with 6Fr devices was due to the clot remaining in the target artery in 64% of tests and distal embolization from the target artery in the remaining 36%.
In ICA occlusions (20 mm) the Millipede 088 achieved 80% first-pass complete ingestion in RBC-rich clots compared with 0% for the 6Fr devices (p=0.002; figure 2B). In mixed clots, the Millipede 088 achieved first-pass complete ingestion in 60% of attempts compared with 0% for the 6Fr devices (p=0.020; figure 2B). For fibrin/platelets-rich clots the Millipede 088 achieved first-pass complete ingestion in 20% of attempts compared with 0% for the 6Fr devices (p=0.173; figure 2B).
Discussion
In this study, we demonstrate that the 8Fr Millipede 088 aspiration catheter with an ID of 0.088’’ can be successfully navigated to the distal M1 segment of the MCA and the basilar artery. We also show that in an in vitro model of the human vasculature, Millipede 088 demonstrates superiority over 6Fr aspiration catheters for several clot phenotypes at the most common sites of occlusion. These findings are important because they demonstrate that navigation of an 8Fr device to the distal M1 is reproducibly achievable in humans and that 8Fr devices are superior to 6Fr devices in an in vitro thrombectomy model.
In the described cadaver work, navigation to the distal MCA-M1 was possible in 83% of vessels (10 of 12) using both the test (Millipede 088) and control (SOFIA Plus) devices, demonstrating comparable navigability performance of the Millipede 088 with the industry standard 6Fr device. In the instances where the aspiration catheters could not be navigated to the M1, the ostium of the ophthalmic origin presented a challenge for both devices. A recent study demonstrated that navigation of a 6Fr device (SOFIA Plus, Microvention) failed to reach the proximal end of the thrombus in 28% of patients treated with an aspiration-first approach.7 While a larger lumen is known to facilitate effective clot removal, it also creates a larger gap between the aspiration catheter and microcatheter or guidewire used for support, and consequently, large bore catheters may require additional internal support to cross the ophthalmic artery in challenging anatomies. In three out of eight cases, further internal support of a SOFIA Plus Catheter or 3MAX was required for the Millipede 088 to reach the M1. Specialized devices such as the Wedge (Microvention) and AXS Offset (Stryker) that help to cross the ophthalmic artery are being tested and are likely to play a role in the delivery of the next generation of larger aspiration catheters, such as Millipede 088.
Clots retrieved from patients can generally be stratified into four main phenotypes based on their histological composition: RBC-rich, mixed, fibrin-rich, and platelet-rich.22 Previous studies have successfully created blood clot analogs for in vitro testing using animal blood of various species, and these have greatly advanced our understanding of clot biomechanics and imaging characteristics.24 25 We present the first in vitro clot retrieval testing using human blood clot analogs. The histological composition of the clot analog phenotypes created in this study is in line with the range of clot compositions typically retrieved during acute ischemic stroke procedures.22
Previous in vitro thrombectomy studies have focused primarily on MCA occlusions when assessing device performance as it is the primary site of occlusions in patients.10 15 16 However, Dutra et al, compared ICA clots with more distal clots in the proximal and distal M1, and the findings demonstrated that more proximal location, higher clot burden, and longer length are associated with worse functional outcome and a longer endovascular procedure.26 Therefore, in this study, we compared the performance of the catheters in both the M1 and ICA. The volume and length of clots were optimized to represent the clinical scenario with shorter 10 mm clots used in the M1 and longer 20 mm clots lodged in the ICA, occluding both the posterior communicating artery and anterior cerebral artery. Indeed, the larger volume clots in this work were associated with less success for all endpoints: FPE, first-pass complete ingestion and second-pass revascularization success. Additionally, there was a higher rate of distal embolization from the target artery in larger volume ICA occlusions.
The achievement of complete revascularization from a single thrombectomy device pass (FPE) is associated with significantly higher rates of good clinical outcome and is the new benchmark for thrombectomy treatment.13 14 In agreement with a previous study investigating a 0.088” aspiration catheter for M1 occlusions, we found that the rates of FPE were significantly better in the Millipede 088 than in the 6Fr devices for all three clot phenotypes.10 In M1 occlusions, Millipede 088 achieved 100% first-pass complete revascularization in all clot phenotypes, compared with an average of 40% in the 6Fr devices.
The removal of the occlusive clot in a fragmented manner with multiple procedural passes increases the potential of embolization to new territories, a major contributing factor to poor neurological outcomes due to additional brain infarction.27 28 In longer ICA occlusions, the rates of FPE were again significantly better in the Millipede 088 than in the 6Fr devices, but neither the Millipede 088 nor 6Fr devices achieved 100% FPE for all clot phenotypes. However, after two passes in ICA occlusions, the Millipede 088 achieved complete revascularization in all three clot phenotypes compared with 20% in RBC-rich and mixed clots and 40% in fibrin/platelets-rich clots for the 6Fr devices. The rate of distal embolization was also higher in 6Fr devices than with the Millipede 088.
Complete ingestion of the clot into the aspiration catheter is beneficial as once the clot has cleared the catheter and reached the syringe or aspiration pump, free flow is restored. This enables the physician to immediately perform angiography to assess revascularization or continue to further removal of the clot. When a clot corks in a catheter, the clinician is forced to retract the corked catheter into the support catheter, often retrieving some or all of the clot but at the expense of losing access to the target artery. Additionally, there is an increased risk of clot fragmentation when removing a corked clot, particularly in the absence of flow arrest. The rates of first-pass complete ingestion were better with the Millipede 088 devices than with the 6Fr devices in both shorter M1 and longer M1 occlusions. The rate of first-pass complete ingestion was best in the RBC-rich clots, which are typically softer, more friable clots. Fibrin/platelet-rich clots are typically stiff, compacted clots and despite having the smallest volume on insertion, they had the poorest rate of first-pass complete ingestion in both ICA and M1 occlusions.
These findings have implications for the treatment of large vessel occlusions. Low rates of FPE results in longer procedures and removal of the clot in a fragmented fashion (ie, multiple passes), which results in a higher rate of distal embolization. Both these factors contribute to poorer patient outcomes.27 29 A device capable of retrieving a larger clot burden should be used to optimize the chances of achieving a successful FPE.13 The use of a balloon guide catheter to achieve proximal flow control has been shown to be associated with a lower risk of distal embolization, shorter procedure time, and higher rate of first-pass success.30 However, when the Millipede 088 is navigated into the distal ICA and M1 it is likely to be occlusive or near occlusive and therefore the advantage of the concomitant use of a balloon guide catheter may be limited in these cases. Further investigation would be required to properly evaluate this. The use of stentriever devices in combination with an aspiration catheter is another commonly used thrombectomy technique. Although the Millipede 088 is designed to allow rescue maneuvers using a stentriever, this technique was not investigated in this study.
It is a limitation of the cadaver model that circulating blood flow is not present and therefore, effects such as coagulation and the impact on friction between the devices and vessels may be different from in vivo conditions. Furthermore, while the fresh-frozen cadaver model is often considered a 'gold standard' for surgical training and biomechanical testing, tissue elasticity and movement may differ from the clinical situation. In the in vitro model, although the occurrence of distal embolization during each retrieval attempt was recorded in this study, the number and size of particles that embolized were not characterized. However, a previous study demonstrated a significant reduction in the number and size of distal emboli using an 088 catheter in comparison with smaller aspiration catheters when clot ingestion occurred.10 It is a limitation of both the cadaver and bench testing that vascular injury cannot be evaluated. The recent regulatory approval and studies of larger lumen catheters (up to 0.074’’) support their risk profile for vascular injury.31 Animal studies including histopathology are conducted to evaluate vascular injury of the Millipede 088 as part of the full preclinical testing program for regulatory approval.
Conclusions
Navigation of the Millipede 088 catheter to the MCA-M1 and basilar artery is feasible in a cadaver model. The ophthalmic artery origin can be a challenge to navigation, which in the majority of cases can be overcome using the support of standard neurovascular devices. In an in vitro model, Millipede 088 demonstrates superior revascularization success for three distinct clot phenotypes at the most common sites of occlusion compared with 6Fr aspiration catheters using human clot analogs.
Data availability statement
All data are available upon reasonable request to the corresponding author.
Ethics statements
Ethics approval
The cadaveric work was approved by the Medical Education & Research Institute (MERI) (Study Numbers 19–1311-ME & 19–0828-ME) accredited by the American Association of Tissue Banks (AATB). Ethical approval for the In-vitro study was granted by the National University of Ireland Research Ethics committee (19-DEC-11).
References
Footnotes
Twitter @FitzSeanT
Contributors SF: study design, performing experiments, data analysis, and drafting the manuscript. DR: performing in vitro experiments and data analysis. JT: study design, data analysis, and drafting the manuscript. RN: study design, performing the cadaveric testing, data analysis, and drafting the manuscript.
Funding This work was supported by the European Regional Development Enterprise Ireland grant number IP-2019–0865.
Competing interests SF received research funding from Enterprise Ireland that is co-funded by Perfuze Ltd. JT declares the following competing interests: Perfuze (physician advisory board, stock options); Microvention (consultant - moderate); Johnson and Johnsons (consultant - moderate). RN declares the following competing interests; Stryker Neurovascular (DAWN Trial principal investigator - no compensation, TREVO Registry steering committee - no compensation; consultant - significant); Cerenovus/Neuravi (ENDOLOW Trial principal investigator - no compensation, EXCELLENT Registry principal investigator - no compensation, ARISE-2 Trial steering committee - no compensation, physician advisory board - modest); Phenox (PROST Trial principal investigator, physician advisory board - modest); Anaconda (physician advisory board - modest); Genentech (physician advisory board - modest); Perfuze (physician advisory board - stock options); Biogen (CHARM Trial steering committee; physician advisory board - modest); Prolong Pharmaceuticals (physician advisory board - modest); Brainomix (physician advisory board - stock options); Viz-AI (physician advisory board - stock options); Corindus Vascular Robotics (physician advisory board - stock options); Vesalio (physician advisory board - stock options); Ceretrieve (physician advisory board - stock options); Astrocyte (physician advisory board - stock options); Cerebrotech (physician advisory board - stock options); Imperative Care (Imperative Trial principal investigator - modest).
Provenance and peer review Not commissioned; externally peer reviewed.