Article Text

Abstract
Objectives To reduce occupational radiation exposure in a hybrid operating room (OR) used for three-dimensional (3D) image guided spine procedures. The effects of staff positioning, different X-ray imaging systems, and freestanding radiation protection shields (RPSs) were considered.
Methods An anthropomorphic phantom was imaged with a robotic ceiling mounted hybrid OR C-arm cone beam CT (hCBCT), a mobile O-arm CBCT (oCBCT), and a mobile two-dimensional C-arm fluoroscopy system. The resulting scatter doses were measured at different positions in the hybrid OR using active personal dosimeters and an ionization chamber. Two types of RPSs were evaluated.
Results Using the hCBCT system instead of the oCBCT system reduced the occupational radiation dose on average by 22%. At 200 cm from the phantom, scatter doses from the hCBCT were 27% lower compared with the oCBCT. One rotational acquisition with hCBCT or oCBCT corresponded to 12 or 16 min of fluoroscopy with the C-arm, respectively. The scatter dose decreased by more than 90% behind an RPS. However, the protection was slightly less effective at 60 cm behind the RPS, due to tertiary scatter from the surroundings.
Conclusions For 3D image guided spine procedures in the hybrid OR, occupational radiation exposure is lowered by using hCBCT rather than oCBCT. Radiation exposure can also be decreased by optimal staff positioning in the OR, considering distance to the source and positioning relative to the walls, ceiling, and RPS. In this setting and workflow, staff can use RPSs instead of heavy aprons during intraoperative CBCT imaging, to achieve effective whole body dose reduction with improved comfort.
- CT
- spine
- technology
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
The use of intraoperative image guided navigation in spine surgery can decrease complications, such as malpositioned pedicle screws, or neural and vascular damage.1 2 In recent years, intraoperative three-dimensional (3D) imaging using cone beam CT (CBCT) for spine surgery has rapidly increased. Navigation based on intraoperative 3D imaging provides more accurate surgical guidance, reducing the need for revision surgery and shortening hospital stay and recovery times.3–5 However, the use of CBCT may increase the radiation exposure to patients and staff.5–9
The health risks associated with occupational radiation exposure are either of a deterministic or stochastic nature. The main deterministic tissue reaction in a surgical or interventional setting is radiation induced lens opacities and cataract, which can occur at substantially lower doses than previously believed.10 Stochastic effects occur by chance and include the induction of cancer. The risk is considered to increase with dose according to the linear-no-threshold model. The International Commission on Radiological Protection has recommended an annual occupational exposure limit of 20 mSv/year, averaged over 5 years, in both effective dose and equivalent eye lens dose.10 11
Staff radiation exposure is caused by X-rays being scattered in the patient, changing their trajectory. Radiation protection measures, such as proper positioning of staff members, radiation protection shields (RPSs), lead aprons, and lead glasses are important in reducing exposure to scatter radiation.12 13 Understanding radiation safety and adhering to safety protocols are vital to minimize occupational radiation exposure.5 6 14 15
We hypothesized that the radiation environment in a hybrid operating room (OR) for 3D image guided spine procedures varies depending on different imaging systems, staff position, and use of RPSs. The commercially available flat panel X-ray systems investigated, henceforth referred to as imaging devices, were a robotic ceiling mounted hybrid OR cone beam CT (hCBCT) system, a mobile O-arm cone beam CT (oCBCT) system, and a mobile C-arm fluoroscopic imaging system (C-arm). Conventional navigation systems are dependent on 3D imaging, and the selected imaging devices in this study represent the state of the art in intraoperative CBCT. The C-arm is used in non-navigated free hand placement of pedicle screws. Occupational dose distribution was evaluated using active personal dosimeters (APD), which are well suited to measure occupational radiation in radiology.16 The scatter doses were measured using an open air ionization chamber more suitable for low dose measurements. The purpose of the present study was to measure and compare occupational radiation dose levels for three imaging devices, evaluating the effects of different protocols, staff positioning, and the use of RPS.
Materials and methods
The study was conducted in a 120 m2 hybrid OR with a ceiling height of 320 cm. Centered and fixed to the floor was a surgical table (Alphamaquet 1150, Maquet AG, Switzerland). An anthropomorphic whole body phantom was positioned on the surgical OR table representing a patient undergoing a spine procedure (PBU-60, Kyoto Kagaku, Tokyo, Japan). The phantom contains a synthetic skeleton embedded in soft tissue substitute.17 The phantom measures 165 cm and weighs 50 kg, serving as an artificial body for generating scatter radiation. In all measurements, the phantom was positioned on the surgical table in the supine position and examined at thoracic and lumbar spine levels, T11–L4.
Imaging devices
Three commercially available devices were compared: the Allura Clarity image guided therapy system (Philips Healthcare, Best, the Netherlands), the O‐arm O2 image guided CBCT (Medtronic, Littleton, Massachusetts, USA), and the Veradius Unity Mobile C-arm (Philips Healthcare). All three devices use a flat panel detector, which enables two‐dimensional (2D) fluoroscopy imaging. The hCBCT and oCBCT can also be used to obtain 3D CBCT images. The oCBCT and the C-arm are mobile (wheel mounted), while the hCBCT is a ceiling mounted robotized device. The three devices have preprogrammed imaging protocols optimized for spine (table 1). When 3D navigation is used, there is no need for fluoroscopy. However, many centers and surgeons still use fluoroscopy assisted free hand technique despite the advantages of 3D navigation. The C-arm in this study is only included for the sake of comparison and to resemble the possible workflow in a spinal surgical theater.
Settings used for the different scanning acquisitions, performed with the Philips Allura Clarity (hybrid operating room cone beam CT system), Medtronic O-arm O2 (O-arm cone beam CT system), and Philips Veradius Unity mobile C-arm
The hCBCT provides three different options, 27, 37, and 48 cm, for field of view (FOV), corresponding to the diagonal measures at the imaging detector. In this study, these options are referred to as small (S), medium (M), and large (L) FOV. The standard clinical acquisition for hCBCT is the large FOV. The hCBCT applies automatic exposure control to modulate the X-ray tube current–time product (mAs), depending on patient thickness, to achieve an adequate image quality. For oCBCT and C-arm, the user has the option to manually select the dose level to achieve an improved image quality. The oCBCT uses three different parameters for imaging acquisitions: patient thickness, dose level, and FOV. In this study, patient thickness values were medium and large. Three available dose settings and two different FOV were evaluated in this work. The standard clinical acquisition is a medium patient thickness with a standard dose setting, and a 20 cm FOV (medium). On the C-arm, the dose level can be set to low, normal, and medium dose. The standard clinical acquisition is a large FOV with a normal dose setting.
Detectors
The occupational dose distribution in the hybrid OR was determined using APDs connected to the Raysafe i3 staff dosimetry system (Unfors Raysafe, Sweden). APDs measure the personal dose equivalent at 10 mm depth, Hp(10), in units of Sievert (Sv), with calibration traceable to the National Institute of Standards and Technology and Physikalisch-Technische Bundesanstalt. Note that Hp(10) is the operational dose quantity recommended for staff dosimetry as it overestimates the effective dose.18
The scatter dose, including tertiary scatter from the ceiling and walls, was determined using a cylindrical 1800 cm3 open air ionization chamber (10×6–1800, Radcal, Monrovia, California, USA), which measures the air kerma free in air (Gy), with calibration traceable to Laboratoire National Henri Becquerel.
Occupational dose distribution
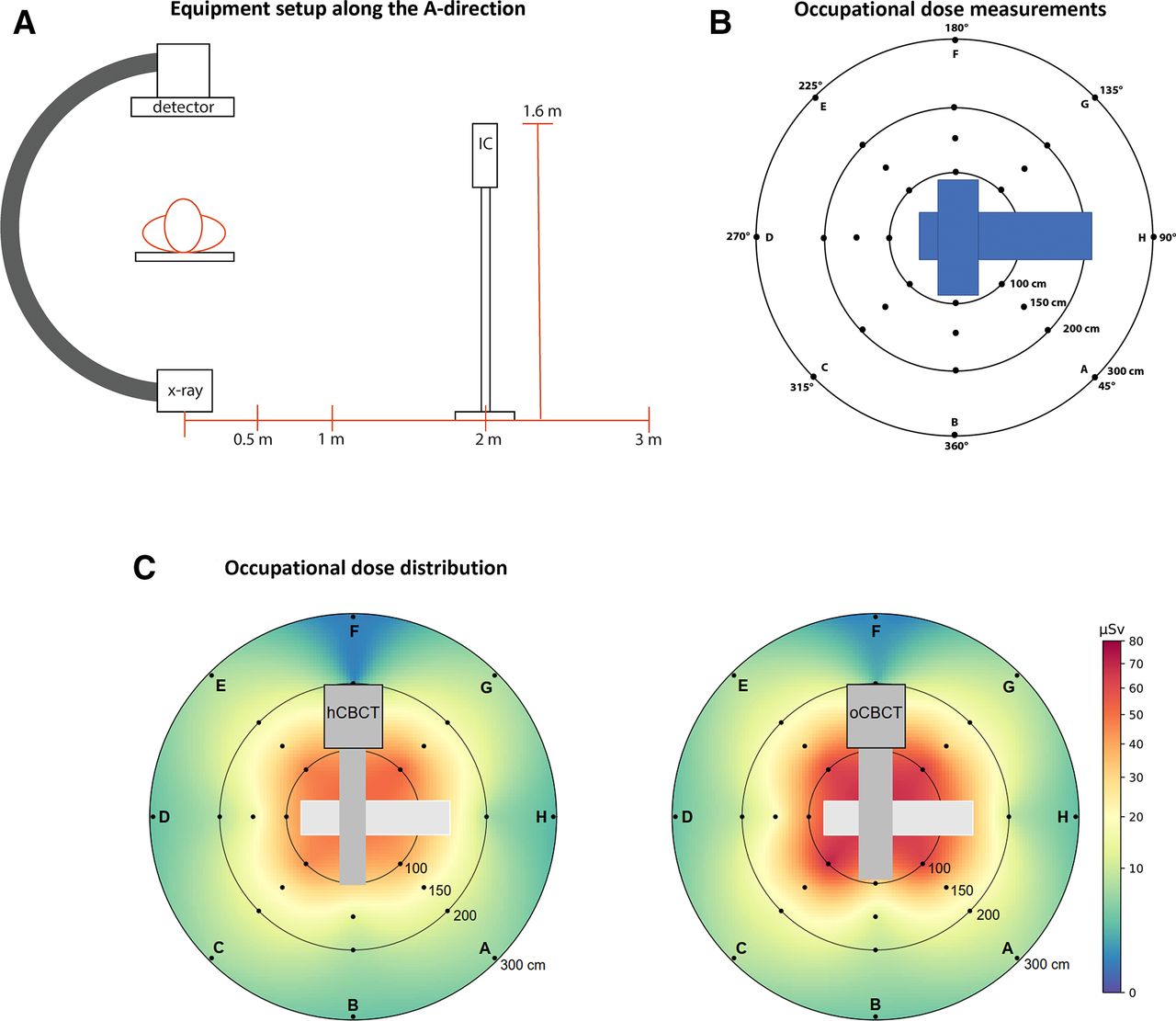
For occupational dose mapping, the radiation dose distribution in the OR was measured at fixed distances from the isocenter, covering a full 360° rotation around the patient. The measurements were performed using eight APDs simultaneously (relative response within 10%). The APDs were placed in eight different directions, A–H, at four different distances (100, 150, 200, and 300 cm) from the isocenter (figure 1A,B). They were attached to thin plastic stands at a height of 160 cm, to simulate the approximate height of the eyes for OR staff. A continuous occupational dose map of the OR was generated from the measurements using a radial basis function interpolation.

Equipment setup and measurement positions. (A) Illustration of the X-ray system, phantom, and position of the ionization chamber (IC) at a fixed height of 160 cm, representing the typical eye level height of operating room staff. (B) Distances from the device isocenter to the different measurement positions in the operating room are indicated. (C) Measurements per rotational acquisition for two devices (hybrid cone beam CT (hCBCT) system figured left and O-arm cone beam CT (oCBCT) system figured right) in terms of the personal dose equivalent Hp(10) (µSv). The results were obtained using standard clinical imaging protocols (described in table 1).
Scatter dose measurements
The scatter dose was measured at selected locations in the OR using the ionization chamber. Measurements were made in the A direction, at 50, 100, 200, and 300 cm from the isocenter, to simulate the scatter dose to staff at different distances from the patient. The ionization chamber was placed on a tripod stand, at a height of 160 cm from the floor, to simulate the eye level height of the OR staff (figure 1A,B).
Radiation protection shields
The scattered radiation behind two different RPSs was investigated to evaluate the effectiveness of commonly used radiation protection equipment in the hybrid OR. The hCBCT and two commercially available RPSs, MAVIG WD308-99 130×185 cm2 (2 mm Pb) and MAVIG WD 257 70×178 cm2 (0.5 mm Pb), were used for this purpose (online supplemental figure 1). The measurements were performed with the ionization chamber due to its high sensitivity to low fluence X-ray fields and its wide energy response, making it suitable for measuring the dose behind an RPS. Each RPS was positioned at different distances from the device isocenter (150–500 cm). In addition, the ionization chamber was positioned at different distances behind each RPS (30–240 cm).
Supplemental material
Statistical analysis
Descriptive statistics are expressed as mean (SD) or in the form of a ratio, as appropriate. The combined SD was evaluated from the measurement precision and from the reproducibility of the measurement setup. For that purpose, the type A evaluation of the standard uncertainty was performed from three readouts measured on two separate occasions with the setup reset in between (ie, six readouts in total.
For all measurements performed with the ionization chamber (air kerma), the relative combined SD was well within 1%, while the measurements performed using active personal dosimeters (Hp(10)) had a relative combined SD generally within 5%. It should be noted that for evaluation of relative dose, the potential errors due to the dependence of the measuring device on the energy, angle of radiation incidence, and the dose rate are expected to be negligible; the errors in the numerator and denominator are correlated and hence partly cancel.
Comparisons between measured doses were performed using a paired sample t test with significance level (alpha) set to 0.01. Error bars are not seen in the figures in the result section because they are smaller than the symbol or line thicknesses of the illustrations.
Results
Occupational radiation dose distribution
As expected, the highest radiation doses were measured closest to the device isocenter, and decreased with distance (figure 1C, table 2). The lowest radiation doses were measured along the F direction, behind the gantry/generator of the device. Using the hCBCT system instead of the oCBCT system reduced the radiation dose on average by 22% (p<10-8). The dose reduction ranged between 2% and 38%, depending on the position in the hybrid OR, at all measured positions compared with those of the oCBCT (table 2).
Occupational radiation doses in the hybrid operating room mapped along positions A-H (see figure 1B) for the hybrid cone beam CT and the O-arm cone beam CT systems
Scatter dose
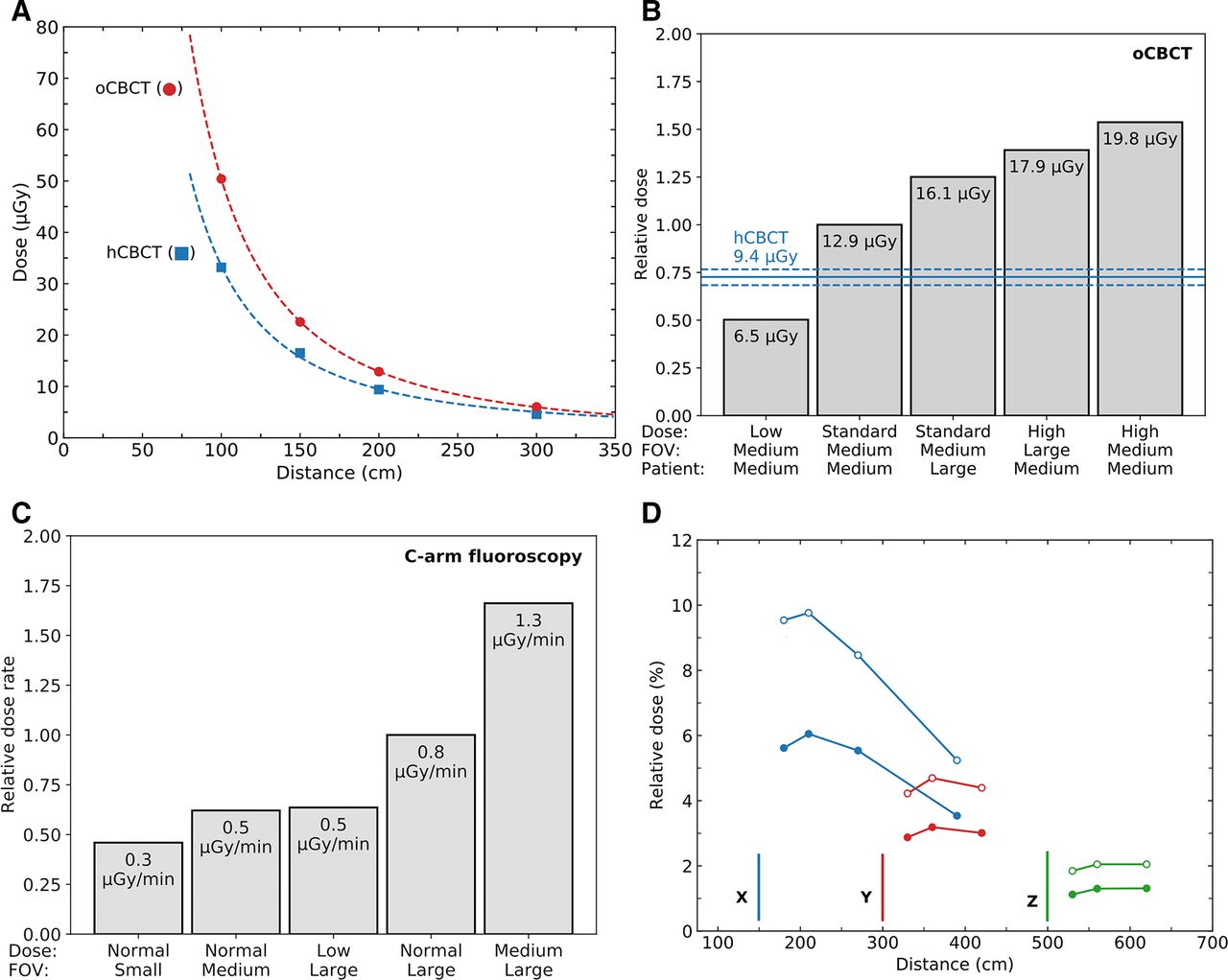
The scattered radiation doses, measured along the A direction in terms of air kerma, were significantly lower for the hCBCT compared with the oCBCT (figure 2A). Scatter doses measured at a distance of 200 cm from the isocenter along the A direction showed 27% lower values for the hCBCT than the oCBCT using the standard clinical protocols (figure 2B). At this distance, the scatter dose from a single CBCT acquisition using the hCBCT or oCBCT corresponded to 12 and 16 min of C-arm fluoroscopy, respectively (figure 2B,C). At 100 cm from the isocenter, the corresponding times were 17 and 26 min, respectively.

{kind=link}
{kind=link}
Scatter dose, relative scatter dose, and scatter radiation rate. (A) Scatter dose (air kerma) per rotational acquisition from the isocenter along the A direction (see figure 1A,B) for the cone beam CT devices (hybrid cone beam CT (hCBCT) and O-arm cone beam CT (oCBCT)), as a function of the distance. The symbols represent measured results, and the lines correspond to the measurements fitted according to the inverse square of the distance from the isocenter. (B) Relative scatter dose (air kerma) for oCBCT, measured at 200 cm from the isocenter along the A direction (see figure 1A,B), using different dose, field of view (FOV), and patient size settings. The solid and broken lines correspond to the mean value (9.4 µGy), minimum (8.8 µGy), and maximum (9.9 µGy), respectively, for hCBCT measured for three different FOVs. (C) Relative scatter dose rate (air kerma rate) for the C-arm, measured at 200 cm from the isocenter along the A direction (see figure 1A,B), using different dose and FOV settings. (D) Scatter radiation (air kerma) measured behind a large radiation protection shield (RPS) (2.0 mm Pb; filled circles), and a small RPS (0.5 mm Pb; open circles), at different distances from the hCBCT isocenter. The results are normalized to the unshielded scatter dose at 180 cm from the device isocenter. The RPSs were placed at 150 (X, blue), 300 (Y, red), and 500 cm (Z, green) from the isocenter, as indicated by the vertical lines. Measurement data behind the screens are shown in the corresponding colors. The results were obtained using the standard hCBCT clinical imaging protocols (described in table 1). The standard deviations of the measurements are smaller than the size of the symbols. The results (A–D) were obtained using standard clinical imaging protocols (described in table 1).
Radiation protection
The use of either RPS reduced the scatter doses (air kerma) from the hCBCT by more than 90% (figure 2D and online supplemental table 1). As expected, there was a significant (p<000001) benefit of using the larger and thicker lead shield (2.0 mm Pb) compared with the smaller and thinner shield (0.5 mm Pb). Two millimeters of lead reduced scatter doses by more than 94%.
Discussion
The aim of this study was to gain a better understanding of the scatter radiation environment in a hybrid OR during spine surgery, and to investigate the difference in the occupational radiation exposure depending on the imaging device used: hCBCT, oCBCT, or C-arm.19–21 To assess staff radiation dose, the occupational dose Hp(10) was measured at different positions in the OR, using different imaging protocols and RPS.
Previous publications have assessed occupational radiation exposure in vascular interventional surgery, comparing hybrid CBCT systems, and with mobile 2D fluoroscopy C-arm systems. Findings in these studies have differed depending on the type of surgical procedure, proximity to the patient, and amount of fluoroscopy. The use of high dose fluoroscopy road maps and cine acquisitions in vascular interventional surgery are not relevant to spinal neurosurgical procedures, making direct comparisons of occupational exposure difficult. To our knowledge, there has been no comparable study that has investigated differences between these devices in terms of the scatter dose and its effect on the occupational radiation environment.
According to the presented results, a 20% reduction in occupational dose can be achieved using hCBCT instead of oCBCT. In addition to a reduction in the occupational dose, a commensurate reduction in the patient dose is expected, as previously shown by Nachabe et al. 4 A possible explanation for the lower radiation dose measured with hCBCT is its use of automatic exposure control. Automatic exposure control modulates the X-ray tube current–time product according to patient thickness. Also, hCBCT uses additional X-ray beam filtration. In contrast, oCBCT has a fixed tube current–time product for a given imaging protocol. Moreover, the hCBCT system performs a 180° rotational scan with the X-ray tube under the surgical OR table, whereas the oCBCT performs a full 360° rotation. This difference causes less scatter from the hCBCT to be directed toward clinical staff, as the majority of the scatter is generated on the X-ray tube side.
The DICOM images rendered by the hCBCT and oCBCT can interchangeably be used with 3D navigation systems. Nonetheless, there are several differences between the two systems to consider. While the hCBCT requires a dedicated hybrid OR and is easily maneuvered due to its robotic ceiling mount, the oCBCT can be moved between ORs but is less easily maneuvered within the OR. Furthermore, the image quality of the two systems is not identical. Hounsfield unit accuracy, noise, and uniformity of hCBCT exceeds the performance of the oCBCT.22 This is important when detailed 3D images for augmented reality navigation are required. Nevertheless, the availability at each center will ultimately determine what imaging device is used and hence it is important to recognize the need for protocol optimization.
The lowest radiation doses were measured in the F direction, which was behind the gantry/generator of the two imaging devices. Although these positions are suboptimal for the surgeon, they can be used by OR staff, such as anesthesiologists, technicians, and students (figure 1C).
Deterministic radiation induced tissue effects, such as lens opacities and cataract, are relevant for OR staff regularly exposed to radiation, especially as radiation protection glasses are not normally worn by this group.11 The occupational eye lens dose at different positions in the hybrid OR can be estimated in terms of the Hp(10) measurements presented in this work. It has previously been shown that Hp(10) measured using APDs can be used to conservatively estimate the eye lens dose.9 23 The International Commission on Radiological Protection10 has recommended an annual limit of 20 mSv in equivalent eye lens dose. In accordance with this recommendation, a surgeon positioned 100 cm from the isocenter along the A direction can perform about 500 or 300 rotational acquisitions with hCBCT or oCBCT, respectively. Since a typical spine surgery can involve 2–8 rotational acquisitions (average of 4 per procedure),8 the average number of procedures that can be performed annually before reaching the recommended limit is about 130 or 80 for the hCBCT or oCBCT, respectively. This example demonstrates how the results presented in this work can be used to estimate risks associated with occupational exposure for staff positioned at different positions in a hybrid OR.
Traditionally, spine surgeries are performed using fluoroscopy. During fluoroscopy, the surgeon often remains at the OR table, wearing a heavy lead apron that can induce discomfort, fatigue, and back pain.24 With the introduction of 3D spine navigation based on CBCT imaging, the occupational radiation exposure can be reduced substantially, as the surgeons no longer must remain at the OR table while the patient is imaged. The surgeon will normally pause the procedure and position themselves behind an RPS before proceeding.8 However, assuming that the OR staff are not positioned behind an RPS, the scatter dose, at 100 cm from the isocenter, from a CBCT performed using the hCBCT or oCBCT is equivalent to 17 or 26 min of fluoroscopy, respectively. Comparing the occupational radiation dose for 3D and 2D imaging should, however, be done with caution, as the use of an RPS during CBCT imaging can reduce the scatter radiation by 90–99%, depending on the size, thickness, and position of the RPS (figure 2D).
Even though differences were measured between the two RPSs, reflecting lead thickness, the absolute reduction in scatter radiation was at least 90%. Thus RPSs are highly efficient and provide protection for the whole body, including the eye lenses. Nonetheless, a position close to and towards the center of the RPS should be considered to avoid tertiary scatter from nearby walls and the ceiling.25 It should, however, be emphasized that this effect reduces the protection of an RPS by no more than 1% compared with using no RPS. Moreover, standing further behind an RPS will reduce exposure, as dictated by the inverse square law.
Limitations
In this study, we found a significant difference in the scatter dose between hCBCT and oCBCT. This is explained by differences in the machine design and imaging protocols used by the different devices. It should be noted that by adjusting the imaging protocols, the differences observed in the scatter dose could potentially be reduced, although possibly at the expense of the image quality. It is possible that adjustments of protocols can be performed to address these differences. In addition, medical imaging is performed to produce relevant diagnostic information and, arguably, doses should be compared based on producing a similar image quality. Neither of these aspects were considered in this study. Instead, as a starting point, we used the equipment adhering to the product recommendations as we perceive it being used in clinical routine.
Conclusions
In this setting, the hCBCT produced lower occupational radiation exposure than the oCBCT. A possible explanation is that the hCBCT uses automatic exposure control. These differences between equipment used with standard settings should be considered when optimizing protocols for intraoperative imaging. For 3D image guided spine procedures, occupational radiation exposure can be minimized by optimal staff positioning, considering the distance to the scatter source and the staff’s position relative to the RPS. In this setting and workflow, staff can use an RPS instead of heavy aprons during intraoperative CBCT imaging to achieve effective whole body dose reduction with improved comfort.
Supplemental material
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors Study design: all authors. Data collection: PC, RV, and AO. Statistical analysis: PC, RV, AO, and EE. Data interpretation: all authors. Draft of manuscript: PC. Critically revising the manuscript for important intellectual content: all authors. Final approval of the version to be published: all authors. All authors agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. Study supervision and guarantor: AE-T.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.