Article Text

Abstract
Background Endovascular therapy (EVT) is effective and safe in patients with tandem occlusion. The benefit of intravenous thrombolysis (IVT) prior to EVT in acute tandem occlusion is debatable.
Objective To compare EVT alone with EVT plus IVT in patients with acute ischemic stroke due to anterior circulation tandem occlusions.
Methods This is an individual patient pooled analysis of the Thrombectomy In TANdem lesions (TITAN) and Endovascular Treatment in Ischemic Stroke (ETIS) Registries. Patients were divided into two groups based on prior IVT treatment: (1) IVT+ group, which included patients who received IVT prior to EVT, (2) IVT− group, which included patients who did not receive IVT prior to EVT. Propensity score (inverse probability of treatment weighting (IPTW)) was used to reduce baseline between-group differences. The primary outcome was favorable outcome—that is, modified Rankin Scale (mRS) score 0 to 2 at 90 days.
Results Overall, 602 consecutive patients with an acute stroke with tandem occlusion were included (380 and 222 in the bridging therapy and EVT alone groups, respectively). Onset to imaging time was shorter in the IVT+ group (median 103 vs 140 min). In contrast, imaging to puncture time was longer in the IVT+ group (median 107 vs 91 min). In IPTW analysis, the IVT+ group had higher odds of favorable outcome, excellent outcome (90-day mRS score 0–1), and successful reperfusion (modified Thrombolysis in Cerebral Infarction score 2b/3 at the end of EVT). There was no difference in the risk of significant hemorrhagic complications between groups. In secondary analysis of patients treated with acute cervical internal carotid artery stenting, bridging therapy was associated with higher odds of favorable outcome and lower odds of mortality at 90 days.
Conclusions Our results suggest that bridging therapy in patients with acute ischemic stroke due to anterior tandem occlusion is safe and may improve functional outcome, even in the setting of acute cervical internal carotid artery stenting during EVT.
- stroke
- hemorrhage
- thrombectomy
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Statistics from Altmetric.com
Introduction
Anterior circulation tandem occlusions accounts for 15–20% of large vessel occlusion strokes.1 2 Endovascular treatment (EVT) is effective and safe treatment for tandem occlusion and provides a high rate of successful reperfusion and functional independence.3 The benefit of intravenous thrombolysis (IVT) prior to EVT in tandem occlusion is debatable because of the large clot burden and the potential need for periprocedural antiplatelet therapy in cases of acute carotid artery stenting.2–4 Multiple studies evaluated the benefit of IVT prior to EVT and reported conflicting results.5–9 Two randomized trial demonstrated the non-inferiority of EVT alone compared with bridging therapy,10 11 but another failed to demonstrate similar findings.12 Tandem occlusion was either under-represented or excluded from previous studies.10–12
In view of a lack of sufficient evidence for the benefit and safety of bridging therapy in tandem occlusions, we aimed in this study to compare the functional and safety outcomes of patients with tandem occlusion treated with bridging therapy with those treated with EVT alone, using data from two large stroke multicenter registries.
Methods
Study cohort
This is a pooled analysis of the Thrombectomy In TANdem lesions (TITAN) and Endovascular Treatment in Ischemic Stroke (ETIS) Registries. Details of the TITAN3 13–15 and ETIS16 Registries have been reported previously. In brief, ETIS (NCT03776877) is an ongoing prospective multicenter observational registry that enrolls patients treated with EVT at six comprehensive stroke centers in France. TITAN pooled individual patients’ data for patients with tandem occlusions treated with EVT at 18 comprehensive stroke centers across Europe and the United States. In the TITAN Registry, tandem occlusion was defined as a proximal intracranial occlusion (distal intracranial carotid artery or M1-M2 segments of the middle cerebral artery) and a cervical internal carotid artery (ICA) lesion (complete occlusion or stenosis ≥90% North American Symptomatic Carotid Endarterectomy Trial). In the ETIS Registry, tandem occlusion was defined as a proximal intracranial occlusion (distal intracranial carotid artery or M1-M2 segments of the middle cerebral artery) and a cervical ICA steno-occlusion (complete occlusion or >0.70% stenosis). All patients received EVT for the intracranial lesion with and without cervical ICA lesion treatment. Cervical ICA lesion treatment options included carotid artery stenting with and without angioplasty, angioplasty alone, or no intervention. The choice of cervical ICA lesion treatment was left to the operators’ preference. Eligible patients received IVT according to the American Heart Association/American Stroke Association guidelines. Patients were divided into two groups based on IVT treatment: (1) IVT+ group, which included patients who received IVT prior to EVT, (2) IVT− group, which included patients who did not receive IVT prior to EVT. There was no standardized selection protocol for EVT treatment and patients were selected for EVT based on the participating center’s protocol.
Outcomes
The primary result for the study is favorable outcome, which is defined as 90-day modified Rankin scale (mRS) score 0–2. Ninety days after the acute event, functional outcome was assessed by a board-certified vascular neurologist during a routinely scheduled clinical visit or by a nurse certified in administering the mRS during a standardized telephone interview if the patient was unable to attend.
The secondary results include excellent outcome (90-day mRS score 0–1), angiographic outcomes, safety outcomes, National Institute of Health Stroke Scale (NIHSS) score shift, and infarct extension. Safety outcomes include 90-day mortality (mRS score 6), parenchymal hemorrhage type 2 (PH2), and symptomatic intracranial hemorrhage (sICH). PH2 and sICH are defined according to European Collaborative Acute Stroke Study (ECASS) criteria.17 Angiographic outcomes include successful reperfusion (modified Thrombolysis in Cerebral Infarction (mTICI) 2b/3) and complete reperfusion (mTICI 3). To assess infarct extension, we calculated the change in the Alberta Stroke Program Early CT Score (ASPECTS) during the first 24 hours (24-hour ASPECTS minus admission ASPECTS).
All outcomes were reported by participating centers with no central adjudication. Data collection and analyses were approved by local institutional review boards.
Statistical analysis
Quantitative variables are reported as means (SD) for normally distributed variables or medians (IQR). Shapiro-Wilk test and histograms were used to assess normality of distributions. Patients were divided into two groups according to use or not of IVT before EVT. Baseline characteristics were described according to study groups, and the magnitude of between-group differences was assessed by calculating the absolute standardized difference; an absolute standardized difference >10% was interpreted as a meaningful difference.18 The main clinical outcomes between the study groups were compared using univariable logistic regression models and ORs were calculated for the IVT+ group compared with IVT− group as effect sizes. To reduce the effects of potential confounders in the between-group comparisons,these comparisons were done by taking into account the potential confounding factors using the inverse probability of treatment weighting (IPTW) propensity score method. IPTW was estimated using stabilized inverse propensity score as weighty in logistic regression models).19 We estimated the propensity score using a non-parsimonious multivariable logistic regression model considering study groups as dependent variable and all the variables in table 1 as covariates. Absolute standardized differences were calculated in the IPTW-adjusted cohort. Effect sizes were estimated after performing multiple imputation to handle missing data. Multiple imputation was performed using a regression switching approach (chained equations with m=10 imputations obtained) and under the missing at random assumption taking into account all variables in table 1 (including study groups and outcomes in the imputation model).20 We estimated the propensity score in each imputed dataset then calculated the IPTW-adjusted effect sizes, which were later combined using Rubin’s rules.21
Baseline characteristics according to the use of intravenous thrombolysis in overall cohort (main analysis), and in patients treated with carotid artery stenting (secondary analysis)
The main analysis included all patients, and we further performed a secondary analysis including only patients treated with carotid artery stenting during EVT. Finally, in the main analysis, to assess the heterogeneity of effect size for favorable outcome across key subgroups, we introduced a multiplicative term into the IPTW-logistic regression models. Statistical analyses were conducted using the SAS software version 9.3 (SAS Institute, Cary, North Carolina, USA) and at the two-tailed α level of 0.05.
Results
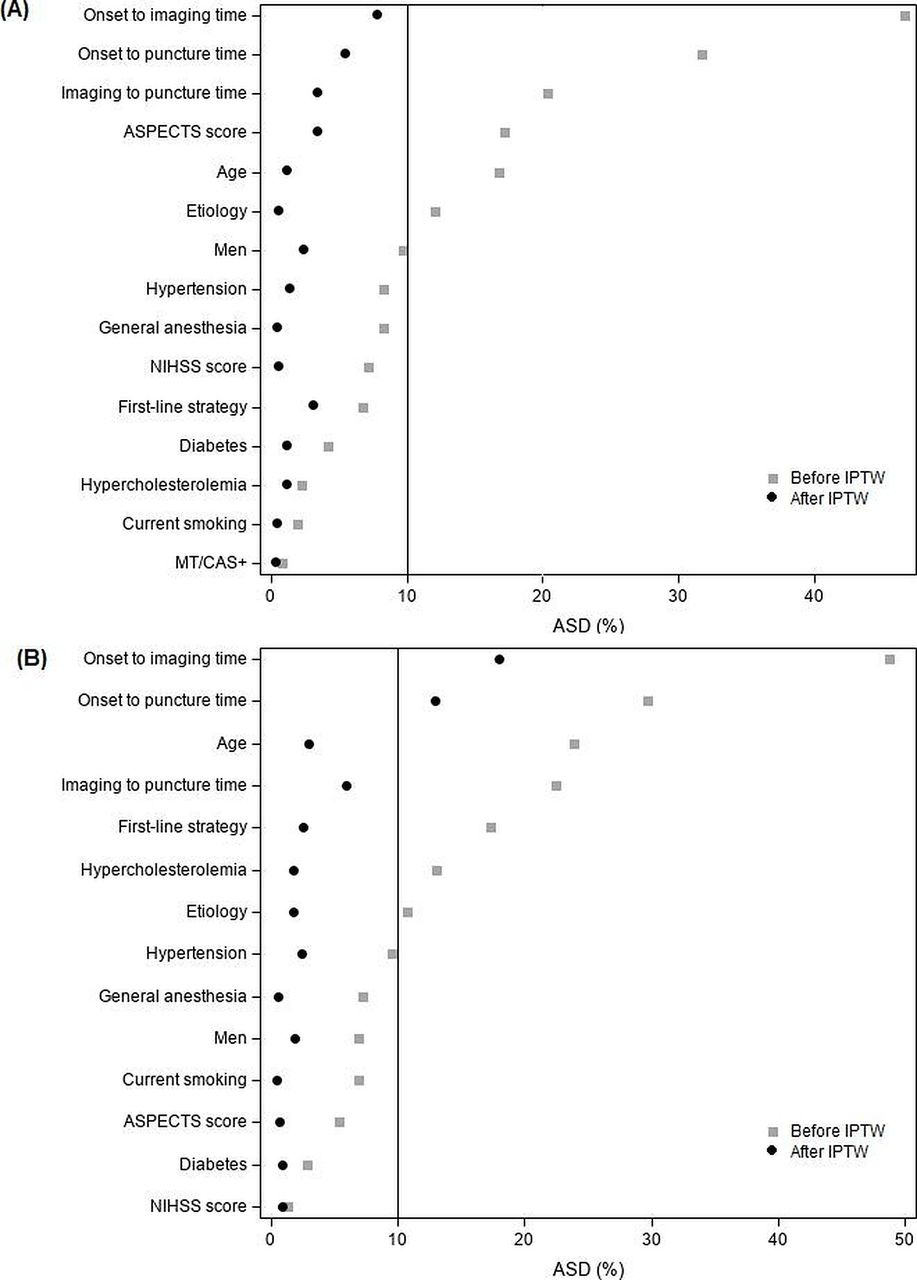
A total of 602 patients were included in the study, of whom 380 received IVT prior to EVT (IVT+) and 222 did not (IVT–). Between-group differences significantly improved with IPTW analysis (figure 1).

Baseline characteristics according to intravenous thrombolysis use in overall (A) and in patients with carotid stenting (secondary analysis) (B) before and after inverse probability of treatment weighting. ASD, absolute standardized difference; ASPECTS, Alberta Stroke Program Early CT Score; CAS, carotid artery stenting; IPTW, inverse probability of treatment weighting; MT, mechanical thrombectomy; NIHSS, National Institutes of Health Stroke Scale.
Primary analysis
In the primary analysis, all patients were included. Baseline characteristics of both groups are depicted in table 1 and online supplemental table e–1. In comparison with the IVT– group, patients in the IVT+ group were younger (mean age 62.1 vs 64.3 years), and had higher ASPECTS score (median 8 vs 7), shorter onset to imaging time (median 103 vs 140 min), and longer imaging to puncture time (median 107 vs 91 min). Stroke severity was similar between both groups (median NIHSS score 16). More patients presented within 6 hours in the IVT+ group (91.1%) than the IVT– group (69.3%). The proportion of patients with intracranial ICA occlusion was 51.3% and 47.7% in the IVT+ and IVT– groups, respectively. Cervical ICA stenting was performed in 214 (56.3%) and 126 (56.8%) patients in the IVT+ and IVT– groups, respectively. Median puncture to recanalization (or end of procedure if EVT failed) was 65 (44–91 min) and 71 (49–105 min) in the IVT+ and IVT– groups, respectively.
Supplemental material
After adjusting for baseline characteristics using IPTW propensity analyses, the IVT+ group had higher odds of favorable outcome (OR=1.1; 95% CI 1.02 to 1.20) and excellent outcome (OR=1.10; 95% CI 1.02 to 1.19) (table 2). Similarly, the IVT+ group had higher odds of successful reperfusion (OR=1.11; 95% CI 1.03 to 1.19). With respect to safety outcomes, there was no difference in the risk of sICH (OR=0.99; 95% CI 0.95 to 1.04), PH2 (OR=0.98; 95% CI 0.95 to 1.02), 90-day mortality (OR=0.96; 95% CI 0.90 to 1.01), or procedural complications (OR=0.99; 95% CI 0.94 to 1.05) between groups (table 2). There was evidence of heterogeneity according to stroke severity (NIHSS score <10 vs≥10) and the benefit of IVT was stronger in patients with moderate-severe stroke (NIHSS ≥10) (P heterogeneity =0.03) (figure 2). Outcomes before handling missing data are provided in supplemental data (online supplemental table e–2).

{kind=link}
{kind=link}
Comparisons of favorable outcome (90-day modified Rankin Scale score 0–2) rate according to intravenous thrombolysis use and key subgroups before and after inverse probability of treatment weighting. ORs were calculated after multiple imputation to handle missing values for variables included in the propensity score, The propensity score was calculated taking into account all variables in table 1. ASPECTS, Alberta Stroke Program Early CT Score; IPTW, inverse probability of treatment weighting; IVT, intravenous thrombolysis; NIHSS, National Institutes of Health Stroke Scale; p-het, P value of heterogeneity.
Comparisons of clinical and procedural outcomes according to intravenous thrombolysis use before and after inverse probability of treatment weighting in overall study sample (main analysis)
Secondary analysis
Secondary analysis included only patients treated with carotid artery stenting during EVT. Baseline characteristics are detailed in table 1. Similar to the primary analysis, patients in the IVT+ group had higher odds of favorable outcome (table 3). There was no difference in the risk of PH2 or sICH between the two groups. Also, there was no difference in the odds of successful reperfusion or excellent reperfusion between the two groups.
Comparisons of clinical and procedural outcomes according to intravenous thrombolysis use in patients treated with carotid artery stenting (secondary analysis) before and after inverse probability of treatment weighting
Discussion
In this pooled analysis of the TITAN and ETIS Registries, we compared bridging therapy with EVT alone in patients with acute ischemic stroke due to anterior circulation tandem occlusion. The main finding of this study is that bridging therapy led to higher odds of favorable functional outcome without increasing the risk of significant hemorrhagic complications, even in patients treated with acute carotid artery stenting during the endovascular procedure.
Previous observational studies comparing bridging therapy with EVT alone reported conflicting results, which created a state of uncertainty about the benefit of IVT before EVT.5–9 This clinical equipoise has led to multiple randomized controlled trials in an attempt to prove the non-inferiority of EVT alone compared with bridging therapy.10 Three of the randomized trials have already been completed and reported conflicting results. The DIRECT-MT (direct intra-arterial thrombectomy in order to revascularize acute ischemic stroke patients with large vessel occlusion efficiently in Chinese tertiary hospitals: a multicenter randomized clinical trial) trial10 compared bridging therapy with EVT alone and demonstrated that EVT alone was non-inferior to the bridging therapy for functional outcome (assessed using 90-day mRS score).10 Similar results were reported in the DEVT (direct endovascular thrombectomy vs combined IVT and endovascular thrombectomy for patients with acute large vessel occlusion in the anterior circulation) trial.11 In contrast to the previous trials, SKIP (the randomized study of endovascular therapy with vs without intravenous tissue plasminogen activator in acute stroke with ICA and M1 occlusion) trial failed to demonstrate non-inferiority of EVT alone compared with bridging therapy.12 The reason for the inconsistency in the results among the three trials is unclear, especially as the three trials had similar inclusion criteria. Tandem occlusion was under-represented in the aforementioned trials.
Tandem occlusion is a well-known predictor of poor recanalization after IVT, probably because most tandem occlusions are due to underlying atherosclerosis with a large clot burden.1 22 Moreover, carotid artery stenting is commonly performed during EVT for patients with tandem occlusions, which in turn requires acute antiplatelet therapy. For these reasons, it might be argued that IVT should be withheld in this subgroup of patients. However, pretreatment with IVT has several potential advantages, such as softening the clot and recanalizing thrombi in small distal intracranial arteries and in the microvasculature. In our study, we observed higher odds of successful reperfusion in the bridging therapy group than in the EVT alone group. The higher recanalization rate also translated to a higher rate of functional independence, and less infarct extension. The results were overall similar in a secondary analysis restricted to patients treated with carotid artery stenting. However, the difference in the successful recanalization was not significant in the secondary analysis. Our results are in line with previous analysis of the TITAN Registry, which demonstrated an association between IVT and successful reperfusion.23
One of the main concerns with the bridging approach is the risk of hemorrhagic complications. There is accumulating evidence suggesting the safety of IVT prior to EVT in large vessel occlusion strokes. In the DIRECT-MT trial, the rate of symptomatic hemorrhage was similar between the two groups. Moreover, in previous analysis of the TITAN Registry, IVT was not a predictor of parenchymal hemorrhage after EVT.24 In our study, there was no significant difference in the rate of parenchymal hemorrhage or symptomatic hemorrhage between the two groups, adding more evidence that IVT prior to EVT is safe in tandem occlusion.
Many factors might affect the response to IVT including, but not limited to, stroke etiology, stroke severity, age, and initial infarct volume. Even though, there was no evidence of heterogeneity according to stroke etiology, the effect of IVT on functional outcome was stronger in patients with extracranial carotid dissection than in patients with atherosclerosis. Procedural antiplatelets (any antiplatelets vs no antiplatelets), initial infarct volume (measured by ASPECTS), and age did not modify the effect of IVT on the functional outcome. Interestingly, there was evidence of heterogeneity according to stroke clinical severity (measured by NIHSS score), and the effect of IVT was significant only in patients with moderate-severe stroke (NIHSS score >10). This finding might be due to imbalance in the sample size between the two groups (NIHSS score ≤10, n=97 vs NIHSS score >10, n=505). Another possible explanation is that patients with a low NIHSS score and tandem occlusion have chronic occlusion with good collateral circulation and are less likely to respond to IVT.
Another important finding of this study that should be highlighted is the difference in the imaging to puncture time between the two groups; the IVT+ group had longer imaging to puncture time than the IVT− group. This is not surprising giving the time needed to initiate IVT treatment, which could delay EVT. This finding highlights the importance of taking all measures to minimize the time for IVT initiation and to shorten imaging to puncture time.
Taking all the results together, our study suggests that IVT prior to EVT is safe and potentially beneficial in tandem occlusion. However, a randomized clinical trial is needed to confirm our findings.
Limitations
This study has a number of limitations, inherent to its non-randomized observational design. First, despite the use of propensity analyses to balance the differences in baseline characteristics between the studied groups, there is still a potential risk of confounding by measured or unmeasured variables. Second, although missing data were handled using multiple imputations, it could still introduce a risk of bias in an unpredictable manner. Third, all outcomes were reported by local operators without central adjudication, which could have resulted in reporting bias. Notably, in the ETIS Registry, imaging outcomes were assessed by one senior neuroradiologist. Finally, information about periprocedural, or post-procedural antiplatelet drugs is not available in the ETIS Registry, therefore, we cannot comment on the interaction between the type, dosing, or number of antiplatelet drugs with the risk of hemorrhage after IVT.
Conclusion
Treatment with IVT before EVT for anterior circulation tandem occlusions was associated with a higher rate of functional independence and successful reperfusion without increasing the risk of hemorrhagic complications.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @marcriboj, @FishingNeurons
Collaborators TITAN (Thrombectomy In TANdem lesions) Investigators:Francis Turjman, Michel Piotin, Henrik Steglich-Arnholm, Markus Holtmannspötter, Christian Taschner, Sebastian Eiden, Diogo C. Haussen, Muhammad Waqas, Maria Boutchakova, Franziska Dorn, Monika Killer-Oberpfalzer, Salvatore Mangiafico, Marios N. Psychogios, Marc-Antoine Labeyrie, Alessandra Biondi, Serge Bracard, Jonathan Andrew Grossberg, Adrien Guenego, Julien Darcourt, Isabelle Vukasinovic, Elisa Pomero, Jason Davies, Leonardo Renieri, Corentin Hecker, Maria Muchada Muchada, Arturo Consoli, Georges Rodesch, Emmanuel Houdart, Johanna Lockau, Andreas Kastrup, Hocine Redjem, Daniel Behme, Hussain Shallwani, Maurer Christopher, Gioia Mione, Lisa Humbertjean, Nolwenn Riou-Comte, François Zhu, Anne-Laure Derelle, Liang Liao.Endovascular Treatment in Ischemic Stroke (ETIS) Investigators:Fondation Adolphe de Rothschild: Michel Piotin, Raphael Blanc, Hocine Redjem, Simon Escalard, Jean-Philippe Desilles, Gabriele Ciccio, Stanislas Smajda, Mikael Mazighi, Mikael Obadia, Candice Sabben, Ovide Corabianu, Thomas de Broucker, Didier Smadja, Sonia Alamowitch, Olivier Ille, Eric Manchon, Pierre-Yves Garcia, Guillaume Taylor, Malek Ben Maacha.Hôpital Foch: Adrien Wang, Serge Evrard, Maya Tchikviladze, Nadia Ajili, Bertrand Lapergue, David Weisenburger, Lucas Gorza, Oguzhan Coskun, Arturo Consoli, Federico Di Maria, Georges Rodesh, Morgan Leguen, Julie Gratieux, Fernando Pico, Haja Rakotoharinandrasana, Philippe Tassan, Roxanna Poll, Sylvie Marinier.CHU Bordeaux: Gaultier Marnat, Florent Gariel, Xavier Barreau, Jérôme Berge, Louis Veunac, Patrice Menegon, Igor Sibon, Ludovic Lucas, Stéphane Olindo, Pauline Renou, Sharmila Sagnier, Mathilde Poli, Sabrina Debruxelles, Thomas Tourdias, Jean-Sebastien Liegey.CHU Nantes: Romain Bourcier, Lili Detraz, Benjamin Daumas-Duport, Pierre-Louis Alexandre, Monica Roy, Cédric Lenoble, Vincent L’allinec, Jean-Baptiste Girot, Hubert Desal.CHRU-Nancy: Benjamin Gory, Isabelle Costa, Serge Bracard, René Anxionnat, Marc Braun, Anne-Laure Derelle, Romain Tonnelet, Liang Liao, François Zhu, Emmanuelle Schmitt, Sophie Planel, Sébastien Richard, Lisa Humbertjean, Gioia Mione, Jean-Christophe Lacour, Nolwenn Riou-Comte, Gabriela Hossu, Marine Beaumont, Mitchelle Bailang, Gérard Audibert, Marie Reitter, Agnès Masson, Lionel Alb, Adriana Tabarna, Marcela Voicu, Iona Podar, Madalina Brezeanu.CHU Montpellier: Vincent Costalat, Caroline Arquizan, Cyril Dargazanli, Grégory Gascou, Pierre-Henri Lefèvre, Imad Derraz, Carlos Riquelme, Nicolas Gaillard, Isabelle Mourand, Lucas Corti.
Contributors Substantial contributions to the conception or design of the work: MA, PP; RGN; AMS, AdH, BG, GM. Acquisition, analysis, and interpretation of the data for the work: MK, JL, AC, RBo, AHS, MR, IS, CD, CA, CC, JMO, RA, GA,GM, MM, RBl, BL, SR. Drafting the work or revising it critically for important intellectual content: MA; RGN; AdH, BG, UF.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests AMS reports support from Penumbra, Stryker, Medtronic; and consulting fees from: Terumo, Stryker, Penumbra, Siemens. BL reports grants from Stryker, Penumbra, and Microvention. MM reports personal fees from Acticor Biotech, Air liquide, Amgen, and Boerhinger. RGN: principal investigator, Stryker Neurovascular (DAWN trial (no compensation), Trevo-2 trial), Cerenovus/Neuravi (ENDOLOW trial, no compensation); consultant to Stryker Neurovascular; steering committee member, Stryker Neurovascular(no compensation), Medtronic (SWIFT trial, SWIFT Prime trial (no compensation)), Cerenovus/Neuravi (ARISE-2 trial, no compensation); angiographic core lab, Medtronic (STAR trial); executive committee member, Penumbra (no compensation); physician advisory board, Cerenovus/Neuravi, Phenox, Anaconda, Genentech, Biogen, Prolong Pharmaceuticals, Allm Inc.(no compensation), Viz-AI (stock options). AHS: financial interest/investor/stock options/ownership: Amnis Therapeutics, Apama Medical,Blink TBI, Inc., Buffalo Technology Partners, Inc., Cardinal Health, Cerebrotech Medical Systems, Inc., Claret Medical, Cognition Medical, Endostream Medical, Ltd., Imperative Care, International Medical Distribution Partners, Rebound Therapeutics Corp., Silk Road Medical, StimMed, Synchron, Three Rivers Medical, Inc., Viseon Spine, Inc; consultant/advisory board: Amnis Therapeutics, Boston Scientific, Canon Medical Systems USA, Inc., Cerebrotech Medical Systems, Inc., Cerenovus, Claret Medical, Corindus, Inc., Endostream Medical, Ltd., Guidepoint 15Global Consulting, Imperative Care, Integra, Medtronic, MicroVention, Northwest University—DSMB Chair for HEAT Trial, Penumbra, Rapid Medical, Rebound Therapeutics Corp., Silk Road Medical, StimMed, Stryker, Three Rivers Medical, Inc.,VasSol, W.L. Gore & Associates; national PI/steering committees: Cerenovus LARGE Trial and ARISE II Trial, Medtronic SWIFTPRIME and SWIFT DIRECT Trials, MicroVention FRED Trial & CONFIDENCE Study, MUSC POSITIVE Trial,Penumbra 3D Separator Trial, COMPASS Trial, INVEST Trial; principal investigator: Cummings Foundation grant.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.