Article Text

Abstract
Background Survival for glioblastoma remains very poor despite decades of research, with a 5-year survival of only 5%. The technological improvements that have revolutionized treatment of ischemic stroke and brain aneurysms have great potential in providing more precise and selective delivery of cancer therapeutic agents to brain tumors.
Methods We describe for the first time the use of perfusion guidance to enhance the precision of endovascular super-selective intra-arterial (ESIA) infusions of mesenchymal stem cells loaded with Delta-24 (MSC-D24) in the treatment of glioblastoma (NCT 03896568).
Results MRI imaging, which best defines the location of the tumor, is co-registered and fused with the patient’s position using cone beam CT, resulting in optimal vessel selection and confirmation of targeted delivery through volumetric perfusion imaging.
Conclusions This technique of perfusion guided-ESIA injections (PG-ESIA) enhances our ability to perform targeted super-selective delivery of therapeutic agents for brain tumors.
- angiography
- brain
- intervention
- neoplasm
- tumor
Statistics from Altmetric.com
Introduction
Over 290 000 new cases of primary brain tumors are diagnosed every year.1 Glioblastoma (GBM) is the most common and most aggressive. Survival for GBM remains very poor despite decades of research, with a 5-year survival of only 5%.2 The technological improvements that have revolutionized treatment of ischemic stroke and brain aneurysms have great potential in providing more precise and selective delivery of cancer therapeutic agents to brain tumors. Endovascular super-selective intra-arterial (ESIA) catheterization and infusion leads to over 100-fold increases in concentration of therapeutic agents in the brain compared with intravenous delivery.3 Intra-arterial (IA) delivery of avastin4 has been investigated for GBM, and ESIA delivery of mesenchymal stem cells loaded with an oncolytic adenovirus (MSC-D24) is currently under investigation (NCT 03896568). IA delivery of Yittrium-905 has also been proposed as a possible therapeutic strategy for brain tumors. Unfortunately, the exact vascular supply to GBM can be difficult to localize on angiography alone because of the variable vascularity of these tumors.6 By merging preoperative anatomic MR images with real-time perfusion images from super-selective injection during angiography, we can precisely identify the vascular supply to brain tumors and facilitate ESIA infusion for brain tumor treatment.
We describe for the first time the use of perfusion guidance to enhance the precision of ESIA infusions using, as an example, infusion of MSC-D24 in the treatment of GBM (NCT 03896568). This technique of perfusion guided-ESIA injections (PG-ESIA) enhances our ability to perform targeted super-selective delivery of therapeutic agents for brain tumors.
Methods
General strategy
MRI is ideal for defining the anatomic location of GBM, particularly the contrast-enhancing portion of the tumor, which histologically contains tumor cells and microvascular proliferation and often has a partially disrupted blood brain barrier (BBB). The contrast-enhancing portion of GBM is typically the desired target when delivering agents intra-arterially because of BBB disruption. During ESIA infusions, cerebral angiography is performed in order to help identify the vessels feeding the tumor, especially the enhancing portion. Traditionally, cerebral angiography defines the tumor based on the presence of a vascular blush, which is often not present or only faintly present in recurrent GBM cases after radiation and chemotherapy.6 As a result, we designed an optimal angiography-based infusion strategy that would benefit from fusing the preoperative MRI scan with real-time perfusion images from super-selective injection during angiography.
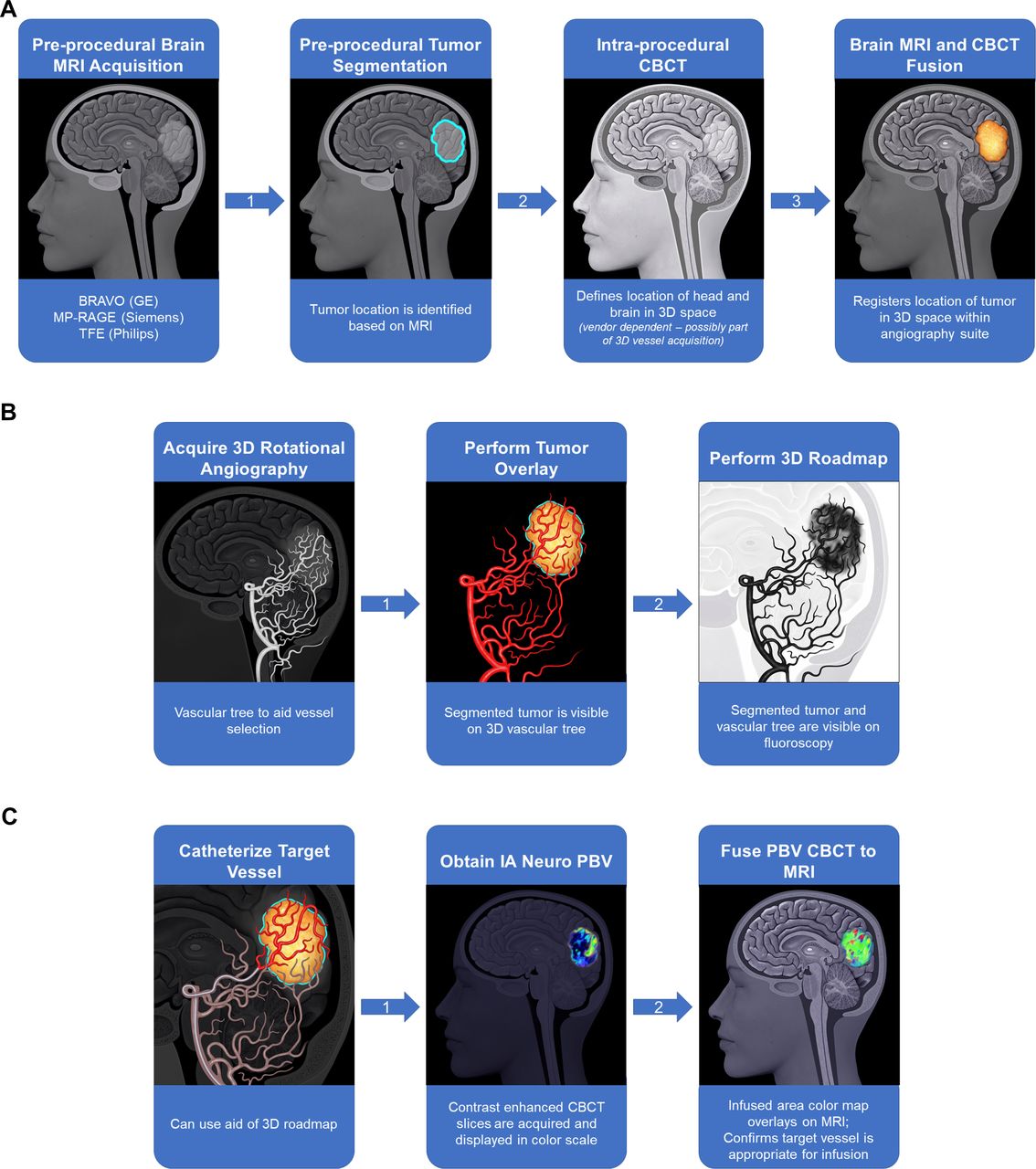
Our workflow from real-time three-dimensional vessel–MR fusion to microcatheter-based perfusion–MR fusion and perfusion volume analysis is shown in figure 1.

Workflow of perfusion-guided endovascular super-selective intra-arterial infusion. (A) Fusion of patient position with MRI. (B) Three-dimensional (3D) overlay for vessel selection. (C) Fusion of parenchymal bloodvolume (PBV) and MRI.
Preoperative MRI
Prior to angiography MRI brain with contrast is obtained to accurately identify the contrast-enhancing portion of the tumor. In order to map the vascular supply to the contrast-enhancing portion of a GBM, the MR images are fused to the angiographic images. To optimally fuse the MRI data to the data acquired in the angiography suite, isotropic data with voxels of equal dimensions on each side should be obtained during the MRI acquisition. A variety of high resolution 1 mm voxel three-dimensional (3D) ultra-fast spoiled gradient echo or 3D fast spine echo acquisition techniques are available across multiple vendors and all provide the necessary isotropic data. We include T1 post-contrast 3D BRAVO, brain volume imaging (General Electric, Milwaukee, Wisconsin, USA) as part of the protocol, which we have found to be optimal for multiplanar reformatting and fusion to the angiographic data. To perform the fusion we use syngo Fusion (Siemens Medical Solutions, Erlangen, Germany). Manual segmentation of the tumor volume from the MRI is performed and the 3D image of the tumor volume can be superimposed on real-time fluoroscopic images during the procedure. To save time during the procedure, segmentation of the tumor volume can be performed in advance.
3D space acquisition
Cone beam computed tomography (CBCT) is integral in planning IA injection and confirming the area of infusion. Unlike traditional CT with a thin fan beam from a high-dose x-ray source, CBCT uses a lower dose x-ray source which projects a cone of x-ray that is detected with the fluoroscopy image intensifier.7 The ability to obtain CBCT in the angiography suite with fluoroscopy allows us to precisely define the 3D location of the patient’s head within the angiography suite for 3D overlay and to obtain cross-sectional volumetric maps of the portion of brain infused by the microcatheter.
3D fusion and vessel selection
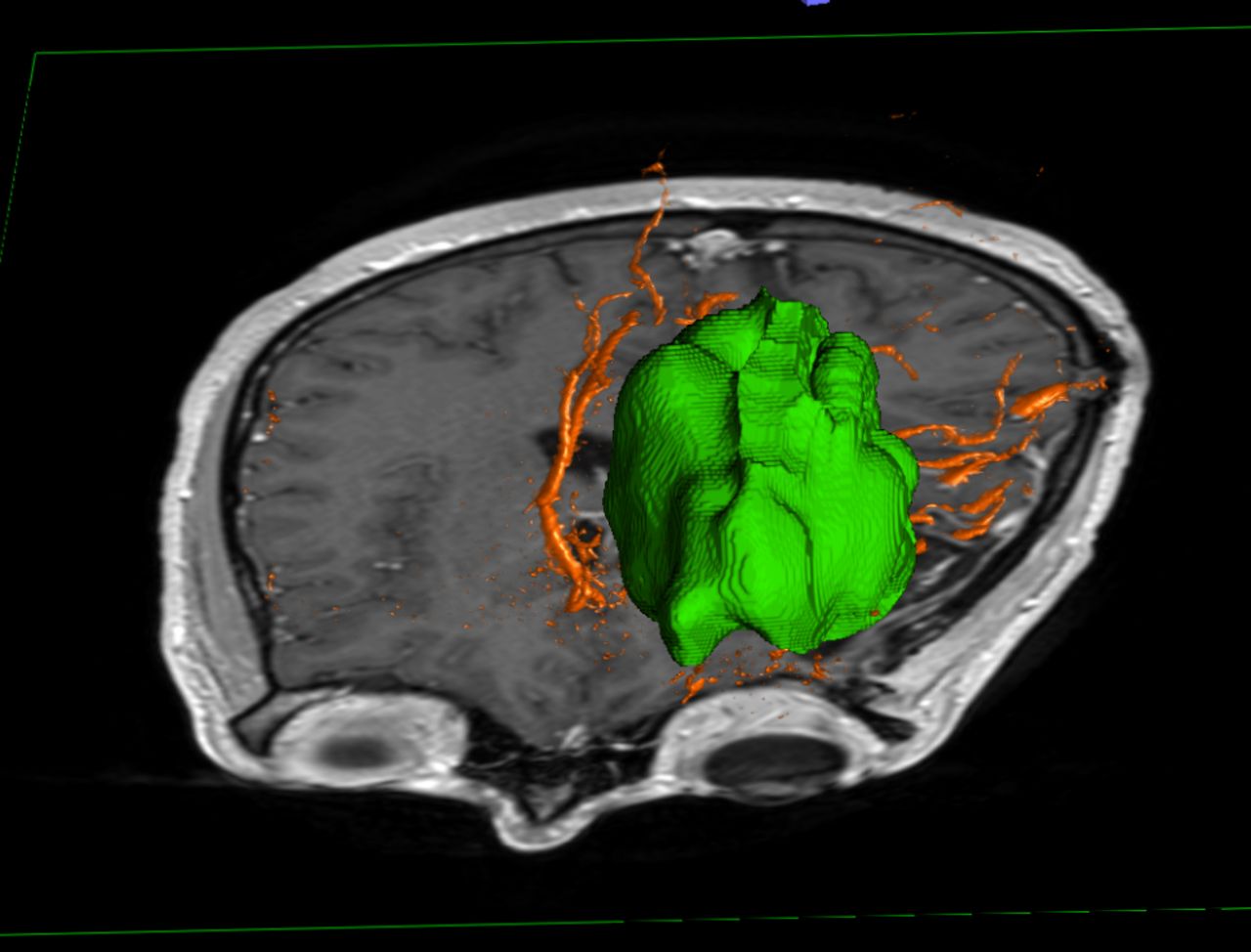
For tumors in the frontal and parietal lobes we acquire initial angiographic injections of the internal carotid artery and for temporal and occipital tumors we perform injections of the vertebral artery. Minimal additional time is needed to perform the 3D fusion. A single rotational 3D DSA (Siemens Medical Solutions, Erlangen, Germany) acquisition includes both a non-contrast mask CBCT and then an arterial phase post-contrast CBCT. On units that can spin both anteroposterior and lateral planes, the acquisition should only take 8–10 s for two rotations. This single angiographic acquisition contains the information needed to automatically register and fuse the data from the brain MRI to the fluoroscopic images. In addition, this rotational angiographic acquisition creates a 3D rendering of the vascular tree. Since both the 3D vascular tree and the tumor volume can be directly superimposed in real time on the fluoroscopic image, it aids in the precise selection of potential target vessels for therapeutic infusion (figure 2). The vessels are fused to the MRI and the 3D representation of the tumor with a process that uses the non-contrast CBCT to perform the fusion with the MRI (figure 3). Once the appropriate branch is identified, the 3D DSA is then used for a 3D Roadmap (Siemens Medical Solutions) which overlays the 3D vascular tree on the fluoroscopic images to aid in vessel catheterization. After the vessel is catheterized, angiography can confirm the tumor blush. However, in many cases no visible tumor blush can be identified, which is very common in recurrent GBM. For those patients, selection of the dominant arterial pedicle for infusion is based on the vessel penetrating and supplying most of the tumor.

Illustrative case 1. Patient with temporal-occipital glioblastoma. Fluoroscopic overlay fusion of three-dimensional (3D) vasculature/vertebrobasilar system from a left vertebral injection and 3D tumor volume. (A) Lateral. (B) Anteroposterior.

Illustrative case 2. Patient with left frontal lobe glioma. Fusion of three-dimensional (3D) DSA with MRI multiplanar reformation (MPR) overlay and 3D tumor volume overlay that aids in the selection of the proper target branch for infusion.
Infusion area 3D acquisition and image fusion
Once the microcatheter has been advanced to the potential tumor-supplying arterial pedicle based on the 3D fusion, we use a technique using the Neuro Parenchymal Blood Volume (Neuro PBV; Siemens Medical Solutions) to confirm the catheter is in a favorable location for tumor treatment. Previously, Neuro PBV has been used with IV contrast to estimate cerebral blood volume (CBV) in patients with ischemic stroke.8 Instead, we use the Neuro PBV following an IA contrast injection through the microcatheter. Similar to the previously described technique to assess CBV, the contrast enhanced CBCT is used to generate a colorized PBV map. However, the map obtained is not one of whole brain CBV but rather the area of brain parenchyma supplied by the catheterized arterial pedicle.
The injection parameters will depend on many variables including cardiac output and size of infusion area and contrast used. Our current injection rate is 1 mL/s for Visipaque 320 (GE Healthcare, Chicago, Illinois, USA) for 5 s. Acquisition is a 5 s rotation for the non-contrast CBCT followed by a 5 s rotation parenchymal phase CBCT with a 7 s x-ray acquisition delay after start of contrast injection to allow for parenchymal opacification. This results in an immediate volumetric map of the area that would be infused by the microcatheter. The non-contrast CBCT is used to fuse the MRI volume and the registration data are used to overlay the subtracted PBV CBCT. This fusion confirms that the tumor is within the area of infusion (figures 4 and 5). The entire process takes only several minutes at most and adds little additional time intra-procedurally over blind infusion in proximal vessels.

Illustrative case 1 showing result after fusion of parenchymal blood volume (PBV) and MRI in a patient with temporal-occipital glioblastoma and posterior cerebral artery infusion.
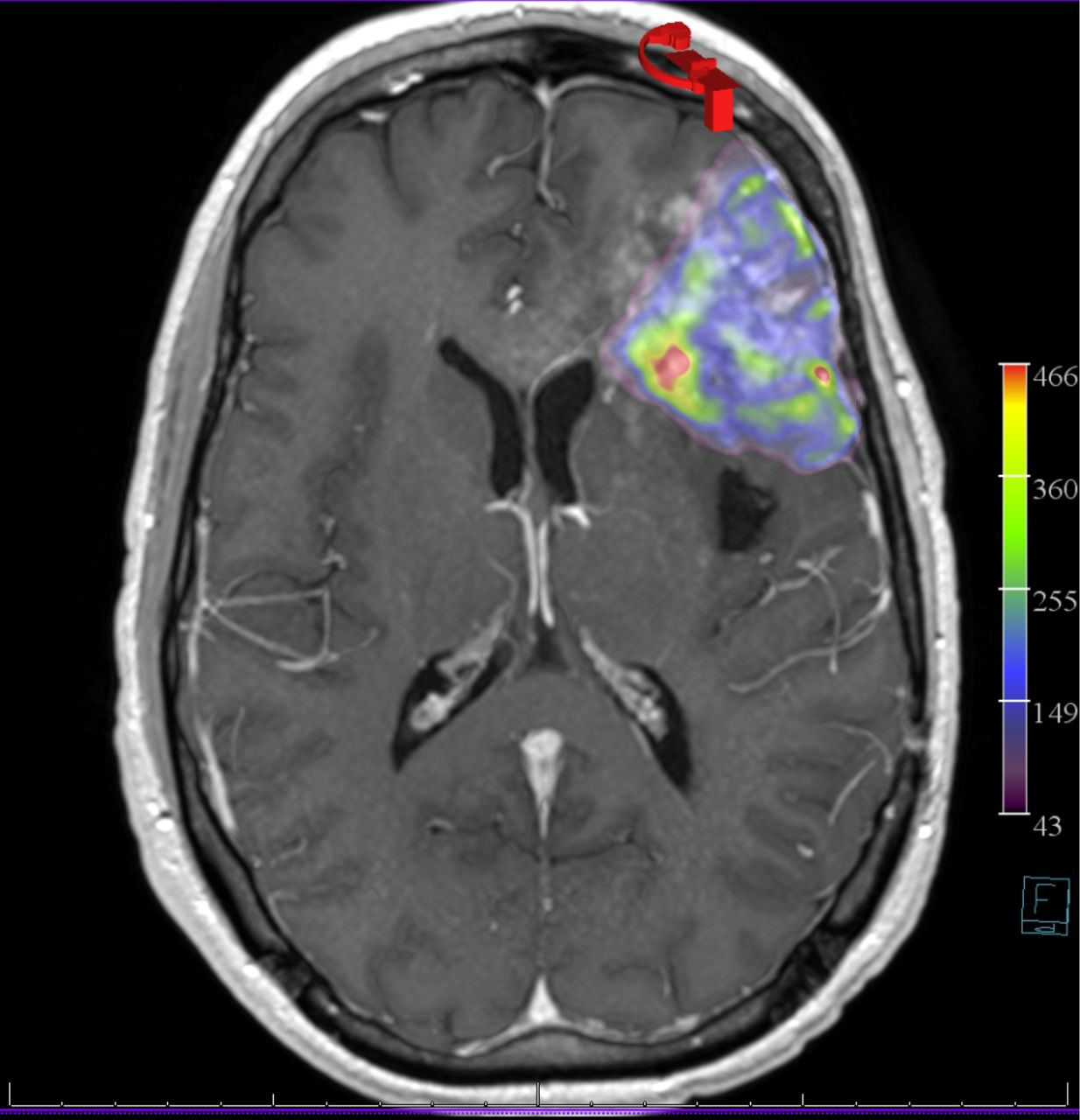
Illustrative case 2 showing fusion of parenchymal blood volume (PBV) generated from a microcatheter injection from a left pre-frontal middle cerebral artery branch with contrast-enhanced MRI in a patient with a left frontal lobe glioblastoma and sub-selective middle cerebral artery infusion of a pre-frontal branch.
Infusion area volume analysis
The MRI and PBV map can be exported to MIM 6.0 (MIM Software, Beachwood, Ohio, USA) to calculate the precise volume of the infused area. This software platform is commonly used by radiation oncology, nuclear medicine, and interventional radiology. MIM allows for automatic fusion of the PBV to the MRI volume without significant manual correction. It uses a landmark-based deformation algorithm that registers each volume to a standard template for fusion. As MIM is commonly used on positron emission tomography (PET) data, it will perform fusion without the non-contrast CBCT source data. The software also performs rapid semi-automated segmentation of the infused area. The PET Edge (MIM Software) gradient-based segmentation tool is very effective in rapidly defining the area of infusion from the PBV map. 3D sculpting tools can be used to refine the edges.
Illustrative cases
Illustrative case 1
A patient in their 40s who presented with left occipital recurrent GBM (figure 6A) underwent MSC-D24 infusion (2×107 cells in 20 mL) through the left posterior cerebral artery (PCA) (figure 6B) as part of a phase I clinical trial (NCT 03896568). The perfusion location and volume from the microcatheter in the PCA were shown (figure 7).

Illustrative case 1. (A) Axial MRI T1 with contrast showing an enhancing left temporal-occipital tumor. (B) Selective left posterior cerebral artery injection through the arterial pedicle supplying the temporal-occipital tumor. Note the lack of tumor blush.

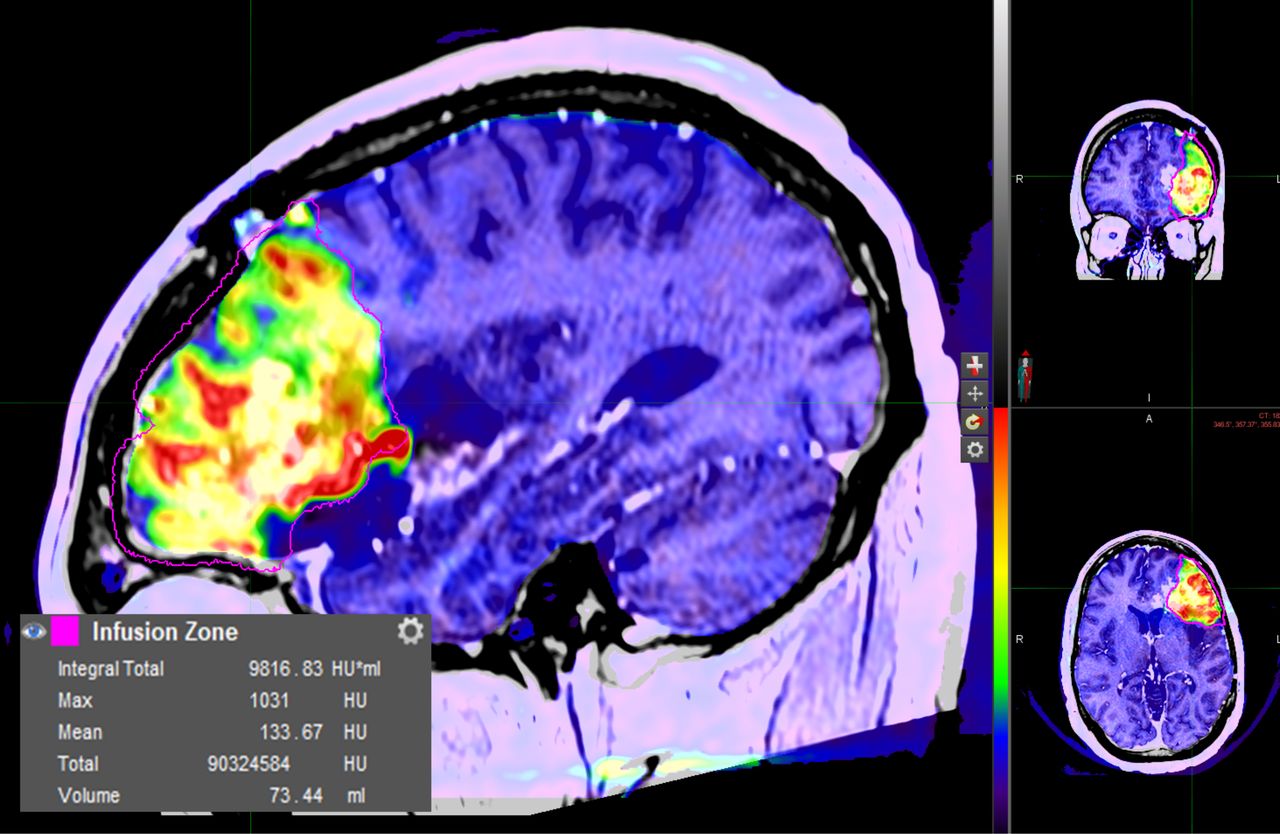
Infusion area volume analysis from illustrative case 1 showing the calculated volume of the infused area. Infused area from the microcatheter (color parenchymal blood volume (PBV) map generated from cone beam computed tomography (CBCT) with contrast injection through the microcatheter). Calculated infusion volume using the MIM Software after PBV map generation. Edge of the tumor defined by PET Edge segmentation tool of the MIM Software.
Illustrative case 2
A patient in their 30s who presented with left frontal recurrent glioblastoma (figure 8A) underwent MSC-D24 infusion (2×107 cells in 20 mL) through the left middle cerebral artery (MCA) (figure 8B) pre-frontal branch as part of a phase I clinical trial (NCT 03896568). The perfusion location and volume from the microcatheter in the MCA were shown (figure 9).

Illustrative case 2. (A) Axial MRI T1 with contrast showing an enhancing left frontal tumor. (B) Selective left middle cerebral artery injection through the pre-frontal branch supplying the frontal tumor. Note again the lack of tumor blush.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Infusion area volume analysis from illustrative case 2 with recurrent left frontal glioblastoma showing the calculated volume of the infused area. Infused area from the microcatheter (color parenchymal blood volume (PBV) map generated from cone beam computed tomography with contrast injection through the microcatheter). Calculated infusion volume using the MIM Software after PBV map generation. Edge of the tumor defined by PET Edge segmentation tool of the MIM Software.
Discussion
In this report we show for the first time that, by merging preoperative MR images with real-time angiographic perfusion images from super-selective microcatheter injections, we can more precisely identify the arterial pedicle to GBM and verify that the perfused territory overlaps the tumor volume. This perfusion-guided ESIA approach makes possible highly targeted super-selective delivery of therapeutic agents for brain tumors, such as MSC-D24, as shown in our illustrative cases.
IA therapy has been successful in treating several cancers4 6 but has had limited success in the treatment of GBM. However, with the advent of stem cell-based therapies for GBM whose effectiveness depends on IA delivery (IV infusion results in pulmonary sequestration), and with the emergence of modern microcatheters that allow access to distal vessels, ESIA infusion has re-emerged as a potential strategy for delivering agents directly into the vascular bed of brain tumors. In the past, the clinical application of IA therapy for brain tumors was limited, at least in part, by neurotoxicity and ocular toxicity, which were largely a result of non-selective infusion of therapeutic agents (typically chemotherapy) into the proximal internal carotid or vertebral arteries resulting in exposure of non-tumoral normal neural tissues to the adverse effects of the therapeutic agents.5 9
With the technological improvements in microcatheters, we are now able to inject agents into the most distal intracranial arterial pedicles supplying the tumor, thereby minimizing exposure of normal brain tissue and maximizing the concentration of therapeutics delivered to the tumor. However, the exact arterial pedicle supply to GBM can be difficult to localize on angiography alone because of variable vascularity of such tumors, particularly in the recurrent setting where a tumor blush is often not found. Indeed, tumors that have received prior radiation often do not have a tumor blush.10 As a result, perfusion maps generated using CBCT during angiography with microcatheters optimize the precision of intracranial IA delivery, ensuring that the therapeutic is delivered to the tumor, sparing normal brain parenchyma. Additionally, the perfusion volume can also be easily calculated and exported for further analysis. This is important if dose calculations for volume infused become an important consideration for a therapeutic agent.
Both Delta-24-RGD, a tumor selective oncolytic adenovirus, and Yttrium-90 microspheres (Y90), a radiation beta emitter, have been proposed to be potentially new IA agents for treatment of GBM. A recent clinical trial showed Delta-24 replicated in human tumors and induced cell death in GBM through direct tumor cell lysis, expression of toxic proteins and inducing a CD8 T cell anti-tumor immune response after direct intratumoral injection.10 With Delta-24 IA infusion, our goal is for it to replicate through the tumor, thus potentially distributing the adenovirus more widely beyond the enhancing tumor portion initially targeted. The anti-tumor response generated can also target the non-enhancing portion of the tumor. Prior studies have shown that human bone marrow-derived MSCs can home to gliomas11 and be successfully loaded with Delta-24 (MSC-D24) for IA delivery.9
Yttrium-90 microspheres are 25–35 micron glass or resin spheres that can deliver lethal doses of radiation. Each sphere delivers 90% of radiation dose within 5 mm and 11 days. IA delivery of Y90, radio-embolization, has primarily been used for oncologic therapies within the liver including hepatocellular carcinoma, metastatic colorectal carcinoma, metastatic neuroendocrine carcinoma and metastatic biliary carcinoma. Use of Y90 outside the liver has been extremely limited. Recently, a canine model demonstrated successful selective arterial microcatheter delivery of Y90 with up to 69% size reduction seen in canine brain tumors.5
The process for radio-embolization of liver tumors involves conventional catheter angiography for treatment planning weeks in advance. During planning, a surrogate radiopharmaceutical, 99mTechnetium-macroagreggated albumin (Tc-MMA), is delivered to verify uptake in tumor, to determine the amount of uptake in normal liver and to perform dosimetry planning. More precise doses for IA radio-embolization therapies have been shown to have improved outcomes for liver tumors.12 13 Precise dosimetry will likely be important for any clinical trials of Y90 infusion in patients with GBM.
While the precise volume of tissue infused is not currently a concern for MSC-D24 as it can replicate outside the area of infusion and should not affect normal brain since it only replicates in glioma cells, radio-embolization requires precise treatment volumes to ensure both effective therapy and to minimize toxicity. However, in general, traditional methods of calculating the therapeutic dose based on weight and body surface area are not applicable to IA therapies. For instance, Gobin et al have proposed that the IA retinoblastoma chemotherapy dose should be based on eye size, not body size.14 Dose escalation studies for IA drug efficacy and toxicity may need to be based on tumor size and volume of brain that is being infused rather than simply the patient’s weight or body surface area for more predictable outcomes.
The limits of this approach are that the precise perfusion volume cannot be predicted pre-procedurally without selective intracranial catheterization. While a separate diagnostic angiogram for mapping is common for liver radio-embolization, it may not be reasonable for GBM therapy given the higher risks of intracranial catheterization. Potentially, our technique of using intra-procedural CBCT perfusion maps could also predict the uptake in tumor to normal brain and total treatment volume in a single session, similar to techniques described in single session hepatic radio-embolization to avoid two separate catheterizations.15
Our experience suggests that future trials of IA infusion for treatment of malignant brain tumors should be guided by fusion of pre-procedural brain MRI to intra-procedural CBCT to ensure the most optimal microcatheterization is performed. Brain MRI should be fused to microcatheter perfusion maps both to document the volume of tumor that is infused and to minimize non-target infusion in potentially dangerous territories.
Conclusion
Endovascular neurosurgical oncology is a field poised for rapid application and growth. Safe ESIA infusions for brain tumors have been made possible by advancements in microcatheter technologies. These infusions will be guided by similar advances in imaging that were not previously available to the neurointerventionalist. Volumetric acquisitions of the 3D intracranial vascular anatomy have become common. These data can be easily fused to the MRI demonstrating the exact vessels supplying brain tumors. Our report shows that perfusion volume maps generated from microcatheter infusion previously developed for stroke and liver tumor radio-embolization can be used for precise intracranial ESIA delivery of therapeutics to GBM by fusing them with the preoperative MRI using existing software tools.
Supplemental material
Ethics statements
Patient consent for publication
Ethics approval
The example cases presented were part of a clinical trial that was approved by the MD Anderson Institutional Review Board protocol # 2015–0953. The participants gave consent before taking part.
Acknowledgments
We thank Kelly Kage of the University of Texas MD Anderson Center Department of Diagnostic Imaging for help with preparation of illustrations.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @s0schen, @PeterKa80460001
Contributors SRC, PK and FFL conceived the study. SRC, MMC and PK analyzed the data. SRC, PK and CE wrote the paper.
Funding This study was supported by the National Cancer Institute (1R01CA214749, 1R01CA247970 P30CA016672 and 2P50CA127001), The University of Texas MD Anderson Moon Shots ProgramTM, The Broach Foundation for Brain Cancer Research, The Elias Family Fund, The Priscila and Jason Hiley Fund, The Baumann Family/Curefest Fund, The Jim and Pam Harris Fund, The Gene Pennebaker Brain Cancer Fund, The Schneider Memorial Cancer Research Fund, The Sweet Family Cancer Research Fund, The Dr Marnie Rose Foundation, The Gold Family Memorial Fund, and The Sorenson Foundation (all to FFL).
Competing interests SRC has received consulting fees. FFL is a patent holder and grant recipient. PK is on the editorial board of JNIS.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.