Article Text

Abstract
Traumatic cerebrovascular injuries following blunt or penetrating trauma are common and carry a high risk of permanent disability or death. Proper screening, diagnosis, and treatment of these lesions is essential to improve patient outcomes. Advances in imaging continue to improve the accuracy of non-invasive diagnosis of these injuries while new clinical data provide better evidence for optimal management, whether medical or invasive. Here, we review screening, diagnosis, and treatment of traumatic cerebrovascular injuries.
- trauma
- intervention
- dissection
- angiography
Statistics from Altmetric.com
Introduction
Patients experiencing craniocervical trauma are at risk of devastating injuries, including traumatic cerebrovascular injury and traumatic brain injury.1 2 Traumatic cerebrovascular injury occurs in 3–20% of patients following craniocervical trauma and is a frequent cause of morbidity and mortality.1 3–5 Timely diagnosis and management can prevent devastating neurological complications.5 With improvement in techniques, expertise, and evidence for endovascular interventions, neurointerventionalists play an increasingly important role in the treatment of patients with traumatic cerebrovascular injury.6–9 In this work, we provide a broad overview of the typical presentation, methods of diagnosis, appropriateness of screening, injury classification, and management of patients with known or suspected traumatic cerebrovascular injuries.
Presentation
Mechanism
Blunt trauma comprises forceful impact with a dull object or surface, as may occur in motor vehicle collisions, assaults, and contact sports injuries. Penetrating trauma comprises objects or surfaces that pierce the body, including high-velocity mechanisms such as gunshot wounds or other projectile injuries, as well as low-velocity mechanisms such as stab wounds. Low-velocity mechanisms of penetrating trauma are typically caused by direct injury along the path of the penetrating object, whereas high-velocity mechanisms may also cause injury beyond the path of penetration due to dissipation of shock waves or heat.10
Location
Since blunt trauma can affect large body regions, blunt cerebrovascular injury (BCVI) often involves multiple vessels. In both BCVI and penetrating cerebrovascular injuries (PCVI), the extracranial carotid arteries are most vulnerable,11–13 ostensibly reflecting the protection of the vertebral arteries and intracranial arteries conferred by the cervical spine and skull.14 PCVI also frequently involves the internal jugular veins or other major veins in the neck.
Timing
Primary injuries are those that are the direct and immediate result of traumatic injury. Secondary injuries are those that occur as a physiological consequence of primary injuries and might not have yet occurred at the time of presentation. Timing of secondary injuries with both BCVI and PCVI is highly variable. In BCVI, the timing of stroke has been observed at a median time of 48 hours after admission, with nearly 40% diagnosed after 72 hours.15 In PCVI, injuries adjacent to the circle of Willis and injuries involving both cerebral hemispheres are associated with earlier development of arterial injury.16
Diagnosis
Because BCVI can occur distant from the site of visible trauma, involve multiple vessels, and be asymptomatic or masked by other injuries at presentation,17 BCVI is clinically under-recognized. In contrast, PCVI is more often grossly apparent or clinically suspected.3 Imaging for diagnosis and characterization of BCVI and PCVI must balance the need for accurate diagnosis with the potential risks of delayed intervention. Catheter angiography, CT angiography (CTA), and magnetic resonance angiography (MRA) may each play a role.3 18–20
Catheter angiography
Catheter angiography provides high-resolution, dynamic imaging and is the gold standard for detection and characterization of both BCVI and PCVI.21 However, catheter angiography has a complication rate of approximately 2.9% in patients experiencing cranial trauma.3 22 Additionally, catheter angiography is more labor-intensive and time-intensive than CTA and MRA, and is less widely available. As a result, the role of catheter angiography has largely moved from its use a screening tool to a vehicle for endovascular intervention.18 However, it is important to note that shunt lesions, such as arteriovenous fistulas and carotid-cavernous fistulas, are often missed by CTA and MRA,23 24 and that catheter angiography continues to play an important role in the workup of clinically suspected fistulas (figure 1).
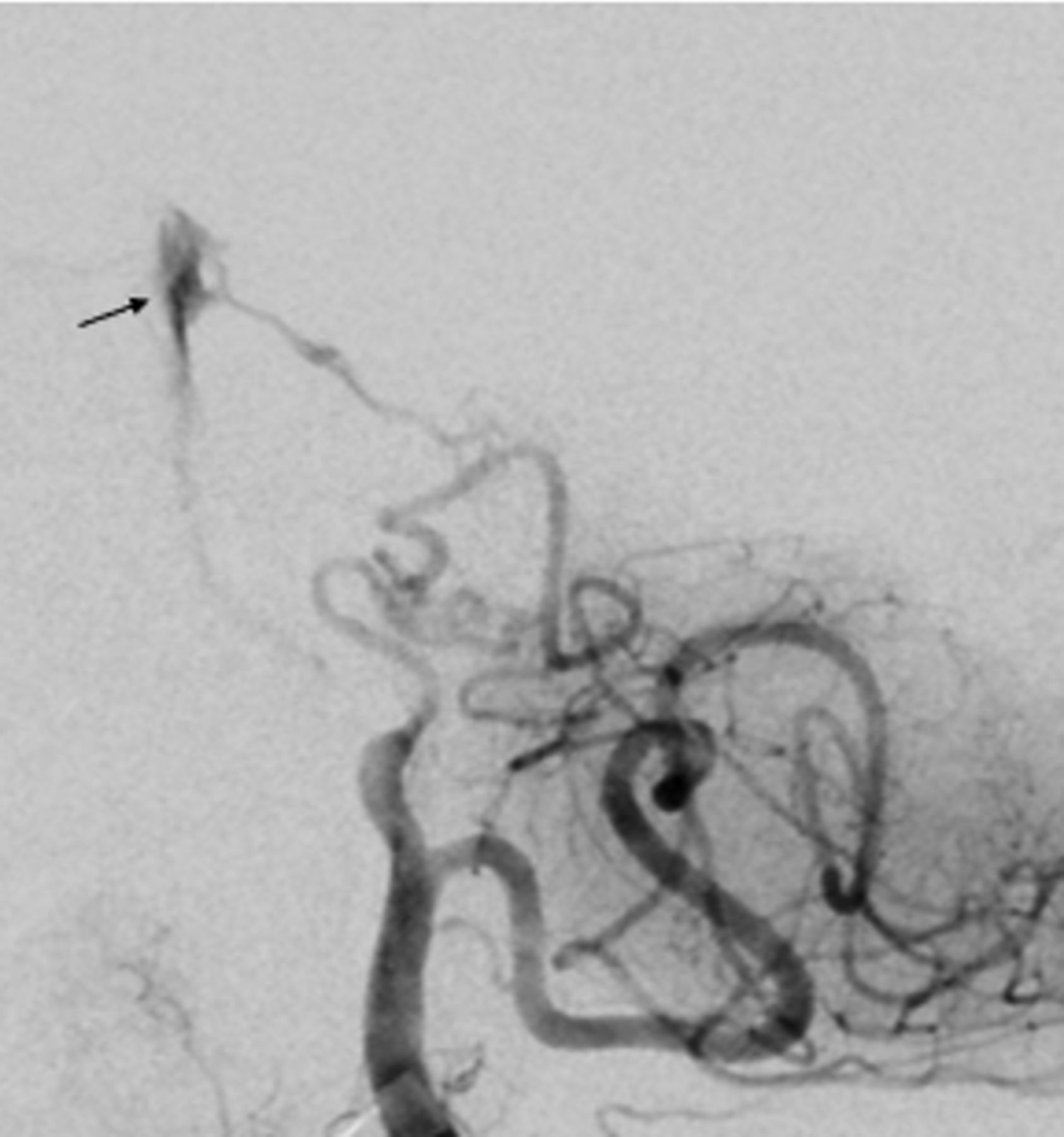
Elderly patient with multiple skull base fractures after a motor vehicle collision. Angiography demonstrated a traumatic arteriovenous fistula (arrow) from the right anterior inferior cerebellar artery to the basilar venous plexus.
Computed tomography angiography
CTA is less invasive, costly, and time-consuming than catheter angiography. The proliferation of modern multidetector row CT scanners has improved the sensitivity of CTA to subtle BCVI and PCVI,25 and the availability of CTA has benefited from its widespread use in ischemic stroke protocols.26 Although less accurate than catheter angiography for the detection of cerebrovascular injuries, CTA performed on modern scanners demonstrates high sensitivity and specificity for both BCVI and PCVI.3 27 In a study of patients with BCVI, 4.5% of patients with positive CTA findings later experienced ischemic stroke, while only 0.5% of those with negative CTA findings experienced ischemic stroke.9 Therefore, first-line screening with CTA can quickly and easily provide information critical for subsequent management.
Magnetic resonance angiography
Like CTA, MRA has improved considerably in quality and availability in recent years.28 Despite having similar diagnostic performance to CTA, it is not generally favored for initial assessment of patients with suspected BCVI or PCVI. Victims of trauma might have retained metal foreign bodies that are unsafe in strong magnetic fields, and MRA is generally slower and less available than CTA at most centers. MRA is also more affected by patient movement, which can be difficult to control in cases of trauma. MRI and MRA may be more useful for targeted questions that are difficult to characterize with other modalities, such as identifying intramural hematoma.3
When to image
Current guidelines for evaluation and management of BCVI by the Eastern Association for the Surgery of Trauma report an improved sensitivity to BCVI after adopting defined clinical criteria for CTA screening, but note that 5% of patients with BCVI do not meet common screening criteria.29 Another recent study identified additional risk factors associated with BCVI and PCVI, including cervical fractures, injury with involvement of the transverse foramina or carotid canal, gunshot injury, and focal neurological deficits prior to imaging.9 These studies have contributed to the widespread acceptance of defined clinical criteria to prompt CTA screening in the aftermath of trauma (Box 1).
Factors increasing the likelihood of underlying blunt cerebrovascular injury
Blunt polytrauma
Multiple cervical fractures, subluxation, or severe flexion/extension
Cervical fracture involving transverse foramen and/or carotid canal
Gunshot injury
Glasgow Coma Scale <13
Focal neurologic deficit at presentation
When not to image
Certain presenting factors may obviate imaging screening for potential BCVI or PCVI. Some minor trauma—for example, low-velocity penetrating neck injury that does not violate the platysma, isolated facial injury, and falls without fracture that are not accompanied by a focal neurological deficit—may carry low risk for underlying cerebrovascular injury.3 Imaging screening offers little value in these patients. Conversely, some critical injuries may preclude safe imaging altogether. For example, cervical arterial transection with airway compression, hypotension, or other so-called ‘hard signs’ of potentially life-threatening vascular injury (table 1) must be managed immediately in order to preserve life, and delaying this management for the sake of imaging is generally inappropriate.30 In these critical situations, imaging may be considered after immediately life-threatening injuries have been dealt with to evaluate the repair or screening for additional sites of injury. Finally, patient factors may also affect the yield of imaging. For example, diagnostic accuracy of imaging can be degraded by patient movement or the presence of metallic foreign bodies, and sedation to reduce movement may be inappropriate after recent trauma.3
Hard and soft signs of potentially life-threatening injury following penetrating cerebrovascular trauma
Classification
BCVI is classified using the five-point Biffl scale, which grades cervical vascular injuries based on the angiographic appearance of the lesion (table 2).31 This classification system was derived from a large series of blunt carotid injuries and provides valuable guidance regarding natural history, prognosis, and management for injuries of each grade. Several studies have validated the Biffl scale, which now serves as the foundation for many screening, diagnosis, and treatment algorithms for BCVI.18 19 22 32
Grading scale for blunt cerebrovascular injury. adapted from Biffl et al 22 31
PCVIs involving the neck have historically been classified based on their anatomical location as described by Roon and Christensen (table 3).33 This classification system is relevant for guiding surgical exploration, which is less widely used in the era of widespread CTA and endovascular interventions.9 A more current classification may involve discrimination of hard and soft signs of cerebrovascular injury. Unlike blunt injuries, there is no widely accepted classification system for penetrating injuries of the head.
Classification of penetrating neck trauma. adapted from Roon and Christensen33
Notably, traumatic arteriovenous fistulas have been inconsistently categorized within these classification schema. Biffl and colleagues classified small arteriovenous fistulas and hemodynamically significant arteriovenous fistulas as grade II and grade V, respectively.22 More recent literature has classified all traumatic arteriovenous fistulas as grade V.34 35 Carotid-cavernous fistulas are not specifically included in this grading.
Management
Management of trauma is largely directed towards prevention or mitigation of secondary injury. For example, the increased risk of secondary stroke with BCVI can be dramatically reduced with prompt management.34–36
Multidisciplinary coordination
Optimal management of patients experiencing cerebrovascular trauma is rarely clear cut, and a thoughtful, multidisciplinary approach is usually necessary. BCVI and PCVI often warrant immediate attention, but the management of these lesions must be considered in the context of the full spectrum of polytrauma. Decisions related to the use of antiplatelet or anticoagulant agents, for example, may be complicated by concomitant non-vascular injuries. Proper management of these patients often requires finding the proper balance between lesions that have conflicting management strategies.
One survey study demonstrated poor agreement across specialties for the management of patients with traumatic cerebrovascular injury.37 Combined with the typical need to balance management of multiple lesions, these results highlight the importance of robust communication between traumatologists, neurosurgeons, orthopedic surgeons, vascular surgeons, and other trauma specialists regarding vascular findings, non-vascular injuries, indications for treatment, and management of other injuries.
Medical management
Many BCVI lesions can be effectively managed medically without invasive intervention, though clinical trial data are lacking to support optimal management strategies.3 4 9 29 Current guidelines recommend the use of antithrombotic therapy in BCVI for reduction of secondary stroke risk.29 Early initiation of antithrombotic agents is important in patients with BCVI, and some patients may warrant prolonged antithrombotic therapy.38 However, patients with concomitant traumatic brain injury or solid organ injury may be poor candidates for antithrombotic therapy due to the risk of bleeding and hemorrhagic expansion.29
The decision between anticoagulant and antiplatelet therapy remains an area of debate.29 39 Potential benefits of anticoagulation include prevention of embolism from fresh thrombus formation, though antiplatelets may be similarly effective and carry a lower risk of hemorrhage extension. Reports indicate that therapeutic anticoagulation with vitamin K antagonists is inferior to aspirin for stroke prevention in BCVI, but the use of aspirin as monotherapy or as a component of dual antiplatelet therapy subsequent to endovascular intervention might lead to more severe bleeding in the acute post-treatment phase compared with vitamin K antagonists.3 40 41 The Cervical Artery Dissection In Stroke Study (CADISS) trial did not identify differences in recurrent stroke rate or residual vessel narrowing in a comparison of patients treated acutely with antiplatelet or anticoagulant therapy following cervical artery dissection.39 Optimal antiplatelet regimens are also difficult to derive from the CADISS trial owing to heterogeneity in the antiplatelet arm of the study. Notwithstanding the lack of clear evidence, our center typically implements medical management with aspirin monotherapy or intravenous heparin, depending on the acuity of injury, ability to tolerate oral intake, and presence of polytrauma. Other centers report implementing dual antiplatelet therapy for some forms of BCVI.
Early initiation of anticoagulation with heparin is indicated in asymptomatic patients following BCVI to prevent stroke,42 and long-term treatment may be necessary in some cases.43 Benefits of heparin anticoagulation are particularly pronounced in grade II BCVI, where progression to lesions of a higher grade is common (figure 2), and in grade IV BCVI to prevent secondary stroke.3 Unlike anticoagulation with vitamin K antagonists, anticoagulation with heparin is comparable to aspirin in lowering stroke risk and influencing injury healing rates.32 44 Antiplatelet agents are generally preferred over heparin anticoagulation for long-term treatment owing to the availability of antiplatelet drugs in oral form.
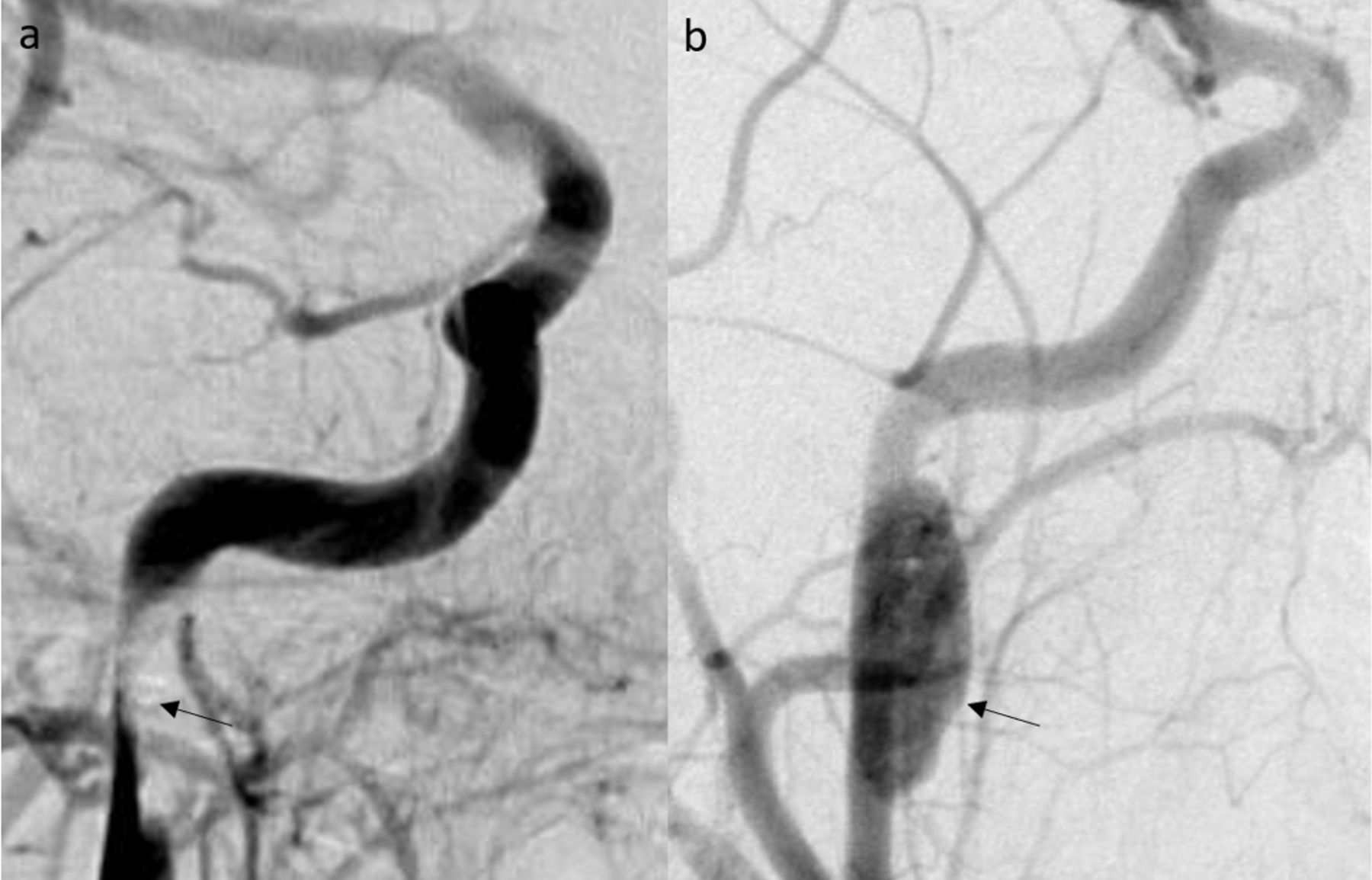
Teenage patient with multiple facial fractures after a motor vehicle accident. Angiography demonstrated dissection of the right internal cerebral artery at the petrous-cavernous junction (arrow), resulting in moderate to severe narrowing and slowing of flow (a) Angiography performed 2 months later demonstrated a 24×8 mm dissecting pseudoaneurysm (arrow) at the site of previous dissection (b).
Despite the effectiveness of medical therapy in managing lesions secondary to BCVI and PCVI, patients receiving medical therapy following cerebrovascular trauma are still at significant risk of ischemic stroke and other complications. Indeed, a study found that 22% of patients experiencing stroke following BCVI were receiving appropriate antithrombotic medication at the time of stroke, reinforcing the importance of close monitoring and escalation of care when necessary.15
Vessel reconstruction
Vessel reconstruction with endoluminal stents can be used to treat cervical arterial dissections and Biffl grade II injuries to decrease secondary stroke risk.3 No trial has demonstrated superiority of endovascular treatment over medical therapy in the setting of carotid artery dissection or vertebral artery dissection, but patients for whom medical therapy fails may warrant stenting, particularly those demonstrating persistent flow limitation or pressure-dependent neurologic symptoms.45 46 The decision to pursue stenting of Biffl grade II injuries should be performed with caution, as stenting of traumatic cervical injuries is associated with a 45% rate of vessel occlusion compared with 5% in those treated with antithrombotic agents.11 Within the narrower context of cervical artery dissection, carotid artery dissection is more likely than vertebral artery dissection to fail medical therapy and require stenting or other intervention.45 However, the antiplatelet therapy required with stents should be considered judiciously in the setting of polytrauma.3
Vessel deconstruction
Vessel deconstruction involves vascular sacrifice using coils, liquid embolic agents, or vascular plugs to stop active hemorrhage, prevent further hemorrhage, or reduce the risk of distal embolic shower (figure 3).3 Unlike stenting, vessel deconstruction via embolization does not necessarily require the use of antiplatelet agents or anticoagulation,18 though it can be helpful to prevent stump emboli. In some circumstances, embolization may be safer and faster than open surgery in critically ill patients.47 The feasibility and appropriateness of emergent endovascular therapies for trauma is likely to benefit from recent improvements in systems of care and in-hospital workflows related to endovascular thrombectomy for acute ischemic stroke.48 49

Teenage patient with uncontrolled bleeding after a gunshot wound to the right neck. Angiography demonstrated transection of the right vertebral artery (arrow) (a). Deconstruction of the right vertebral artery with coils (arrow) was successful (b).
Most vessel deconstruction procedures in patients with trauma involve arterial deconstruction, but venous deconstruction may be warranted in some patients with traumatic arteriovenous fistulas.3 50 51 Notably, some of these traumatic fistulas, especially low-flow carotid-cavernous fistulas, can resolve spontaneously. In cases with a low risk of progression and relative ease of monitoring, conservative management may be appropriate.
Pseudoaneurysm repair
Traumatic pseudoaneurysms rarely resolve without intervention, with angiographic improvement observed in only 8% of untreated pseudoaneurysms.22 Initial management may involve antithrombotic agents, but in cases where pseudoaneurysms enlarge, compress adjacent structures, or lead to embolic phenomenon, definitive treatment is usually warranted.3 Endovascular treatment of traumatic pseudoaneurysms is most commonly achieved with direct coil embolization of the pseudoaneurysm with preservation of flow in the adjacent parent artery.18 In one study, the technical success rate for embolization of traumatic pseudoaneurysms exceeded 98%.52 As a result, pseudoaneurysms are the most common variety of traumatic cerebrovascular injury treated by endovascular means (figure 4).3 18 More recently, the development of flow diverting stents has created a new avenue to treat traumatic pseudoaneurysms.53 54 Although this treatment is not first-line or approved, flow diversion may have value in patients with pseudoaneurysms that have fusiform morphology or exert mass effect on adjacent structures, and in whom dual antiplatelet therapy is safe.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Teenage patient with a gunshot wound to the head. Angiography demonstrated a 12 mm pseudoaneurysm (a, red arrow) of the right middle cerebral artery with adjacent hemorrhage (a, black arrow). The patient underwent successful n-butyl-cyanoacrylate (embolization of the pseudoaneurysm (b).
Thrombectomy
Cerebrovascular trauma workflows have benefited from recent improvements in systems of care and in-hospital workflows surrounding mechanical thrombectomy.48 49 Patients experiencing BCVI or PCVI may directly benefit from mechanical thrombectomy when large vessel occlusions develop secondary to cerebrovascular trauma. A study of mechanical thrombectomy for stroke secondary to arterial dissection demonstrated successful recanalization in 80% of cases.55
Venous thrombectomy is less commonly performed than arterial thrombectomy, ostensibly owing to weaker evidence, greater effectiveness of medical management, and greater physiological tolerance of venous occlusions. Evidence for venous thrombectomy in the setting of trauma is especially scant, but extrapolating evidence from non-trauma settings suggests venous thrombectomy may warrant consideration in specific clinical scenarios, including clear neurological deterioration or infarct progression attributable to venous sinus thrombosis despite appropriate anticoagulation.56 57
Follow-up of untreated lesions
Untreated, high-grade cerebrovascular lesions secondary to traumatic injury are associated with high rates of morbidity and mortality. As a result, these lesions have received greater attention from trauma specialists.5 Generally, earlier medical or interventional treatment of high-grade lesions leads to better clinical outcomes.
For lesions managed non-operatively, lesion evolution typically occurs within 30 days of initial injury and rarely beyond 90 days of injury.5 Many authors recommend initial imaging follow-up with CTA or MRA within 7–14 days of injury, and continued surveillance through 90 days. For lesions that have not progressed within 90 days, continued imaging surveillance might not be necessary to monitor for progression but might aid in the decision to discontinue antiplatelet or anticoagulant medication.
Non-vascular management
Management of multiple concomitant injuries in the setting of polytrauma can be extremely challenging and requires thoughtful triage and prioritization of risk, as non-vascular injuries may also demand immediate attention.58 For example, primary injury to a cerebral artery can result in secondary ischemia and edema of the brain, which can lead to elevated intracranial pressure. In such cases, external ventricular drainage or craniectomy may be lifesaving. Similarly, injuries to the cervical vessels may be accompanied by injuries to the aerodigestive tract that must be promptly addressed to maintain an appropriate airway and prevent chemical injury or infection in the neck and mediastinum.
Non-vascular injuries may also impede management of vascular injuries. For instance, up to 9.2% of patients with severe traumatic brain injury have accompanying BCVI.59 In such cases, mitigation of secondary ischemic risk of BCVI may incur an elevated risk of intracranial hemorrhage or expansion of hemorrhagic contusions.14
Conclusions
Traumatic cerebrovascular injuries are common and potentially devastating. Modern advances in imaging techniques and treatment, combined with emerging evidence and collaborative multidisciplinary approaches, provide an opportunity to improve the diagnosis and management of BCVI and PCVI and reduce the potential for significant long-term morbidity that can result from inappropriately managed cerebrovascular trauma.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Contributors Designing/planning the manuscript: DCL, ARC, APK. Drafting the manuscript: DCL, APK. Critically reviewing and editing: APK, ARC. Approving the final version: DCL, APK, ARC.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests APK’s institution receives research funds related to industry trials from Medtronic and Microvention. APK does not personally receive these funds. APK receives consulting income from Penumbra and Microvention. This relationship is not related to the content of this manuscript.
Provenance and peer review Commissioned; externally peer reviewed.