Article Text

Abstract
Cerebral venous thrombosis (CVT) mostly affects young people. So far, endovascular treatment (EVT) has not been shown to be beneficial in CVT, partially because venous EVT tools are not yet fully optimized, and therefore EVT is only used as a rescue treatment in rare cases. Identifying a subgroup of CVT patients that could benefit from EVT is challenging, given the milder course of disease compared with acute ischemic stroke, the paucity of data on prognostic factors (both in the clinical and imaging domain), and the lack of consensus on what constitutes 'technical success' in CVT EVT. In this review, we discuss the major obstacles that are encountered when trying to identify CVT patients that may benefit from EVT, and propose a roadmap that could help to overcome these challenges in the near future.
- vein
- thrombectomy
- thrombolysis
- stroke
- device
Statistics from Altmetric.com
Introduction
Cerebral venous thrombosis (CVT) mostly affects young people and occurs with an incidence slightly lower than ruptured intracranial aneurysms. So far, endovascular treatment (EVT) has not been shown to be beneficial in CVT: a recent randomized trial investigating its benefit was stopped early for futility, and most other data are derived from small retrospective single center studies and thus prone to bias. Therefore, at present, EVT is only used as a rescue treatment in rare cases. Identifying a subgroup of CVT patients that could benefit from EVT is challenging, for several reasons. First, given the much younger patient population that is affected by CVT compared with acute ischemic stroke, traditional outcome measures, such as the modified Rankin Scale score, may not be appropriate. Second, our knowledge on prognostic factors and predictors of EVT effect is limited, and thus uncertainty remains regarding in which patients EVT should be considered. In particular, the importance of imaging findings in CVT has not been studied well. Third, the question of whether EVT should be used as a firstline or rescue treatment needs to be answered. Fourth, as opposed to acute ischemic stroke, partial recanalization may suffice to improve symptoms and there is no consistent definition of 'technical success' when performing EVT for CVT. Fifth, current EVT tools have been developed for the arterial vasculature and are not optimized for venous vessels. In this review, we discuss these major obstacles that are encountered when trying to identify CVT patients that may benefit from EVT, and propose possible solutions to overcome these challenges.
Literature search
We searched the electronic databases Medline (PubMed), Google Scholar, and Embase using the search terms 'venous', 'sinus', 'vein', 'thrombus', 'occlusion', 'brain', 'cerebral', 'intracranial', 'endovascular', 'thrombolysis', 'alteplase', 'urokinase', 'local', 'mechanical', 'thrombectomy', and 'catheter'. We included original research studies, systematic reviews, and meta-analyses that (1) reported angiographic and/or clinical outcomes of patients with CVT treated with some form of endovascular technique (either mechanical or pharmacological), (2) included at least 5 patients, and (3) were published in the English language. Bibliographies of identified manuscripts were screened for additional relevant studies. The literature search is up to date as of October 10, 2021. Online supplemental tables 1 and 2 summarize key findings of the 42 studies that were identified during the literature search, most of which were small single center retrospective studies. We identified only one randomized controlled trial comparing EVT with best medical management in CVT that was stopped early for futility.1 We further identified three systematic reviews, which concluded that no particular EVT technique was superior to another (online supplemental table 3).2–4
Epidemiology of CVT
CVT accounts for approximately 0.5% of all strokes,5 with an incidence of 1–2 per 100 000 person years, which is similar to ruptured intracranial aneurysms.6 Incidence rates vary among ethnicities,7 and are generally higher in more recent studies compared with older studies,8 9 likely related to the improvement in imaging techniques. In autopsy series, however, CVT is found in up to 9%, suggesting that the true incidence may be higher.10
Risk factors include female sex, age between 30 and 50, pregnancy and puerpurium, malignancies, infections, thrombophilia and other prothrombotic medical conditions, and drugs. Local factors include trauma (eg, a skull fracture that involves a sinus) and local infections.5 In a large prospective cohort study, the mean age at diagnosis was 39 years, and 75% of patients were women.11 Our literature review confirmed the female predominance and relatively young age of the affected patient population, and one or more of the above mentioned risk factors were identified in most patients (online supplemental table 1).
Symptom onset may be acute (ie, <2 days in 30% of cases), subacute (ie, 2–30 days in 50% of cases), or insidious (ie, >30 day in 10% of cases).12 In acute cases, the predominant symptom is headache, which occurs in >75%,13 and was also the most common symptom in the EVT studies in our literature search (online supplemental table 1). Seizures occur in up to 40%, and focal neurological deficits, most commonly motor weakness up to hemiparesis, in up to 44%.14 Although this review will focus on acute and subacute presentations, it is important to note that intracranial hypertension and dural arteriovenous fistulas may develop as sequelae of chronic CVT and can cause chronic headache with papilledema, tinnitus, ocular palsy and exophthalmos.5 15
The risk of focal neurological deficits and death as sequelae of CVT has decreased over the past decades, probably as a result of earlier recognition and improved medical care in general.10
Imaging manifestations of CVT
Direct signs
The filling defects in the thrombosed vessels can be visualized directly on non-invasive imaging, such as CT or MR venography. The most commonly involved vessel in CVT is the superior sagittal sinus, followed by the transverse sinus and the deep venous system, with thrombi extending into multiple sinuses (eg, the transverse and sigmoid sinus) in up to 90%.16 Occlusion locations in the EVT CVT studies we identified in the literature search showed a similar distribution (online supplemental table 1). Cortical vein thrombosis has been reported in 17% of cases,11 although cortical vein involvement may be underreported since it may not be recognized when a large sinus thrombosis is the predominant finding.17
Indirect signs
Often a patient may undergo brain parenchymal imaging and CVT may not be suspected. In these cases, venography may not be performed and indirect signs may be the only clue to the diagnosis. Indirect signs include a hyperdense on (non-contrast CT)/hypointense (on gradient recalled echo MRI and susceptibility weighted MRI) thrombus in the location of a sinus or cerebral vein and visualization of collateral venous pathways; enlarged medullary veins, which are particularly well seen on gradient recalled echo and susceptibility weightedMRI, and tentorial and dural enhancement due to enlarged dural collateral vessels.18 These findings are, however, unspecific and only present in a minority of patients.17
Parenchymal changes occur in almost 50% of cases.8 Both vasogenic and cytotoxic edema may occur and be present simultaneously. Hemorrhagic changes are seen in 40%,11 although hemorrhage rates may be higher in certain patient subgroups, such as those with vaccine induced CVT.19
Medical and surgical management of CVT
Because CVT is a relatively rare disease, available data on medical and surgical management are scarce, and thus the evidence supporting current recommendations of North American and European guidelines is weak.20 21 Currently, the cornerstone of CVT treatment is anticoagulation with unfractionated or low molecular weight heparin, even in patients with hemorrhagic lesions. Supportive treatment is provided as needed, for example in the form of antiepileptic drugs in case of a seizure, or antibiotics to treat a local underlying infection.20 21 No robust data are available regarding the benefit of systemic thrombolysis and steroids in the acute phase and secondary prevention strategies in the post-acute phase.20 21
With regard to surgical management, decompressive surgery (hemicraniectomy or hematoma evacuation) has been proven beneficial and is thus recommended in patients with impending herniation.20 21
Endovascular treatment for CVT: current state of evidence
The available data on EVT in patients with CVT do not allow for a recommendation of EVT as a routine treatment. The Thrombolysis or Anticoagulation for Cerebral Venous Thrombosis (TO-ACT) randomized controlled trial, which compared EVT in addition to best medical management with best medical management alone in CVT patients with at least one risk factor for poor outcome, was stopped early for futility.1 Numerous case reports and small retrospective studies reporting successful EVT for CVT mostly lack a control group and are at high risk of bias (online supplemental table 1).
To establish or dismiss EVT as a treatment option for CVT, the following questions need to be answered: (1) is there a subgroup of patients that may still benefit from EVT? (2) If yes, can imaging help us to identify these patients? (3) How do we evaluate technical EVT success most accurately? (4) Which clinical outcome measures should be chosen that are appropriate and relevant for the CVT patient population? Although acute ischemic stroke and CVT are fundamentally different diseases, the current situation of EVT for CVT in some ways resembles the situation of EVT for acute ischemic stroke a decade ago, when early EVT trials failed to show benefit, mainly because patient selection criteria did not ensure that enrolled patients benefited from treatment.
In the following, we review the challenges associated with these questions, and propose a framework for how to overcome them.
The challenge of choosing an appropriate clinical outcome
Outcomes in CVT are considered to be generally good (ie, less disabling compared with other neurovascular emergencies, such as acute ischemic stroke or ruptured intracranial aneurysms). Clinical outcome in CVT is mostly described with the modified Rankin Scale (mRS) score, which was also the most commonly reported outcome in the identified CVT EVT studies (online supplemental table 2). Reported mortality rates were mostly below 10%.11 On the other hand, in a large prospective cohort study, at 6 months, 22% of patients did not fully recover at 6 months and 14% did not have a good outcome (mRS >2).8 Studies that evaluated long term sequelae have also found that patients with CVT often suffer from residual symptoms, such as chronic headache and cognitive complaints. The studies that were identified in our literature review showed, on average, similar outcomes, although with a higher variability, probably due to their small sample sizes and inclusion of more severely affected patients that required EVT as rescue treatment (online supplemental table 2). Given the much younger patient population, however, caution should be used in applying the same definition of 'good outcome' to CVT patients that is used in acute ischemic stroke. A young woman with an mRS score of 1 at 6 months after CVT, for example, may well be functionally independent, but chronic headaches and subjective cognitive impairment may still have a substantial negative impact on her life and even prevent her from returning to work.22 Using alternative mRS criteria (eg, mRS 0–1, return to baseline mRS, change compared with baseline mRS), more granular cognitive outcome scales (eg, Montreal Cognitive Assessment), patient self-reported outcomes (eg, European Quality of Life Five Dimensions, EQ-5D), or even economic outcome measures (healthcare costs, absent days from work) may allow for a more meaningful outcome reporting in CVT patients.22 Needless to say, all of these outcomes have their advantages and disadvantages, and whether a trial using such outcomes will change practice is uncertain.
The challenge of patient selection
One of the major problems when establishing EVT as a treatment for CVT is accurate identification of those patients who are likely to benefit from EVT. Figures 1 and 2 show two exemplary similar cases with extensive thrombosis involving several sinuses. The first one worsened despite immediate anticoagulation with heparin, and underwent EVT, with a good outcome (figure 1). The second patient, despite having a similarly high thrombus burden, improved with heparin and oral anticoagulation with vitamin K antagonists alone (figure 2). In the International Study on Cerebral Vein and Dural Sinus Thrombosis Study (ISCVT), a large prospective cohort study (n=624), age >27 years, male sex, coma, mental status disorder, hemorrhagic changes at baseline imaging, deep cerebral vein thrombosis, CNS infection, and malignancy were identified as independent risk factors for poor outcome,11 most of which were confirmed in a later validation study and incorporated into a proposed risk score.23 Furthermore, preliminary small studies that were published during the COVID-19 pandemic suggest that patients with vaccine induced CVT may be at high risk of poor outcome and often do not respond to medical management, suggesting that EVT could be beneficial in this patient subgroup.19 It is however not clear whether these factors are also predictive of the EVT treatment effect, which would be a key requirement for an EVT selection criterion.
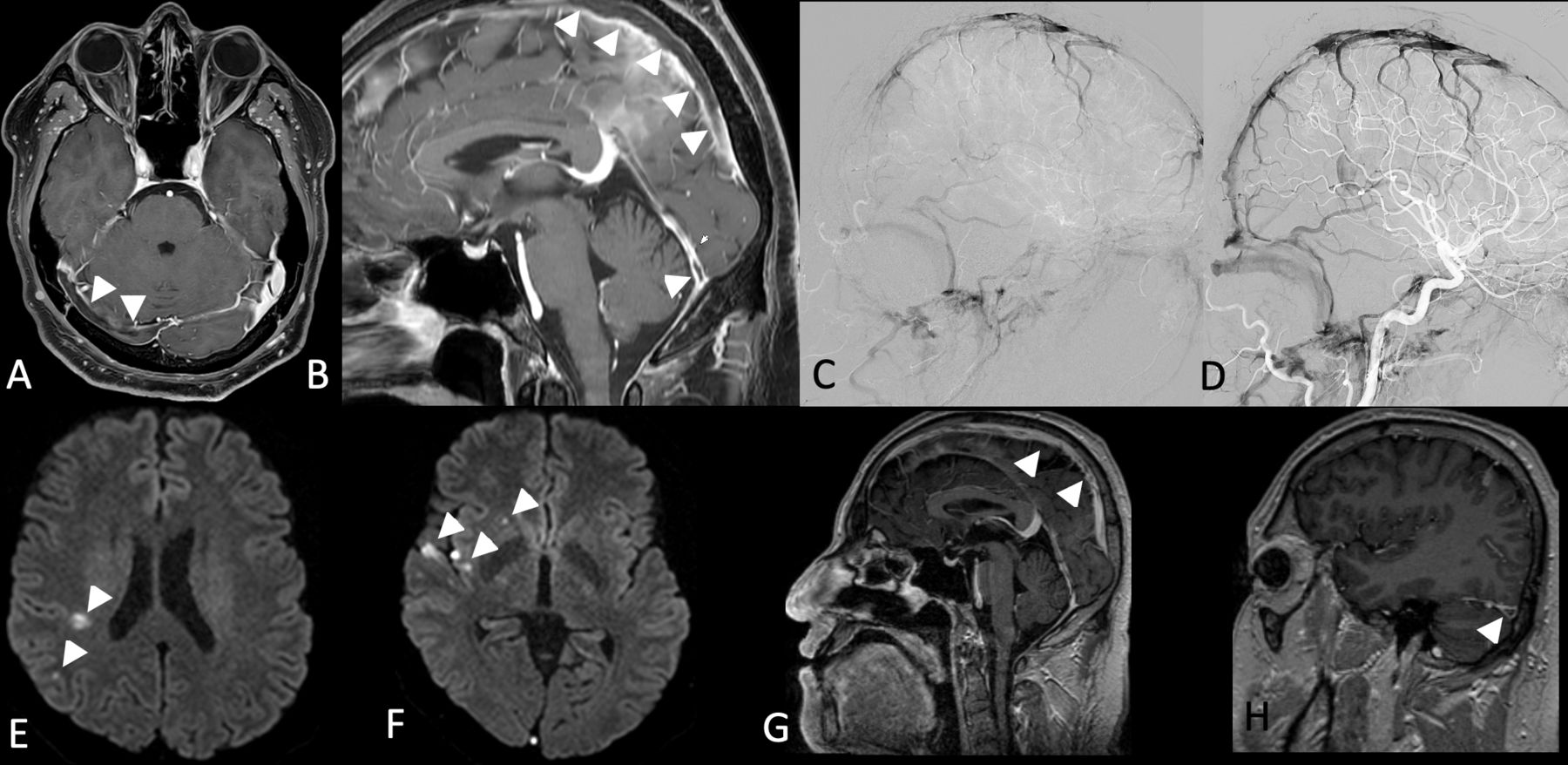
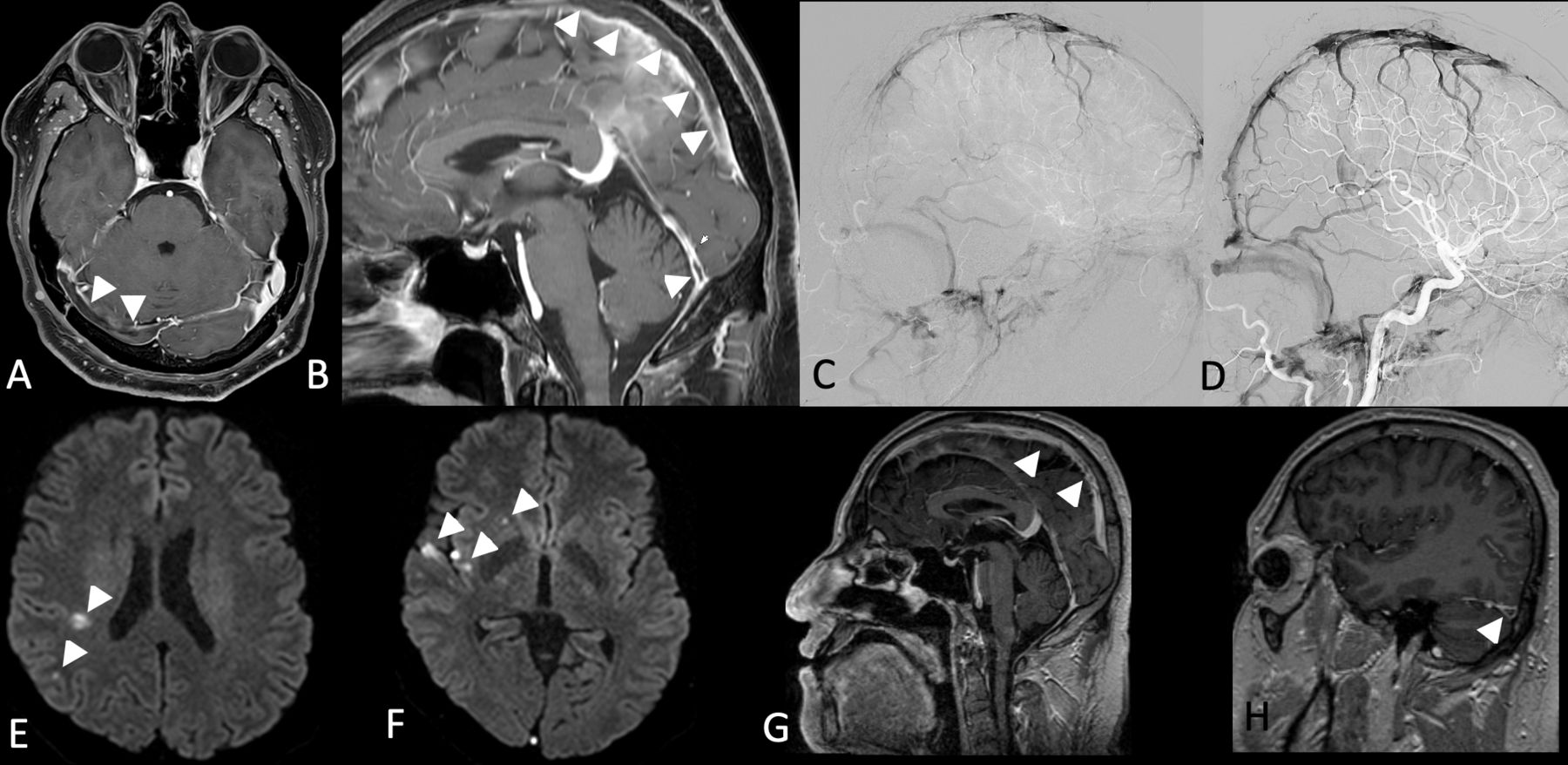
A patient in their thirties presented with headaches and right-sided cranial nerve VI palsy (National Institutes of Health Stroke Scale (NIHSS) score of 1). Contrast enhanced MRI showed extensive thrombosis of the right transverse sinus (arrows in A), thrombosis of the sigmoid sinus and internal jugular vein, the superior sagittal sinus, and straight sinus (arrows in B). There were no imaging findings of infarction or hemorrhage at that time. The patient was treated with heparin and oral anticoagulation. On day 4, his headaches worsened, MRI showed no new findings, and it was decided to proceed with endovascular treatment (EVT) (pre-EVT angiogram shown in C). Arterial access was established via the right radial artery and venous access via the right internal jugular vein. Multiple thrombectomy passes with a 6×30 mm stent retriever and a CAT 7 aspiration catheter (combined approach) were then performed to reduce the thrombus burden in the right transverse sinus, sigmoid sinus, superior sagittal sinus, and straight sinus. After partial recanalization of all thrombosed sinuses (post-EVT angiogram shown in D), the patient was transferred to the stroke unit. Diffusion weighted imaging on day 5 (24 hours after EVT) showed several small infarcts in the right hemisphere (arrows in E and F), and partial recanalization of the superior sagittal sinus (arrows in G) and the right transverse sinus and remaining sinuses, with small residual filling defects (arrow in H). The patient’s symptoms nearly completely resolved within 24 hours after EVT (NIHSS 0), with slight residual headaches that did not require medication. He was discharged on day 7 after the procedure and returned to work several weeks after discharge. (Courtesy of Dr Ioannis Tsogkas and Dr Marios-Nikos Psychogios.)
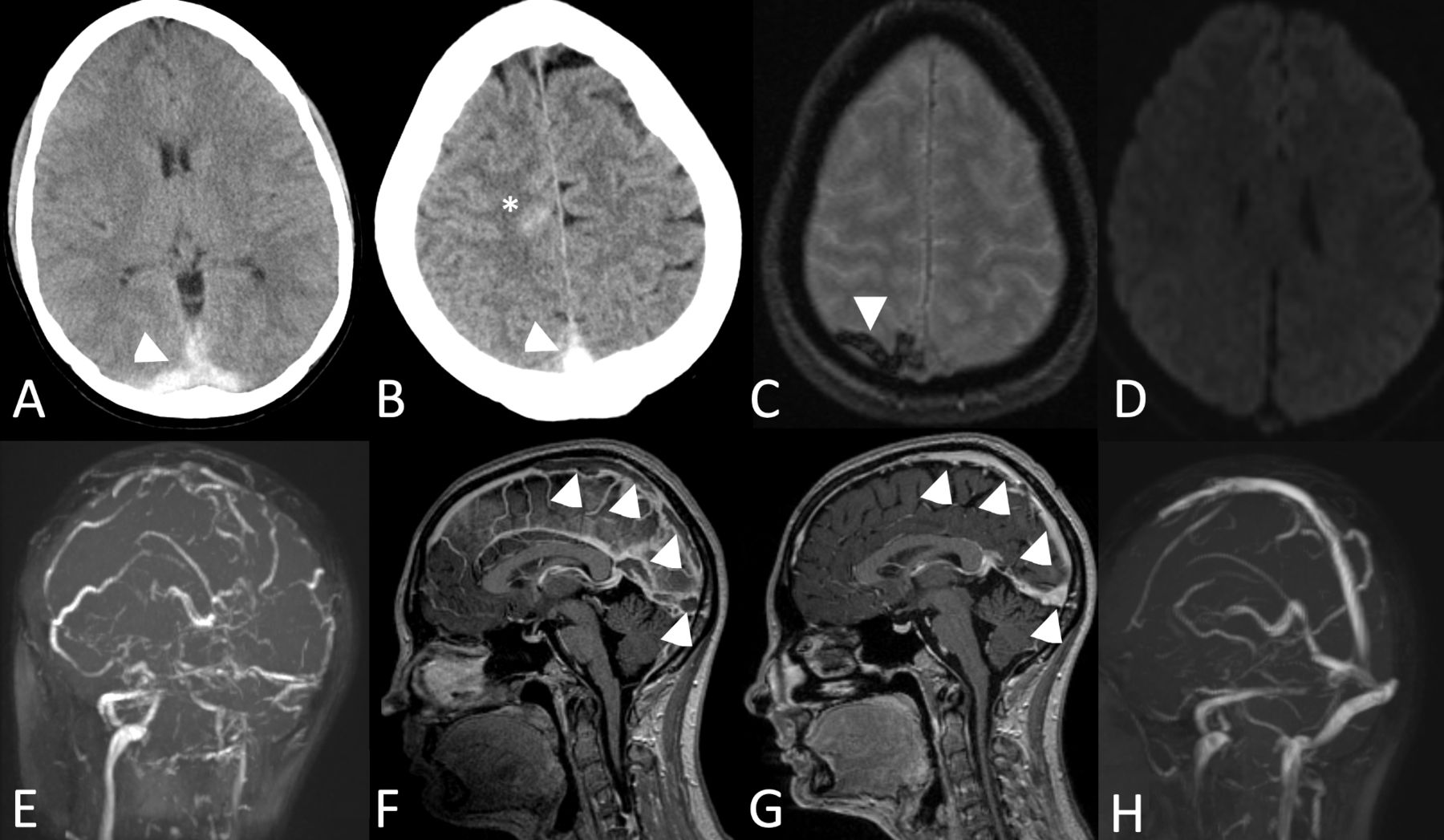
A patient in their forties presented with sudden headaches, left-sided hemiparesis, and blurry vision (National Institutes of Health Stroke Scale (NIHSS) score of 8). Non-contrast CT showed hyperattenuation of the superior sagittal sinus, transverse sinuses (arrows in A and B, and small subarachnoid hemorrhage in the right frontal lobe (asterisk in B). Subsequent MRI was performed and showed susceptibility artifacts in the thrombosed sinuses and in a cortical vein in the right parietal lobe (arrow in C) but no enlarged cortical and medullary veins (C). No infarction was present on diffusion weighted imaging (D). Venous time of flight MR angiography (E) and contrast enhanced MRI (F) confirmed extensive thrombosis of the superior sagittal sinus and transverse sinuses (E, arrows in F). Treatment with heparin was initiated, followed by oral anticoagulation with vitamin K antagonists. The patient’s symptoms nearly fully resolved (NIHSS at 24 hours was 1). Follow-up MRI at 1 month (G, contrast enhanced MRI; H, venous time of flight MR angiography) shows complete revascularization of the occluded sinuses (arrows in G). The brain parenchyma did not show any abnormalities.
Another major problem with regard to patient selection is that most population based studies report outcomes of CVT in general, mostly without stratifying by occlusion location. Currently, only thrombi in larger vessels (superior sagittal sinus, transverse, sigmoid, and straight sinus) can be safely accessed and recanalized with endovascular tools. Assuming that thrombosis of larger vessels carries a higher risk of poor outcome, we may conclude that patients with EVT accessible occlusions may also be the ones at high risk of poor outcome with current best management. The ISCVT Study showed that deep cerebral vein thrombosis is a predictor of poor outcome,11 but outcomes of occlusion locations that are amenable to EVT versus those that are inaccessible by endovascular means were not reported separately.
The challenge of imaging CVT
Closely related to the problem of patient selection is the question of how to best image patients with CVT. To guide EVT decision making, imaging in CVT should answer two questions: (1) is there a target occlusion amenable for EVT and (2) is there tissue at risk for hemorrhage or edema that can be salvaged with EVT? While the first question can reliably be answered with CT or MR venography, which were the predominantly used imaging modalities in the identified CVT EVT studies (online supplemental table 1), there is a paucity of data on what constitutes the best imaging method for the brain parenchyma in CVT in general, and for assessing the risk of parenchymal damage and poor prognosis in particular. Several smaller studies have identified imaging features associated with a poor clinical outcome, such as hemorrhagic changes,11 23 24 and reduced cerebral blood flow and cerebral blood volume.25 26 However, thresholded 'core' and penumbra perfusion maps as we know them from acute ischemic stroke imaging, are not available for venous infarcts. Some authors have described the imaging complex of 'venous congestion', which they loosely defined as 'findings of intracranial hemorrhage, hematoma, or edema' to be associated with poor outcomes.24 Assessing venous congestion in a more standardized, quantitative way is possible with susceptibility weighted MRI and quantitative susceptibility mapping,27–29 but this is currently only done in the context of research studies and has not yet found its way into routine practice. Somewhat counterintuitively, diffusion restriction, which is considered the gold standard for infarct 'core' in acute ischemic stroke, commonly resolves on follow-up imaging and is thus not a reliable marker for irreversible tissue damage in CVT.30 31 Importantly, even if imaging findings are indicative of a poor prognosis with current best medical management, they are not necessarily useful EVT selection criteria, since they may not predict the EVT treatment effect. We identified only one study that explicitly investigated predictors of the EVT treatment effect, in which deoxyhemoglobin-rich thrombi were associated with increased chances of complete recanalization following EVT.32
Because the clinical picture of CVT is highly variable and fluctuates over time, and dedicated symptom severity scores (similar to the National Institutes of Health Stroke Scale for acute ischemic stroke) are not established for CVT, imaging could play an even greater role in patient selection for treatment and prognostication than it does in acute ischemic stroke. But the imaging information can only be leveraged based on well defined imaging findings yet to be established in large scale studies to identify patients at high risk of poor outcomes with current best medical management and those who may benefit from EVT.
Table 1 and online supplemental figure 1 provide an overview of imaging findings that have been proven to be associated with poor prognosis, and that could therefore serve as starting points for such large scale imaging studies.
Imaging features in patients with cerebral venous thrombosis associated with a poor prognosis
The challenge of timing EVT for CVT
Since most patients with CVT do relatively well, at least when using current outcome definitions, it may be reasonable to use EVT as a 'rescue treatment' in patients with clinical worsening, rather than as a firstline treatment strategy. Of the 42 identified EVT studies, only eight included CVT patients that underwent primary EVT (online supplemental table 2). However, thrombus composition changes over time, and as thrombi mature, their resistance to fibrinolytic drugs increases, and the chances of successful EVT may decrease, particularly in case of local intravenous thrombolytic treatments, so that the benefit of EVT may be decreased with rescue treatment.33 The fact that, unlike in acute ischemic stroke, we often cannot determine with certainty how long the thrombosis has existed prior to diagnosis adds to the uncertainty with regard to EVT timing. It is often assumed that the first symptom (almost always headache) marks the starting point of the thrombosis, but there are no reliable data suggesting that this is truly the case.
The challenge of defining 'technical success' in EVT for CVT
Currently, we are not clear about how to define technical treatment success of EVT. As opposed to acute ischemic stroke, in which there is a close relationship between angiographic reperfusion quality and clinical outcome, complete reperfusion may not be needed in CVT; reducing the thrombus burden may be sufficient to allow autofibrinolysis to dissolve the residual thrombus and achieve a good outcome (figure 1).34 Thus a more cautious approach may be reasonable, in which emphasis is put on avoiding treatment complications, even if this comes at the cost of leaving a higher thrombus volume in situ, as long as the final angiogram does not show substantially delayed venous drainage. Most EVT studies we identified used a trichotomized assessment (complete, partial, or no recanalization; online supplemental table 2), but did not provide outcomes stratified by recanalization status. The only randomized CVT EVT trial that has been conducted so far (TO-ACT) reported complete recanalization rates at 6–12 months, but did not assess recanalization immediately after the procedure, which would probably be a more immediate and meaningful measure of technical EVT treatment success.1
The problem of available tools
Typical aspiration catheters have a diameter of 2–3 mm, and the largest available stent retriever measures 6 mm in diameter, while the superior sagittal sinus has an average diameter of 10 mm in the occipital region.35 Thus complete thrombus removal is not possible with available aspiration catheters (figure 3A,C,D) and stent retrievers. Fogarty catheter systems are in theory sufficiently large to allow for complete thrombus removal,36 but their stiffness prevents them from being used in smaller sinuses and more distal vessels. Local intravenous thrombolysis is yet another treatment option. In theory, large bore aspiration catheters with diameters of 7 mm or more would allow for near complete thrombus removal (figure 3B,C), but such catheters are currently not available. Of the 42 identified studies, 30 reported using a combination of local intravenous thrombolysis (most commonly intravenous urokinase) and mechanical thrombus debulking or maceration. Eight studies reported using local intravenous thrombolysis only and only two studies exclusively used mechanical thrombus debulking; two studies did not specify their EVT technique (online supplemental table 2). The available evidence is not sufficient to determine the optimal endovascular treatment approach. The problem is further complicated by the fact that, due to the insufficient evidence for EVT as a treatment for CVT in general, not much effort has been made to optimize endovascular tools for venous EVT, and the results with current devices are therefore likely to be different from an ideal scenario in which dedicated venous EVT tools are available. Furthermore, large arachnoid granulations (online supplemental figure 2A,B), anatomical variants such as a persistent occipital sinus (online supplemental figure 2C,D), or focal dural defects with brain herniation into sinuses (online supplemental figure 2E,F) may render it impossible to access the thrombus and prohibit successful EVT.

{kind=link}
{kind=link}
{kind=link}
Current and ideal aspiration catheters for cerebral venous thrombosis (CVT) endovascular treatment (EVT). (A) Schematic drawing of a thrombus (red) in the superior sagittal sinus (8 mm diameter, shown in blue) and a typical 2 mm aspiration catheter, as it is currently commonly used for CVT EVT. (B) The same situation with an ideal, large bore aspiration catheter of 7 mm in diameter which is, however, currently not available. (C) Cross sectional view of (A) and (B) at the level of the dashed line, and illustrates the residual thrombus after one aspiration attempt with the two respective aspiration catheters. While a conventional 2 mm aspiration catheter merely creates a small channel in the thrombus (shown on the left in C), a large bore aspiration catheter would leave only minimal residual mural thrombus behind (shown on the right in C). (D) Conventional aspiration catheter. as shown in (A) in situ.
A way to move forward
Determining whether there is a subgroup of CVT patients who can benefit from EVT is challenging. Outcomes following CVT are presumed to be generally good, at least according to currently used outcome measures. Not much is known about the prognosis of patients with EVT amenable occlusions in particular, the clinical picture is widely variable, standardized imaging selection criteria for EVT have not been established, and the available endovascular tools have been designed for arterial occlusions and are therefore not optimized for the cerebral venous vasculature.
The steps that are needed for a systematic and 'fair' evaluation of EVT for CVT are (1) identification of imaging factors that are predictive of a poor prognosis and associated with an EVT treatment effect, and could therefore serve as imaging selection criteria for EVT, (2) validation of those imaging criteria in large datasets, (3) consensus on an appropriate definition for technical EVT success and meaningful clinical outcome measures, and (4) development of appropriate endovascular tools that are tailored to the venous cerebral anatomy. It may be argued that the neurovascular community should rather focus their research efforts on more common conditions, and similarly, the market may not be large enough for device manufacturers to justify development of dedicated EVT tools for CVT. However, the incidence of CVT is similar to ruptured intracranial aneurysms, a disease which has been studied extensively in numerous large prospective cohort studies as well as several randomized trials, and a whole device armamentarium has been developed for endovascular aneurysm treatment. Patients with CVT are young, and often pregnant women or young mothers that have just given birth to a child. We owe it to these patients and their families to thoroughly investigate whether EVT can help to improve their outcome, and should make it our priority to create sufficiently large databases and a framework that allow us to answer this question with confidence.
Supplemental material
Supplemental material
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
Acknowledgments
The authors thank Dr Ioannis Tsogkas and Prof. Marios Psychogios for figure 1 and Mr. Basti Uhmann for his help with figure 3.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @joachimfladt
Contributors JO, MG, RM and JF: conceptualization, drafting, and critical revision of the manuscript. All authors: critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial, or not-for-profit sectors.
Competing interests MG is a consultant for Medtronic, Stryker, Microvention, GE Healthcare, and Mentice. JO is a consultant for NICOLab.
Provenance and peer review Commissioned; internally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.