Article Text

Abstract
Background The primary goal of the CLARYS study is to assess the protection against rebleeding when treating ruptured bifurcation aneurysms with the Woven EndoBridge (WEB) device.
Methods The CLARYS study is a prospective, multicenter study conducted in 13 European centers. Patients with ruptured bifurcation aneurysms were consecutively included between February 2016 and September 2017. The primary endpoint was defined as the rebleeding rate of the target aneurysm treated with the WEB within 30 days postprocedure. Secondary endpoints included periprocedural and postprocedural adverse events, total procedure and fluoroscopy times, and modified Rankin Scale score at 1 month and 1 year.
Results Sixty patients with 60 ruptured bifurcation aneurysms to be treated with the WEB were included. A WEB device was successfully implanted in 93.3%. The rebleeding rate at 1 month and 1 year was 0%. The mean fluoroscopy time was 27.0 min. Twenty-three periprocedural complications were observed in 18 patients and resolved without sequelae in 16 patients. Two of these complications were attributed to the procedure and/or the use of the WEB, leading to a procedure/device-related intraoperative complication rate of 3.3%. Overall mortality at 1 month and 1 year was 1.7% and 3.8%, respectively and overall morbidity at 1 month and 1 year was 15% and 9.6%, respectively. WEB-related 1-month and 1-year morbidity and mortality was 0%.
Conclusions The interim results of CLARYS show that the endovascular treatment of ruptured bifurcation aneurysms with the WEB is safe and effective and, in particular, provides effective protection against rebleeding. It may induce profound change in the endovascular management of ruptured bifurcation aneurysms.
- aneurysm
- device
- hemorrhage
- intervention
- subarachnoid
Data availability statement
Data are available upon reasonable request. All data available upon request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Current literature1–3 indicates that coiling yields a better clinical outcome than clipping. The balloon remodeling technique4 is a widely used adjunctive tool to allow treatment of complex aneurysms, especially broad-based aneurysms, and has shown to be as safe as coiling alone.5 6 In some cases, coiling may be technically challenging owing to aneurysm geometry that necessitates the additional use of a stent.7 This treatment requires the concomitant use of antiplatelet medication, making it difficult to manage in patients with subarachnoid hemorrhage (SAH), especially if an external ventricular shunt is required.8 Ruptured bifurcation aneurysms present a larger challenge to treat due to their complex configurations and locations as coils are more prone to collapse in this situation.9 For these specific situations, newer endovascular management techniques are therefore required.
Over the past decade, the intrasaccular flow disruptor Woven EndoBridge (WEB, MicroVention, Aliso Viejo, California, USA) has been developed for the treatment of bifurcation aneurysms. Since its CE marking, the WEB has been evaluated in multiple clinical studies, including WEBCAST,10 French Observatory,11 WEBCAST 2,12 and WEB-IT.13 14 These studies have unanimously demonstrated the favorable safety and efficacy profile of the WEB in treating intracranial aneurysms, including the most challenging wide-neck bifurcation aneurysms. Published studies have included, in most cases, unruptured aneurysms.
The principle of operation of the WEB is to cause a progressive thrombosis of the aneurysmal sac, secondary to the effect of endosaccular flow disruption. In ruptured aneurysm treatment, the key point is to determine whether the aneurysmal sac thrombosis after WEB placement is fast enough to prevent early rebleeding, allowing its safe use in the acute stage. A few publications, either single center or retrospective, have shown promising results, reporting a very low rate of re-rupture after the treatment of ruptured aneurysms using WEB.15–19 However, there have been no multicenter studies assessing the clinical performance of using the WEB to treat ruptured aneurysms thus far.
This ability of the WEB to prevent early rebleeding—that is, within 1 month of aneurysm rupture20—seemed so important to us that we made it the primary endpoint of the study. In addition, special attention was paid to the extremely rigorous detection of any rebleeding after WEB treatment, and the protocol was specifically designed with this in mind. We also wanted to focus on clinical outcomes and clinical complications when using the WEB device in the specific setting of ruptured aneurysms. Since this early protection against rebleeding is associated with long-term clinical outcome, we will present here, in addition to the 1-month results, the 1-year clinical results.
Materials and methods
Study design
The CLARYS study is a prospective, multicenter, single arm study conducted at 13 interventional neuroradiological departments in France and Germany. The study enrolled patients with ruptured aneurysms of the anterior and posterior intracranial circulations. In this study, a patient with a ruptured aneurysm was defined as a patient with CT, MRI, or lumbar puncture evidence of SAH attributed to the index aneurysm within the past 30 days.
The CLARYS study is registered in ClinicalTrial.gov under NCT02687607. It received approval based on the national regulatory requirements, including sites’ ethics committee. Informed consent was obtained in compliance with applicable regulatory and institutional guidelines. The study was conducted under Good Clinical Practice:
An independent core laboratory evaluated all angiographic data and adjudicated effectiveness outcomes.
All adverse events were independently adjudicated by a clinical event adjudicator (CEA).
Data collected were 100% monitored and verified by an independent clinical research organization.
Inclusion criteria for the study were ruptured (Hunt and Hess grade I, II, or III) saccular aneurysms located in the basilar artery, middle cerebral artery (MCA) bifurcation, internal carotid artery terminus, anterior communicating artery, anterior cerebral artery, or posterior communicating artery. Diameter and height of the aneurysm had to have appropriate size for treatment with the WEB device, with a maximum width diameter ≤10 mm. All subjects meeting the inclusion/exclusion criteria and who underwent at least one attempt of treatment with a WEB device were enrolled in CLARYS.
Procedure
The embolization procedure was performed under similar conditions as those for standard coiling for ruptured aneurysms. After positioning a guiding catheter into the internal carotid artery or vertebral artery, the aneurysm was catheterized with a VIA 21, VIA 27, or VIA 33 microcatheter (MicroVention, Aliso Viejo, California, USA). The decision on which form of WEB (barrel shape, referred to as ‘WEB SL’ and sphere shape, referred to as ‘WEB SLS’) to use was left to the operator. An angiogram was obtained to check the position of the WEB in the aneurysm and to evaluate flow stagnation inside the aneurysm. Treatment with other devices (balloon, coils, or stents) was performed if deemed necessary by the treating physician. Any technical issues noted during the procedure were documented. Any adverse events or complications noted during the procedure/post-embolization were also documented on the case report and adverse event report forms.
CLARYS protocol to detect rebleeding after WEB placement
The protocol has been carefully designed to strictly monitor any rebleeding that may have occurred after the placement of the WEB device.
1. To ensure that there was no bleeding between the initial diagnosis of SAH and WEB placement, the initial imaging should be performed less than 6 hours prior to femoral puncture. It was mandatory to systematically repeat the flat-panel CT in the angiosuite in the following two situation:
(a) Either the time between the last CT scan and the start of the procedure was greater than 6 hours, even in the absence of any clinical change.
(b) A clinical worsening was observed at any time between the last CT scan and the placement of the WEB.
2. To ensure that any bleeding that might have occurred after WEB placement (and up to 1 month after treatment) was detected:
(a) A flat-panel CT scan was systematically performed in the angiosuite at the end of the treatment.
(b) A non-enhanced CT or MRI scan should be performed for any change in the patient’s neurological status (any new neurological deficit, disturbance of consciousness, worsening of acute headaches, signs of intracranial hypertension), from the time of the postoperative flat-panel CT scan until 1 month after the procedure.
Details of any additional diagnostic imaging preprocedure or performed between postprocedure and hospital discharge were collected and provided to the core laboratory/CEA. Thirty-day (±7 days) neurological follow-up was assessed with the modified Rankin Scale (mRS), completed during the office visit or by telephone interview. Any adverse events noted during the follow-up visit were documented and reviewed by the CEA.
CLARYS endpoints
The primary endpoint was defined as the rebleeding rate of the target aneurysm treated with the WEB within 30 days postprocedure. Rebleeding from the target aneurysm was defined as obvious evidence of hemorrhage on CT or MRI scans and hemorrhage depicted in the same territory as the initial bleeding and hemorrhage increased in size compared with initial preoperative CT scan.
Secondary endpoints included periprocedural and postprocedural adverse events, mRS score, and total procedure and fluoroscopy times. Definitions of adverse events and serious adverse events are in line with EN ISO 14155.
The 12-month clinical and angiographic follow-up was also a secondary endpoint. Nevertheless, patient safety requires that clinical data at 1 year be presented in this paper as well.
Results
Patient demographic and baseline characteristics
From February 2016 to September 2017, 60 patients (31 women and 29 men) aged 26–78 years (mean 54.5±11.5 years) were treated with the WEB device. The baseline characteristics including medical history, Hunt and Hess score, and mRS score, are presented in table 1. More than 50% had a history of smoking and more than one-third had a history of systemic hypertension.
Patient and aneurysm characteristics
Aneurysm characteristics
All patients were diagnosed with ruptured aneurysms. Each patient was treated for one aneurysm. The anatomical locations and dimensions of the treated aneurysms are listed in table 1. Most (60%) of the treated aneurysms were broad-based and mainly (81.6%) located in the anterior communicating artery or MCA bifurcations.
Procedural data
Deployment of the WEB device was successfully achieved in 56 cases (figure 1), yielding a technical success rate of 93.3% (56/60). In the four cases in which the WEB device was not implanted, the WEB device was successfully retrieved prior to detachment and the aneurysms were subsequently treated with coils. In two of the four cases, the WEB device was not deployed properly owing to unfavorable aneurysm morphology. Safe detachment of the WEB was not possible in the third case due to the unclear visualization of the aneurysm, and satisfactory positioning was not achieved in the fourth case.
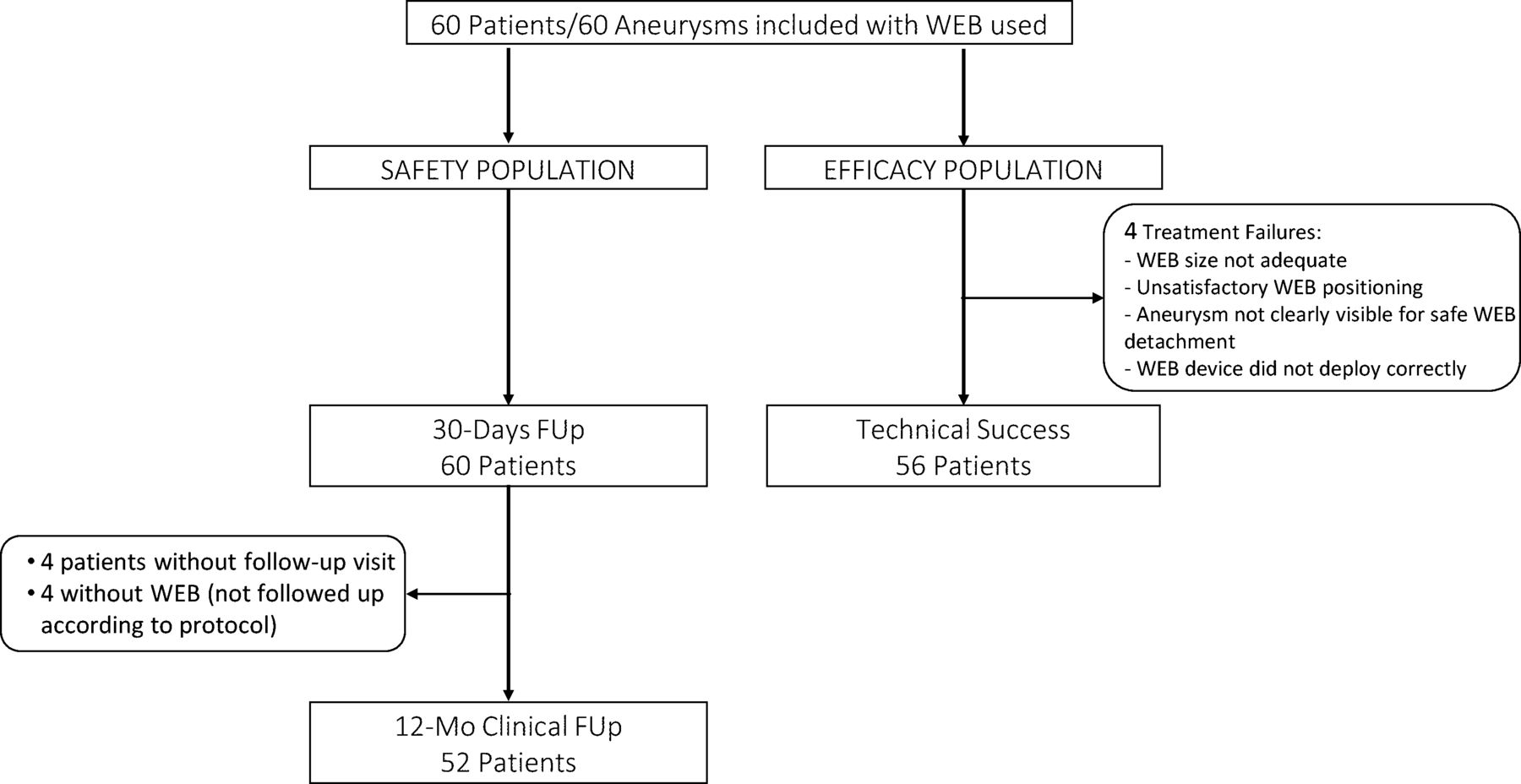
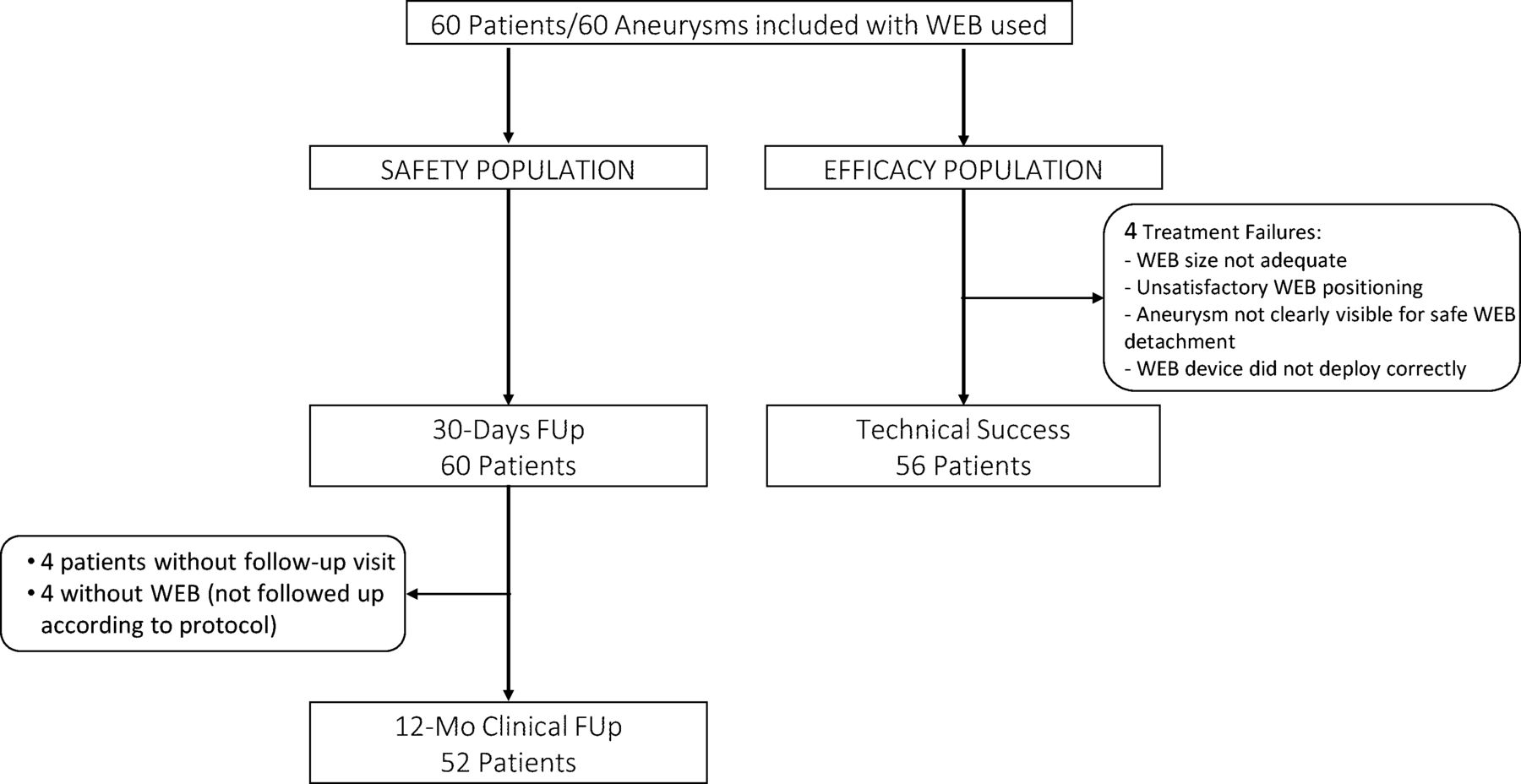{kind=link}
Population flow chart for safety and efficacy analysis.
Forty-five (80.4%) of 56 aneurysms were treated with the WEB SL and 11 (19.6%) aneurysms were treated with the WEB SLS. Adjunctive devices were used in 3 of the 56 (5.4%) patients successfully treated with the WEB, including balloon remodeling in one aneurysm, and stenting in two aneurysms because there was a protrusion of the device in the parent vessel.
Procedure time and fluoroscopy time were calculated for the 56 patients in whom a WEB device was implanted. Mean WEB procedure time was 75.3 min (range 12–235) and mean fluoroscopy time was 27.0 min (range 6–82).
Perioperative antiplatelet medication
Table 2 depicts the antiplatelet therapy, if any, administered to patients, according to the time of its administration. All, but four patients, were not receiving antiplatelet treatment prior the procedure. A total of 43% of patients received one or more antiplatelet agents during the procedure, which was continued postprocedure in 30% of treated patients.
Perioperative antiplatelet medication
Primary endpoint: effectiveness defined as the rebleeding rate within 30 days postprocedure
No rebleeding was observed in any patients up to 1 month after WEB placement in the target aneurysm. Thus, the rebleeding rate in this cohort was 0.0% and, no target aneurysm re-treatments were performed within the month following WEB placement.
Safety: periprocedural adverse events
Safety was assessed in the whole population, including the four treatment failures (figure 1).
Twenty-three periprocedural events, with or without clinical consequences, were observed in 18 patients (table 3):
Ten were thromboembolic events (16.7%), leading to clinical consequences in 2 patients:
(a) Two were related to the WEB. One clot occurred at the level of the neck of the aneurysm treated with WEB. It was treated with abciximab but led to an ischemic occipital stroke, with visual field modification. The other clot was a protrusion of the WEB leading to clot formation at the level of the neck, treated with abciximab and deployment of a stent, without clinical impact.
(b) Five were adjudicated to be possibly related to the WEB or procedure, without knowing the accountability of one more than the other. All received perioperative antiplatelet treatment, and for three patients, this treatment was extended postprocedure. None had clinical consequences.
(c) Three were adjudicated as not related to the WEB but to the procedure. One patient had preoperative antiplatelet therapy; all three patients received intraprocedural antiplatelet therapy, which was extended postoperatively in two patients. One had a clinical consequence: a thromboembolic complication with perfusion deficit within a branch distal to the WEB, without any WEB protrusion or clot at the level of the neck (this patient received antiplatelet therapy perioperatively and postoperatively).
Two events were perioperative rupture (3.3%): both occurred after several repositioning maneuvers of the WEB. Bleeding was observed on the angiogram after removal of the WEB. Both were treated with coils. Both ruptures did not lead to modification of the clinical status.
Four events were vasospasm (6.7%), all adjudicated to the underlying disease condition. One of those led to a worsening of the clinical condition.
One event was a hydrocephalus (1.7%), also adjudicated to the underlying disease condition, which did not lead to clinical modification.
one event was a patient with headache, adjudicated to the underlying disease condition, which did not lead to clinical modification.
Five events were non-neurological, including pneumonia (1), epistaxis (1), and hematuria (1), all in the same patient; hypertension (1) and urinary tract infection (1) were also noted. All were without clinical neurological consequences.
Periprocedural events, with or without clinical consequences and adjudication of causality by the clinical event adjudicator (CEA)
To summarize, among the 23 periprocedural events:
Four were related to the WEB; 5 were related to the procedure or the WEB; 3 were related to procedure, not to the WEB; 11 were neither related to the procedure nor to the WEB.
There were 18 neurological/neurovascular periprocedural events, with or without clinical consequences, occurring in 17/60 patients.
Among them, 2/60 (3.3%) patients had neurological clinical impact in relation to the procedure and/or device. Both were periprocedural thromboembolic events.
Of the two patients who had a neurological clinical consequence in relation to the procedure and/or device:
One patient developed a clot that occurred at the level of the aneurysm neck treated with the WEB, leading to an ischemic occipital stroke. This patient was initially Hunt and Hess grade II at admission, mRS score 2 at 1 month.
One patient developed a perfusion deficit within a branch distal to the WEB, without any WEB protrusion or clot at the level of the neck. The patient was Hunt and Hess grade II at baseline. This patient also had a vasospasm that was adjudicated as responsible for the clinical worsening, with an mRS score of 4 at 1 month.
Serious adverse events (SAEs) after the procedure and before 1 month
As adjudicated by the CEA, 17 serious adverse events occurred in 11 patients following the procedure up to follow-up at 30 days. None of them were related to WEB.
Of the 17 SAEs, four had clinical sequelae:
One patient (No 1) died 6 days after the procedure owing to clinical vasospasm and this event was adjudicated to be related to the patient’s disease condition, resulting in a mortality rate of 1.7% (1/60).
Two were related to the underlying disease: one case of clinical vasospasm and one case of hydrocephalus
One was infection of the central venous catheter, adjudicated to be related to the concurrent conditions
The remaining 13 SAEs all resolved without clinical sequelae: 2 clinical vasospasms, 2 hydrocephalus, 2 pneumoniae, 2 urinary tract infections, 1 SAH, 1 pulmonary embolism, 1 peripheral thromboembolism, 1 arrhythmia, and 1 infection.
Morbidity at 1 month
The overall morbidity (mRS score >2) rate at 1 month was 15.0% (9/60). The morbidity in all nine patients was adjudicated as unrelated to the WEB.
Among these nine patients:
Three had an mRS score of 5, adjudicated to be associated with the underlying disease: patient No 4 experienced vasospasm 3 days after the procedure, patient No 7 experienced hydrocephalus 1 day after the procedure, and the third patient had urinary tract infection, hypothyroidism, and pulmonary disease.
Two had an mRS score of 4: patient No 3 experienced periprocedural vasospasm that was related to the pre-existing underlying disease condition, patient No 5 had a periprocedural thromboembolic event that was related to the procedure and also experienced two vasospasm events 1 and 2 days after the procedure that were much more severe than the periprocedural thromboembolic event.
Four had an mRS score of 3. One was the patient already described in the SAE section, having infection of the central venous catheter. The three other patients (including Patient No 6) had no event with clinical impact and the morbidities are related to the initial SAH.
Perioperative antiplatelet regimen in the context of periprocedural adverse events
In summary, the status of the presence or absence of antiplatelet therapy when a non-peripheral intraoperative complication occurred was as follows:
Among the 10 thromboembolic complications, only one patient received preoperative antiplatelet therapy, and all received intraoperative antiplatelet therapy, which was continued postoperatively in six patients.
Among the two intraoperative ruptures, one patient was receiving antiplatelet therapy during the procedure.
The one patient who presented with hydrocephalus received intraoperative and postoperative antiplatelet therapy.
Clinical results at 12 months
At the 1-year follow-up, no ruptured aneurysm acutely treated by WEB has shown rebleeding.
Among the baseline population of 60 patients, 52 patients were evaluated for 12-month clinical safety (figure 1). The four patients who were not treated with the WEB device were followed up only to 30 days according to the protocol. Four additional patients were not evaluated at 1 year because they refused to return to hospital and the mRS score could not be evaluated at that time. However, their clinical status was assessed between 1 and 11 months: the first patient had a mRS score of 0 at 1 month and moved abroad without leaving any contact details, the second and third patients were seen at 3 and 7 months, respectively, and their mRS score was 0, the last patient was called at 11 months, but reported no complications, and the mRS score was not evaluated. Patients re-treated before the 12-month visit are included in the 1-year clinical follow-up analysis.
The results of mortality and morbidity among the 52 patients are described in the table 4.
Description of morbidity and mortality at 1 month and 1 year
The overall 1-year mortality was 3.8% (2/52). The two deaths were adjudicated to be related to the initial disease condition:
Patient No 1 has already been described above: they experienced a vasospasm and died 6 days after the procedure.
Patient No 2, over 70 years of age, had a progressive worsening of their general status, without new hemorrhage. They were never discharged from hospital and died over 70 days after the initial bleeding.
The 1-year morbidity rate was 9.6% (5/52). The five events meeting the morbidity definition were adjudicated to be related to the initial disease condition.
Three patients experienced a vasospasm and have already been described above. Their events were adjudicated as related to their initial disease condition. For patient No 3, the perioperative vasospasm resulted in an ischemic stroke requiring prophylactic craniectomy. The mRS score was 4 at 1 month and remains 4 at 1 year. Patient No 4 experienced a vasospasm 3 days after the procedure, the mRS score was 5 at 1 month and 4 at 1 year. Patient No 5 experienced a periprocedural thromboembolic event that was related to the procedure. Afterwards, the patient experienced two vasospasms 1 and 2 days after the procedure that were much more severe than the periprocedural thromboembolic event, the mRS score was 4 at 30 days postprocedure and 3 at 1 year.
Patient No 6 had a mRS score of 5 at 1 month, adjudicated to be related to initial SAH, the mRS score was 3 at 1 year.
Patient No 7 developed a postoperative hydrocephalus leading to cognitive impairment, the mRS score was 5 at 1 month and 4 at 1 year.
All patients, except patient No 2, have already been described in the 1-month morbidity section. In this latter section, four other patients had 1- month morbidity (mRS score >2). Among them, the clinical status of three patients improved between 1 month and 1 year follow-up (two patients from mRS score 3 to 2, and one patient from mRS score 3 to 1). The fourth patient was not evaluated at 1 year according to the predefined study methodology as they did not have the WEB device implanted.
Summary
A summary of the overall data is as follows:
0% rebleeding rate at 1 month and 1 year.
3.3% periprocedural events with clinical consequences, related to the procedure and/or device, all due to periprocedural thromboembolic events.
0% WEB-related 1-month and 1-year mortality.
0% WEB-related 1-month and 1-year morbidity.
Overall 1-month mortality: 1.7 %/overall 1-year mortality: 3.8%.
Overall 1-month morbidity: 15%/overall 1year morbidity: 9.6%.
Discussion
The CLARYS study demonstrates that the WEB device is safe and effective in the treatment of ruptured bifurcation aneurysms, as shown by the fact that there was no target aneurysm rebleeding within 30 days of follow-up, up to 1 year, in any of the 56 cases treated. Treatment with the WEB was feasible (93.3% technical success rate) with a low device-related complication rate (3.3%) and low overall 1-month mortality rate (1.7%). The 1-month death that did occur in this cohort was adjudicated as related to the underlying disease condition and unrelated to the device itself. Another patient died 2.5 months after the hemorrhage without ever bleeding again and their death was not related to the WEB.
Protection against rebleeding
The CLARYS protocol was carefully designed to detect any rebleeding during the month after the endovascular treatment of a ruptured aneurysm using the WEB and, to our knowledge, this is the first study to look at this rigorously. This absence of early bleeding is a fundamental element to emphasize considering that the principle of operation of the WEB is to promote a progressive thrombosis of the aneurysmal sac secondary to the endosaccular flow disruption. It is an encouraging factor for its use in the acute stage for the treatment of ruptured aneurysms. This is a fundamental point, to be put into perspective in comparison with the effectiveness of currently available treatments, including endovascular coiling. The only important drawback is the small size of our population compared with the large studies already published.
Molyneux et al 2 reported rebleeding rates of 1.9% after the first procedure and before 30 days in 1073 patients with ruptured intracranial aneurysms treated with endovascular coiling in the International Subarachnoid Aneurysm Trial (ISAT). Of course, the comparison must be weighted: ISAT was a randomized study with a large number of patients in comparison with the number in our study. The treatments were performed 25 years ago, but the fundamentals of today’s endovascular treatment existed even then: use of coils, remodeling technique, subtractive angiography, and 3D imaging. All other endovascular innovations —whether stents or flow diverters—are generally not used in the emergency setting. So the comparison still makes sense, because the CLARYS study is the first study to specifically and rigorously investigate protection against acute rebleeding.
The absence of rebleeding in ruptured aneurysms following treatment with WEB was previously reported. Caroff et al 15 were the first to report their single-center experience of the use of the WEB in ruptured aneurysms, and observed no rebleeding between discharge and the 3-month follow-up in any of their six treated patients. van Rooij et al 17 then investigated a single-center cohort of 100 patients with ruptured aneurysms who were treated with the WEB, and also found no rebleeding during the 3 to 6 months of follow-up.
Technical success rate and procedure times
In this study, treatment using the WEB device alone was performed in 53 cases (88.3%) despite the use of larger microcatheters (from 0.021 to 0.033 in) than those used to coil aneurysms (0.017 in). Coiling of the aneurysm was performed in four cases when WEB placement was deemed impossible or unsatisfactory. Adjunctive devices, including one balloon and two stents, were successfully used to manage protrusion of the device in the parent artery. No technical complications or adverse events were observed with the adjunctive use of balloons and stents. This preliminary evidence demonstrates that the adjunctive use of balloon and stent placement with the WEB device is feasible, with an acceptable safety profile; the use of the balloon to assist in WEB placement has recently been described by Mihalea et al.21
As no components of the WEB protrude outside of the aneurysm, patients are not required to remain on dual antiplatelet therapy after the implantation procedure. Compared with a coiling procedure that requires multiple devices, the WEB procedure requires only one device, leading to fast procedure time (mean procedure time of 1 hour 15 min) and low radiation exposure (mean fluoroscopy time of 27 min). These excellent times were obtained despite the anatomical difficulty of treating these aneurysms, particularly because of their location on bifurcations and the large width of their necks (dome-to-neck ratio <2 in 88% of the aneurysms).
Perioperative thromboembolic complications
In our series, the rate of intraoperative complications and postoperative morbidity/mortality compares favorably with that of large series of patients with ruptured aneurysms treated with coiling. Thromboembolic events, either with or without perfusion deficits, were the most frequent intraoperative complication observed in this study.
Thus, 16.7% of the periprocedural events that were observed, with or without clinical consequences, were thromboembolic complications. This rate of thromboembolic events is comparable to that (13.3%) reported in the CLARITY study, which assessed endovascular coiling treatment for ruptured aneurysms in 782 patients.22 It should be remembered that this complication rate increased with the width of the neck: when the neck was >4 mm (which represents 60% of the population in CLARYS), the thromboembolic complication rate in CLARITY increased to 20.8%.1 In the ARETA study,6 thromboembolic complications were the most frequently encountered (10.4% of the 753 ruptured aneurysms treated by coiling) and were more frequent for aneurysms located on the MCA bifurcation (18.5% vs 8.3% for the other locations). This location is encountered 20.3% in ARETA vs 38.3% in CLARYS.
The rates of thromboembolic complications reported to date in single-center series of ruptured aneurysms treated with the WEB is highly variable: Caroff et al 15 reported 33% in a preliminary series including only six patients; van Rooij et al 17 reported 9% but it is not known if all angiographic complications even those without clinical consequences were included; and Liebig et al 16 reported 9.6% but this is again a retrospective series.
Fortunately, only two patients had a clinical impact from thromboembolic complications related to the procedure or WEB (3.3%). This confirms that the thromboembolic complications are ultimately the prerogative of endovascular treatment of aneurysms, much more so than bleeding complications secondary to intraoperative aneurysm rupture (0% in the CLARYS study).
Perioperative rupture
The 3.3% risk of a rupture during WEB placement is low, similar to the risk for non-ruptured cases,23 and also comparable to CLARITY (4.4%)22 and ARETA (3.1%),6 suggesting a non-device-specific iatrogenic etiology for this complication. It confirms the incredibly high safety of the device.
Other complications
Vasospasm was another frequent intraoperative complication in the CLARYS study: angiographic vasospasm was observed in 3 patients (5%) and clinical vasospasm was observed in one patient (1.7%), resulting in a total vasospasm rate of 6.7%. It was lower than the vasospasm rate reported for coiling procedures,24 25 probably due to an overall low Hunt and Hess score in CLARYS, since a Hunt and Hess score greater than III was an exclusion criterion.
Limitations
Our study had some limitations. First, the number of patients treated was relatively small. Second, CLARYS did not collect all ruptured aneurysms but only those treated by the WEB because the purpose of the study was not to determine the place of WEB in the treatment of ruptured aneurysms but to determine whether WEB protects against rebleeding. Third, this was a single-arm, not randomized study. It would be challenging to directly compare the results of WEB with other techniques in treating ruptured bifurcation aneurysms. However, it is the first Good Clinical Practice study dedicated to ruptured bifurcation aneurysms treated with the WEB.
Conclusions
With a zero rate of rebleeding at 1 month and also at 1 year, the results of CLARYS are extremely encouraging for use of the WEB in the treatment of ruptured aneurysms, allowing protection against early and mid–late rebleeds.
The importance of these promising results could lead to a significant change in our practices for the endovascular treatment of ruptured bifurcation aneurysms, which has been based for the past 30 years on treatment with either clip or coils.
Of course, before any efficacy statement is made, it is essential to confirm this clinical efficacy by an evaluation of the mid-term angiographic efficacy. We have also been able to confirm a high success rate and a low complication rate, which allows rapid procedures and broadens the range of aneurysms suitable for endovascular treatment. One-year follow-up with imaging results is ongoing to supplement the encouraging clinical outcomes.
Supplemental material
Data availability statement
Data are available upon reasonable request. All data available upon request.
Ethics statements
Patient consent for publication
Ethics approval
The study received national regulatory authorization following each country’s requirement: In France, the study was approved by CCTIRS (Advisory Committee on Information Processing in Health Research) and declared to the CNIL (National Commission for Information Technology and Civil Liberties); no ethics committee or institutional review board approval was required under French regulations. In Germany, the study was approved by local ethics committees of each participating centers except Berlin which did not require new submission. The ethics committees are: Ethikkommission Medizinische Fakultät Heidelberg, Ruhr Universität Bochum Ethik-Kommission der Medizinischen Fakultät, Ethik-Kommuission der Arztekammer Hamburg Körperschaft des Offentlichen Rechts and Fachbereich-Medizin Frankfurt Goethe Universität Ethik-Kommission; the process did not include ID of the approvals.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @jildazz, @Fie0815, @CRISTIANMIHALEA
Contributors All authors have provided a substantial contribution to the conception and design of the studies and/or the acquisition and/or the analysis of the data and/or the interpretation of the data; drafted the work or revised it for significant intellectual content; approved the final version of the manuscript; agree to be accountable for all aspects of the work, including its accuracy and integrity.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests JF acts as associate editor of the Journal of NeuroInterventional Surgery; MM acts as a member of the editorial board of Neuroradiology. LS: consultant for Microvention, Balt, Phenox, Stryker, Medtronic, PI for CLARYS, grant or contract from Philips with institution; DH: consultant for Microvention; XB: consultant for Microvention; JF: Consultant for Medtronic, Microvention, and Cerus; VCo: consultant for Microvention, educational grant and research grant with payment to institution; TL: consultant for Microvention/Sequent Medical, Stryker, Medtronic, and Cerus; MM: consultant and expert testimony for Medtronic, Microvention, and Stryker with payment to institution; WW: payment or honoraria for proctoring and lectures from Microvention; CC: consultant for Microvention, MIVI, Stryker, and Cerenovus; J-HB: payment or honoraria for proctoring and lectures from Microvention; MB: consultant for Microvention, Cerenovus, Acandis, and Rapid; GB: support for travel from Microvention; SF: honoraria for lecture and data preparations regarding WEB; AB: consultant for Microvention; JM: consultant for Microvention. LP: consultant for Microvention, Balt, Perflow, Phenox, Vesalio, clinical event adjudicator for CLARYS; JBy: core laboratory reviewer for CLARYS.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.