Article Text

Abstract
Background Sex disparities in acute ischemic stroke outcomes are well reported with IV thrombolysis. Despite several studies, there is still a lack of consensus on whether endovascular thrombectomy (EVT) outcomes differ between men and women.
Objective To compare sex differences in EVT outcomes at 90-day follow-up and assess whether progression in functional status from discharge to 90-day follow-up differs between men and women.
Methods From the Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT) prospective cohort study (2016–2018), adult men and women (≥18 years) with anterior circulation large vessel occlusion (internal carotid artery, middle cerebral artery M1/M2) treated with EVT up to 24 hours from last known well were matched using propensity scores. Discharge and 90-day modified Rankin Scale (mRS) scores were compared between men and women. Furthermore, we evaluated the improvement in mRS scores from discharge to 90 days in men and women using a repeated-measures, mixed-effects regression model.
Results Of 285 patients, 139 (48.8%) were women. Women were older with median (IQR) age 69 (57–81) years vs 64.5 (56–75), p=0.044, had smaller median perfusion deficits (Tmax >6 s) 109 vs 154 mL (p<0.001), and had better collaterals on CT angiography and CT perfusion but similar ischemic core size (relative cerebral blood flow <30%: 7.6 (0–25.2) vs 11.4 (0–38) mL, p=0.22). In 65 propensity-matched pairs, despite similar discharge functional independence rates (women: 42% vs men: 48%, aOR=0.55, 95% CI 0.18 to 1.69, p=0.30), women exhibited worse 90-day functional independence rates (women: 46% vs men: 60%, aOR=0.41, 95% CI 0.16 to 1.00, p=0.05). The reduction in mRS scores from discharge to 90 days also demonstrated a significantly larger improvement in men (discharge 2.49 and 90 days 1.88, improvement 0.61) than in women (discharge 2.52 and 90 days 2.44, improvement 0.08, p=0.036).
Conclusion In a propensity-matched cohort from the SELECT study, women had similar discharge outcomes as men following EVT, but the improvement from discharge to 90 days was significantly worse in women, suggesting the influence of post-discharge factors. Further exploration of this phenomenon to identify target interventions is warranted.
Trial registration number NCT02446587.
- thrombectomy
- intervention
- stroke
- CT perfusion
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Statistics from Altmetric.com
Introduction
Disparities in health and stroke-related outcomes between the sexes has been a longstanding area of interest to healthcare systems worldwide.1–5 Women, known to live longer than men, have been shown to have higher rates of disability and worse quality of life than men after acute ischemic stroke.6 7 Studies evaluating sex disparities in stroke treatments show lower rates of intravenous thrombolytic use8 and risk factor reduction therapies in women.1 In patients with large vessel occlusion (LVO) undergoing endovascular thrombectomy, these disparities in outcome have been controversial.9–13 While a subgroup analysis from MR CLEAN (Multicenter Randomized CLinical trial of Endovascular treatment for Acute ischemic stroke in the Netherlands) trial found that only men experienced a major benefit from endovascular thrombectomy (EVT),9 a larger, pooled analysis of seven multicenter randomized clinical trials including MR CLEAN found that women derive similar benefit and good outcomes after EVT as men do relative to their respective controls.10 When men and women who have undergone EVT are compared, some studies have found that women are less likely than men to be independent at 90 days,11 12 while others found similar 90-day disability rates.13 These studies also did not adjust for important baseline clinical or imaging characteristics9–11 13 or recovery following hospital discharge9–13 while evaluating whether there are disparities in functional outcomes at 90-day follow-up.
It is also unclear whether the disparities in outcomes are related to differences in baseline clinical or imaging characteristics, response to the intervention, or recovery following hospital discharge. Women are generally older when they have their first stroke. Furthermore, baseline differences in imaging characteristics and vessel diameter with their effect on stroke outcomes by sex have been reported.14 Additionally, sex-specific responses to rehabilitation15 and sex-related differences in clinical, psychological, and social factors15 16 that may affect functional improvements during the post-acute phase have also been described previously.
In this hypothesis-generating, secondary analysis of the Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT) prospective cohort study, we sought to evaluate the differences in EVT outcomes as measured by discharge and 90-day modified Rankin Scale (mRS) scores between men and women, and determine whether progression of functional status from discharge to 90-day follow-up beyond discharge is associated with the sex of the patient.
Methods
The data that support the findings of this study are available from the corresponding author on reasonable request.
Study design and participants
This is a secondary analysis of a prospective, multicenter cohort study of imaging selection, ‘Optimizing Patient Selection for Endovascular Treatment in Acute Ischemic Stroke (SELECT): a prospective multicenter cohort study of imaging selection’ (NCT02446587). The study population, methodology, and primary results of the SELECT trial have been published.17 18 Patients with acute ischemic stroke and anterior circulation LVO who presented up to 24 hours from symptom onset at nine US study sites were enrolled between January 2016 and February 2018. Major inclusion criteria for the study were (1) adults ≥18 years with acute ischemic stroke, (2) National Institutes of Health Stroke Scale (NIHSS) score ≥6 at presentation, (3) LVO on CT angiography (CTA) in anterior circulation (in the internal carotid artery (ICA), middle cerebral artery (MCA) M1/M2 segments), and (4) no or minimal deficits at baseline (mRS score 0–1). All patients received a standardized pre-thrombectomy imaging protocol with non-contrast CT, CTA, and CT perfusion with automated processing using RAPID software (iSchemaView, Menlo Park, California, USA). Imaging studies were evaluated by an independent neuroimaging core laboratory blinded to clinical outcomes and enrollment site. Decision to proceed with thrombectomy versus medical management alone was at the discretion of the site investigators. All patients received best medical management as defined by the contemporary American Heart Association/ American Stroke Association guidelines, including use of IV thrombolysis with alteplase within 4.5 hours of last known well if applicable.19 Endovascular thrombectomy constituted attempted clot retrieval using a stent retriever, aspiration device, or a combination thereof. For the purpose of this analysis, men and women were matched based on baseline clinical and imaging characteristics to compare study outcomes.
Ethical approval disclosure
The study protocol was approved by the institution review board (IRB) at each participating site prior to the start of the study, and it was registered at ClinicalTrials.gov (NCT02446587). The ethical committees that approved the study are: UT McGovern Medical School – Houston, Texas - UT Committee for Protection of Human Subjects (HSC-MS-15–0337); Emory University – Atlanta, Georgia: Emory University IRB (CR1_IRB00083782); Florida Hospital – Orlando, Florida: Florida Hospital IRB (6 99 641–2); Stanford University, Palo Alto, California - Stanford IRB (37774); St Louis University – St Louis, Missouri - SLU IRB (26092); Kansas University – Kansas City, Kansas: KUMC IRB (IRB00000161); Valley Baptist Hospital – Harlingen, Texas - MetroWest Medical Center IRB (2015–095); Riverside Methodist Hospital – Columbus, Ohio: WIRB (1160694); and WellStar Health System - Marietta, Georgia: WIRB (1162531). All study participants or their legally authorized representatives provided written informed consent prior to data entry into the SELECT database up to 7 days after the procedure.
Imaging evaluation
The imaging evaluation included preprocedure CT Alberta Stroke Program Early CT Score (ASPECTS), modified collateral score, CT perfusion (cerebral blood flow, Tmax maps), hypoperfusion intensity ratio (Tmax >10 s volume/Tmax >6 s volume), modified Thrombolysis in Cerebral Infarction20 on cerebral angiogram, and final infarct volume, as measured on postprocedure DWI sequences using manual segmentation of the region of interest. If postprocedure MRI was not available, final infarct volume was measured on non-contrast CT.
Study outcomes
The primary outcome was the 90-day mRS score, assessed by reviewers, blinded to treatment allocation and imaging findings, in-person (preferred) or over a phone call if an in-person visit was not feasible. Functional independence, defined as mRS score of 0–2 was also evaluated. Safety endpoints included symptomatic intracerebral hemorrhage, defined as worsening of NIHSS score of 4 or more with evidence of any intracerebral hemorrhage on follow-up imaging,21 neurological worsening defined as worsening of NIHSS score of 4 or more at 24 hours from presentation NIHSS score, and mortality at 90 days. The difference between functional status at discharge and at 90-day follow-up as measured by mRS was also evaluated.
Statistical analysis
Patients who received EVT were stratified by sex; their baseline clinical and imaging characteristics were described and compared. Univariable comparisons were made using Pearson’s Χ2 test or Fisher’s exact test for categorical variables and Student’s t-test or Wilcoxon rank sum test for continuous variables, where appropriate. A propensity-matched analysis was also undertaken, using age, NIHSS score, time from last known well to procedure, occlusion location, ischemic core volume, hypoperfusion intensity ratio, collaterals score, coronary artery disease congestive heart failure and atrial fibrillation history to ensure a balanced 1:1 sample of men and women, using nearest neighbor match for probability of characteristics associated with sex. Since there was a high degree of correlation between ischemic core at baseline and penumbra (Tmax >6 s) at baseline, only ischemic core at baseline was used to create the model for calculation of propensity scores.
Difference in functional outcome by sex was evaluated using multivariable ordinal logistic regression models adjusting for potential confounders—age, race, NIHSS score at presentation, serum glucose, IV tissue plasminogen activator status, transfer status, ischemic core volume, clot location, time from last known well to groin puncture, time from groin puncture to reperfusion/end of the procedure, and discharge disposition. Point estimates and 95% confidence intervals were reported for common OR. Effect of sex on functional independence (mRS score 0–2) was also assessed using a multivariable logistic regression model with the aforementioned covariates, and OR with 95% CI was reported.
To evaluate the improvement from discharge to 90-day follow-up in mRS scores in men and women, we analyzed how mRS score at discharge and at 90-day follow-up changed using a repeated-measure, mixed-effects regression model with a linear approximation of mRS scores. Predicted mRS scores (estimated marginal means) with p value for interaction terms were reported to identify if the improvement in mRS scores from discharge to 90-day follow-up differs between the two sexes.
STATA 15 (StataCorp. 2017. Stata Statistical Software: Release 15. College Station, Texas: StataCorp LLC.) was used for all statistical analyses. All p values were two-sided and p<0.05 was considered statistically significant.
Results
Clinical and imaging baseline characteristics: comparison by sex
Of 361 patients enrolled in the SELECT study, 285 received EVT and were included in the analysis. 146 (51.2%) were men and 139 (48.8%) were women. A summary of baseline clinical and imaging characteristics of the overall cohort of patients receiving EVT stratified by sex is provided in table 1. Women included in the study cohort were older (median years (IQR) 69 (57–81) vs 64.5 (56–75), p=0.044), had lower prevalence of coronary artery disease (women: 14.7% vs men: 26.6%, p=0.015) and a higher prevalence of atrial fibrillation (women: 40.6% vs men: 26.9%, p=0.015). IV thrombolysis rates did not differ; 68.5% of men as compared with 62.6% of women received IV tissue plasminogen activator (p=0.29). There were no differences in time from last known well to arrival at an EVT-capable hospital (men: 2.10 hours (IQR 0.90–3.90) vs women: 2.50 (1.08–4.33), p=0.12) and in stroke severity (NIHSS score) at presentation (men: 16 (12–20) vs women: 17 (11–22), p=0.44].
Baseline characteristics in SELECT population treated with endovascular thrombectomy (EVT)
There were significant differences in imaging characteristics. While the median ASPECTS on non-contrast CT did not differ significantly between the two groups (men: 8 (7–9) vs women: 8 (7–9), p=0.87) and median ischemic core size was numerically smaller in women (men: 11.4 (0–38) mL vs women: 7.6 (0–25.2) mL, p=0.22); critically hypoperfused tissue (Tmax >6s) volume was significantly smaller in women (men: 154 (104–198) mL vs women: 109 (66–151.2) mL, p<0.001). The collaterals on CTA were similar (median (IQR) modified collateral scores: men 1 (1–2) vs women 2 (1–3), p=0.13), while collaterals on perfusion imaging, measured as hypoperfusion intensity ratio, were significantly better in women (men 0.51 (0.37–0.63) vs women 0.41 (0.25–0.56), p<0.001). The rates of achieving successful reperfusion after EVT were similar (men: 121 (82.9%) vs women: 114 (82.0%), p=0.85).
Propensity-matched analysis: baseline characteristics
In a propensity-matched analysis, women and men were matched on age, NIHSS score, serum glucose at presentation, coronary artery disease, congestive heart failure, atrial fibrillation, clot location, ischemic core volume, hypoperfusion intensity ratio, collateral scores, and time from last known well to procedure. A total of 65 matched pairs were identified. A summary of the baseline characteristics of these matched pairs is provided in table 2. After propensity matching, there were no differences in age (men: 64 (IQR 54–74) vs women: 67 (52–76), p=0.56), presentation NIHSS score(men: 15 (12–20) vs women: 16 (10–20), p=0.76), ASPECTS (men: 8 (7–9) vs women: 8 (7–9), p=0.71), or ischemic core volume (men: 6 (0–21) vs women: 12 (0–25), p=0.30). However, critically hypoperfused tissue (Tmax>6s) volume was smaller in women (men: 131 (94–200.1) mL vs 109 (66–141) ml, p=0.007).
Baseline characteristics in a propensity-matched SELECT population treated with endovascular thrombectomy (EVT)
Propensity-matched cohort: comparative outcomes
Table 3 provides the clinical and imaging outcomes in matched pairs of men and women. The rates of functional independence at discharge (men: 31 (48%) vs women: 27 (42%), p=0.48) did not differ between the two groups. The distribution of functional outcomes at discharge did not differ (men: 3 (1–4) vs women: 3 (1–4), p=0.77). In multivariable analysis, no significant difference was observed in functional independence (aOR=0.55 (95% CI 0.18 to 1.69), p=0.30) or distribution of functional outcomes (common OR=0.86, 95% CI 0.44 to 1.71, p=0.67) between men and women. Safety outcomes were similar (neurological worsening—men: 11% vs women: 8%, p=0.62; symptomatic intracerebral hemorrhage—men: 8% vs women: 5%, p=0.72; in-hospital mortality—men: 2% vs women: 6%, p=0.37).
Clinical outcomes in a propensity-matched SELECT population treated with endovascular thrombectomy (EVT)
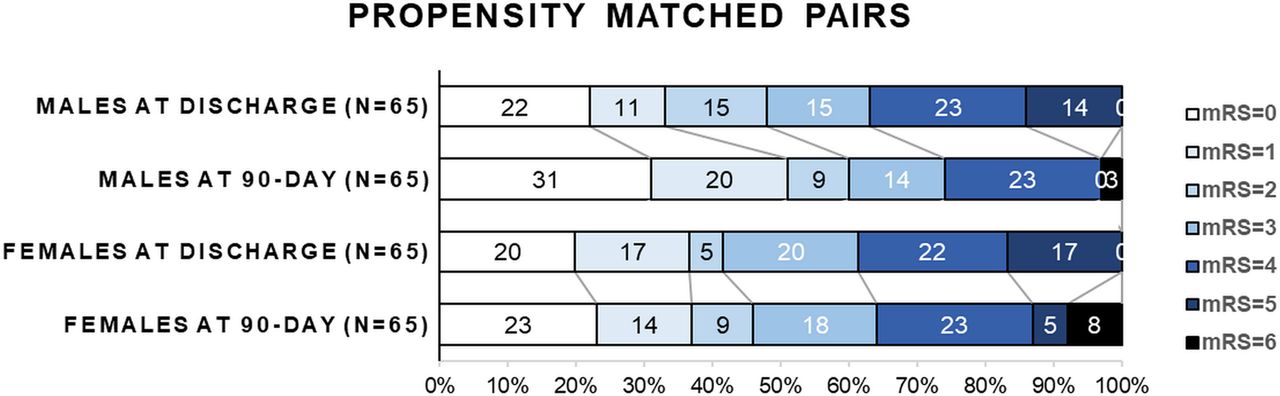
However, at 90-day follow-up, women demonstrated numerically worse functional independence rates (women: 46% vs men: 60%, aOR=0.41, 95% CI 0.16 to 1.00, p=0.05) and a significant ordinal shift towards worse functional outcomes in women (adjusted cOR=0.49, 95% CI 0.25 to 0.96, p=0.04) was observed. Additionally, the distribution of functional outcomes (men: 1 (0–4) vs women: 3 (1–4), p=0.09) demonstrated a trend towards statistical significance. The 90-day mortality did not differ (men: 2 (3%) vs women: 5 (8%), p=0.44). Figure 1 demonstrates the distribution of functional outcomes on mRS score in men and women at discharge and at 90-day follow-up in the propensity-matched cohort.

Distribution of modified Rankin Scale (mRS) scores at discharge and 90-day follow-up, stratified by sex in propensity-matched SELECT population treated with endovascular thrombectomy. While the distribution of mRS scores did not differ at discharge (adjusted common OR (cOR)=0.86, 95% CI 0.44 to 1.71, p=0.67), 90-day mRS scores were significantly worse in women (cOR=0.49, 95% CI 0.25 to 0.96, p=0.04).
The improvement in predicted mRS score from discharge to 90-day follow-up differed significantly by sex, with men exhibiting a significantly larger improvement (at discharge: 2.49, at 90-day follow-up: 1.88 for an improvement of 0.61) as compared with women (at discharge: 2.52, at 90-day follow-up: 2.44 for an improvement of 0.08, p=0.036). Figure 2 illustrates the predicted mRS scores for men and women at discharge and how they change at 90-day follow-up, both unadjusted and adjusted for potential covariates.

{kind=link}
{kind=link}
Predicted improvement in modified Rankin Scale (mRS) scores from discharge to 90-day follow-up. In a propensity-matched SELECT cohort treated with endovascular thrombectomy, women demonstrate a significantly lower reduction in mRS scores than men: (A) in an unadjusted model, and (B) In a model adjusted for baseline differences and potential clinical and imaging confounders.
Discussion
In a propensity-matched cohort of 65 pairs in this secondary analysis from the SELECT prospective cohort study, although there was no difference in the functional independence rate at discharge, men had a higher rate of 90-day functional independence than women. Additionally, the improvement from discharge to 90 days by the reduction in predicted mRS score during this interval was significantly larger in men than in women.
Multiple studies have attempted to examine sex disparities and EVT outcomes.9–13 However, very few manuscripts have discussed post-discharge progression after EVT based on sexes. This manuscript represents the first analysis based on such approach using multicenter data. Also, we acknowledge and account for significant imaging differences observed between men and women due to the natural history of the disease. Furthermore, our study dataset represents the pragmatic, real-world practice from nine high-volume EVT centers in the USA.
Participation of women in large randomized controlled trials assessing endovascular thrombectomy is a topic of importance with a significant geographic variation, showing a higher proportion of representation of women in predominantly North American trials—SWIFT PRIME (52%), DAWN (55%), and DEFUSE 3 (51%), and comparatively lower in predominantly European trials—MR CLEAN (42%) and REVASCAT (47%).22–26 The differences in participation add to the limitations of the studies evaluating EVT outcomes and treatment effect disparities by sex across the world that originated from these trials and further quantifies the need for an unbiased assessment of the impact of sex on EVT outcomes and treatment effect.
Similarly, prior reports on EVT outcomes and potential treatment effect by sex have been conflicting. A subanalysis from the HERMES patient-level meta-analysis showed similar treatment effect of thrombectomy by sex,27 while an analysis from MR CLEAN data showed better outcomes in men.9 In a post hoc analysis of the DEFUSE 3 trial, 35% of women but 54% of men who underwent EVT in the late window were functionally independent at 90 days.12 Another analysis that combined data from the SWIFT (Solitaire With the Intention For Thrombectomy), STAR (Solitaire Thrombectomy for Acute Revascularization), and SWIFT PRIME (Solitaire With the Intention For Thrombectomy as Primary Endovascular Treatment) cohorts reported similar functional independence rates between men and women at 90 days and found that women had more years of optimal life (disability-adjusted life year) after EVT.28 Differences in EVT outcomes when comparing men to women in these studies may in part be due to differences in the baseline clinical and imaging characteristics, as well as the design and enrollment criteria for the individual trials. There are baseline clinical and imaging characteristics that demonstrate significant differences between two sexes due to natural history of the stroke. Thus, women generally present later in life, and have significantly different imaging characteristics.12 Our study differs from the aforementioned analyses evaluating effect of sex on EVT outcomes as we attempted to account for these differences by using a propensity-matched cohort. Furthermore, we evaluated outcomes at discharge and 90-day follow-up, but also characterized how the improvement from discharge to 90-day follow-up differs between the two sexes.
In our cohort, women had smaller perfusion deficit, better collaterals, and smaller core infarct at presentation. Additionally, women had a trend towards smaller follow-up infarct volumes after EVT in spite of similar successful reperfusion rates. The comparison of imaging characteristics by sex in the DEFUSE 3 trial12 was consistent with our findings as women had better collaterals, smaller presentation core volumes, and slower infarct growth than men. Women, however, still had lower functional independence rates in DEFUSE 3. This highlights the importance of factors other than reperfusion, such as baseline imaging and clinical variables, that might affect thrombectomy outcomes. To mitigate the impact of potential baseline clinical and imaging factors, we performed a propensity-matched analysis and found better improvement in men from discharge to 90-day follow-up than in women. A prior single-center study also reported similar functional independence rates at discharge, but less likelihood of women being independent at 90 days.29 That study, however, included patients with both anterior and posterior circulation LVO and allowed for patients with baseline disability (mRS score >2) in the analysis. These findings highlight potential disparities in post-discharge care between men and women. Although the discharge disposition did not differ between the two sexes in our study, it is plausible that several social, psychological, and physical factors affected the post-discharge recovery of women as compared with men, suggesting the need for more comprehensive surveillance of post-discharge health status in patients receiving EVT.
Women were older in our cohort. Frailty renders older individuals more prone to adverse health outcomes, and women are shown to be disproportionately affected by frailty.30 31 Prior studies have demonstrated that women had higher frailty at the time of stroke incidence, leading to worse outcomes.32
Women and men in our cohort had similar discharge rates to acute inpatient rehabilitation. Prior reports showed better response to acute rehabilitation in women than in men. However, other potential factors, including higher rates of social isolation with consequent negative effects on outcomes,33 might have contributed to women having lower improvement rates with post-stroke rehabilitation. In the animal models, social isolation was associated with poor functional recovery after stroke.34 According to 2010 census data, 51% of women versus 71% of men over the age of 55 have a spouse present at home.35 Studies have also shown that women are at a higher risk of experiencing widowhood than men,36 which might contribute to worse post-stroke cognitive outcomes in women.37
Moreover, with post-stroke depression being a significant risk factor for worse outcomes, the severity of depressive symptoms has been found to be greater in women following stroke.38 39
The differential natural history of stroke based on sex means that there will be differences in the clinical characteristics of men and women participating in acute ischemic stroke trials, which may eventually affect their short and long-term clinical outcomes. Our study demonstrated significantly different post-discharge progression after EVT in a matched prospective cohort, presenting at nine high-volume EVT centers across the USA. This may highlight the need to actively identify potential sex-related disparities and measures to minimize them in longitudinal studies to prevent potential bias affecting clinical trials evaluating EVT outcomes and treatment benefits, including provision of external support and standardization of secondary stroke prevention and post-stroke rehabilitation.
Post-discharge longitudinal studies are necessary to assess the frequency and duration of rehabilitation and the psychobehavioral, socioeconomic, and biological factors that affect the benefit from rehabilitation and post-discharge improvement after thrombectomy. These studies would assess these influences on sex/gender disparities and provide insights on potential interventions to maximize post-discharge recovery after thrombectomy.
The SELECT trial was primarily designed to evaluate imaging profiles and their effect on functional and safety outcomes after acute ischemic stroke, but the presence of significant differences in various imaging characteristics between men and women based on the natural history of stroke, together with prospective design and consecutive enrollment of patients at nine high-volume EVT centers in the USA, make the data unique in its ability to evaluate the question under consideration.
Our study has several limitations. This was a retrospective secondary analysis from a prospective cohort study, and thus might have carried the potential inherent limitations of these types of analyses. As the study represent an analysis of non-randomized data, we refrained from evaluating sex differences in EVT treatment effect. Furthermore, the SELECT trial enrolled patients between January 2016 and February 2018. Recent advances in the field of post-discharge care for acute ischemic stroke, including remote delivery of rehabilitation through telemedicine, might affect the findings of the study. We also did not evaluate the effect of stroke laterality on potential post-discharge progression. Insurance status and disposition at 90-day follow-up was not available for analysis. Additionally, we lacked the sociobehavioral, socioeconomic, and psychological variables that might have explained the differences in outcomes. Clinical and imaging characteristics were significantly different between men and women and might have influenced the outcomes. To reduce the influence of these factors a propensity-matched analysis was preferred and executed. Despite this, our hypothesis-generating study sheds light on the potential differences in post-thrombectomy improvement in women as compared with men with the potential disparities in post-acute stroke care by sex.
Conclusion
In a propensity-matched cohort of men and women from the SELECT study, women had similar discharge outcomes to those of men following EVT. The improvement from discharge to 90-day follow-up, however, was significantly worse in women, suggesting the influence of factors affecting post-discharge recovery. Further exploration of this phenomenon to identify targeted interventions is warranted.
Supplemental material
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by UT McGovern Medical School – Houston, Texas - UT Committee for Protection of Human Subjects (HSC-MS-15-0337), Emory University – Atlanta, Georgia: Emory University IRB (CR1_IRB00083782); Florida Hospital – Orlando, Florida: Florida Hospital IRB (699641-2), Stanford University, Palo Alto, California - Stanford IRB (37774); St. Louis University – St. Louis, Missouri - SLU IRB (26092), Kansas University – Kansas City, Kansas: KUMC IRB (IRB00000161); Valley Baptist Hospital – Harlingen, Texas - MetroWest Medical Center IRB (2015-095); Riverside Methodist Hospital – Columbus, Ohio: WIRB (1160694); and WellStar Health System - Marietta, Georgia: WIRB (1162531). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
This study was a secondary analysis of the SELECT trial data. The authors would like to acknowledge the contribution from the site investigators and coordinators, who supported the enrollment in the SELECT trial at UT McGovern Medical School – Houston, Texas; Emory University – Atlanta, Georgia; Florida Hospital – Orlando, Florida; Stanford University, Palo Alto, California; St Louis University – St. Louis, Missouri, Kansas University – Kansas City, Kansas; Valley Baptist Hospital – Harlingen, Texas; Riverside Methodist Hospital – Columbus, Ohio; and WellStar Health System - Marietta, Georgia.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @Faris_Shaker, @amrsarrajMD
Contributors ASa designed and conceptualized the research and provided administrative and material support and as a guarantor accepts full responsibility for the work and/or the conduct of the study, had access to the data, and controlled the decision to publish. ASa, JTF, and TNN drafted the manuscript. DKP contributed to the data analysis. SS, ASh, FS, LEF, EMJ, CGL, SJS, NLI, MVD, SM-S, JS, JPT, AWA, and SIT provided ciritical revisions of the manuscript for important intellectual content.
Funding The SELECT trial (Optimizing Patient’s Selection for Endovascular Treatment in Acute Ischemic Stroke) was funded by Stryker Neurovascular through a grant to UT McGovern Medical School.
Competing interests ASa reports serving as the principal investigator of the SELECT (Optimizing Patient’s Selection for Endovascular Treatment in Acute Ischemic Stroke) and SELECT-2 trials through a grant from Stryker Neurovascular to University of Texas McGovern–Houston; as a consultant, speaker bureau member, and advisory board member for Stryker; and as a site principal investigator for the TREVO Registry and DEFUSE 3 trials (Endovascular Therapy Following Imaging Evaluation for Ischemic Stroke). JTF is a member of the editorial boards of the Journal of NeuroInterventional Surgery (JNIS), and reports receiving consulting fees from Stryker outside this research work. SIT is an editorial board member of JNIS. TNN reports receiving research support from Medtronic and the Society of Vascular and Interventional Neurology outside this work.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.