Article Text

Abstract
Background Endovascular treatment of intracranial vascular diseases, such as aneurysms, is often challenged by unfavorable vascular anatomy. The Bendit Steerable Microcatheter (Bendit Technologies, Tel Aviv, Israel) has bending and torqueing capabilities designed to improve navigation and stability during device delivery, with or without a guidewire. We describe our preclinical experience with the Bendit 17 and Bendit 21 microcatheters in a rabbit aneurysm model.
Methods Bifurcation and side wall aneurysms were created surgically in six New Zealand rabbits. We attempted to navigate Bendit devices through the vasculature and enter the aneurysms without a guidewire. Various positions within the aneurysm were selectively explored. Angiographic imaging was used to visualize catheterization, navigation, vascular manipulations, and placement of coils, stents, and intrasaccular devices.
Results We successfully navigated the Bendit microcatheters to all aneurysms without a guidewire. We successfully recanalized a nearly occluded carotid artery and navigated the Bendit through a braided stent. In contrast, we were unable to navigate a comparator device with a guidewire as effectively as the Bendit. Coils were introduced at different locations within the aneurysm and could be pushed, pulled, and repositioned with the Bendit tip. Finally, we used the Bendit to deliver intrasaccular devices designed for terminal aneurysms to treat side wall aneurysms.
Conclusions Bendit’s bending and torqueing abilities, combined with its stability in the bent position, enable quick navigation and optimal deployment of devices. Clinical studies are necessary to determine whether these navigation advantages lead to more efficient treatment of intracranial and peripheral aneurysms.
- aneurysm
- catheter
- coil
- guidewire
- stent
Data availability statement
No data are available. Not applicable.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Navigation through unfavorable vascular anatomy and unstable device delivery are common challenges for the endovascular treatment of intracranial aneurysms.1–3 Furthermore, the most suitable microcatheter shape remains controversial.4–7 In contrast with conventional microcatheters, which have a fixed shape and cannot be altered inside of the patient, bendable and steerable microcatheters allow the user to change the angle and shape of the tip in real time. Although large steerable catheters have been used for years in cardiovascular angiography,8 9 only a few studies have discussed the potential benefits of steerable microcatheters in other applications, mostly in the liver and kidney.2 8 10–12 The Bendit Steerable Microcatheter (Bendit Technologies, Tel Aviv, Israel), which received clearance from the Food and Drug Administration in 2019 for peripheral use only, has three-dimensional controlled bending (articulating) and steering capabilities. Furthermore, the device can be used without a guidewire. This is due to the Bendit’s combined tube structure, which maintains the device’s torsional rigidity, as well as its geometry, which combines a larger internal diameter with a smaller outer diameter. The Bendit’s real time bending and torquing capabilities, coupled with its torsional rigidity, have the potential to improve the delivery of diagnostic, embolic, and therapeutic materials. While comparator microcatheters such as the Headway Duo (MicroVention) have been shown to be very trackable and useful for endovascular embolization procedures,13 they lack the real time bending and torqueing abilities of steerable microcatheters.
In this study, we provide a technical description of the Bendit microcatheters and describe our preclinical experience with the device. We investigated our ability to use the Bendit catheter to navigate through vasculature, position aneurysm coils and stents, and deploy devices for aneurysm repair using a rabbit model.
Methods
Technical description of the device
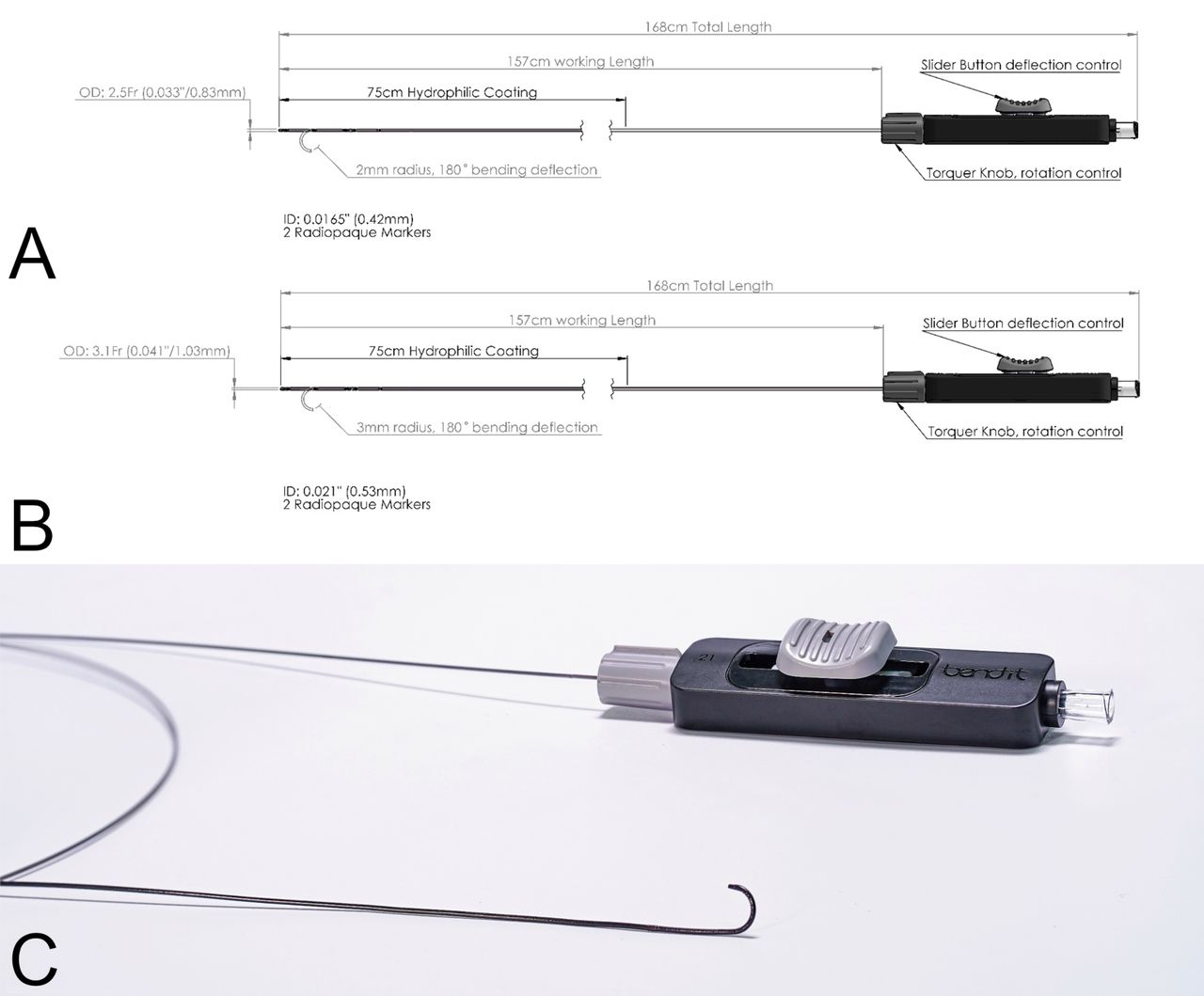
The Bendit 17 and Bendit 21 microcatheters are composed of two nitinol hypotubes connected at their distal ends and feature proprietary laser cut patterns along the 35 cm distal section (figure 1). These laser cuts give the Bendit its flexibility, while the nitinol structure (a metal alloy of nickel and titanium) allows the device to maintain its one-to-one torsional rigidity, unique to the Bendit. Both devices feature two radiopaque markers at the distal ends, 3 cm apart. The Bendit 17 has an inner diameter of 0.0165 inches (0.42 mm) and an outer diameter of 2.5 F (0.033 inches or 0.83 mm), making it suitable for use in smaller vessels. The Bendit 21 has an inner diameter of 0.021 inches (0.533 mm) and an outer diameter of 3.1 F (0.041 inches or 1.05 mm) at the level of the second marker, while it narrows to 2.9 F (0.037 inches or 0.95 mm) in the distal 3 cm after the proximal marker.

General dimensions of the (A) Bendit 17 and (B) Bendit 21 microcatheters. (C) The manual control for the Bendit. Moving the sliding button up and down bends the tip 180° in either direction. The rotating knob allows the device to be torqued.
The Bendit is maneuvered with a single manual control that can be locked at any degree of angulation, maintaining the shape while torqueing. Moving the steering slider button forward and backward deflects the tip up to 180° over a 2 or 3 mm radius (for the Bendit 17 and Bendit 21, respectively) and straightens it back into position. The working length of the two Bendit devices is 157 cm, and the distal 75 cm end of the device features a hydrophilic coating. The torque knob can be moved left and right, rotating the tip for bidirectional torqueability. The system automatically locks the microcatheter shape when the button is released, keeping it steady and stable while the tip is precisely positioned to deliver treatment. The catheter remains soft in the neutral position (ie, when tracking). The device provides support for coaxial/multiaxial telescoping. Contrast can be injected continuously with or without roadmapping.
The microcatheter tip is stable when bent; when delivering rigid devices, the catheter shape and position is maintained, straightening only when the device passes through the preshaped segment. We measured the average force to keep the tip aligned while controlling the maximum deflection, which was equal to 0.244 N±0.041 N. The maximum force with Confidence/Reliability 95/90 is 0.329 N.
Preclinical experiments
The study was approved by the committee for animal experiments from Land Salzburg, Austria (20901-TVG/136/10–2021). Six New Zealand rabbits were used for the preclinical study. In three rabbits, a bifurcation aneurysm was surgically created and allowed to mature for at least 1 month.14–16 In the remaining three rabbits, two side wall aneurysms of different sizes were surgically created in each common carotid artery and allowed to mature for at least 1 month.
We used a 6 F Terumo introducer sheath (TERUMO International Systems at the femoral artery. A 5 F Codman guide catheter (Johnson & Johnson) was used, with the Bendit 17 or 21 for coaxial catheterization of the carotid arteries. We attempted to navigate through a nearly occluded right carotid artery with both the Bendit and the Headway 21 (MicroVention) (inner diameter=0.0165 inches (0.419 mm), outer diameter=1.6 F). The nearly occluded right carotid artery occurred unexpectedly as a result of the surgical suturing, allowing us to test the ability of the Bendit 17 to cross the severe near total occlusion. We also attempted to navigate the Bendit through LVIS (MicroVention) stents deployed in the carotid artery.
Three intrasaccular devices were placed in side wall aneurysms: one WEB 17 device (MicroVention) and two 021 Contour Neurovascular System devices (Cerus Endovascular). While the Bendit 17 was used in most of our preclinical work, the Bendit 21 was used to deploy the WEB and Contour Neurovascular System devices for compatibility with the delivered devices. Angiographic imaging via conventional fluoroscopy, as well as digital subtraction angiography (DSA), was used to visualize catheterization, positioning, and the placement of coils and intrasaccular devices in different parts of the aneurysm.
Results
Catheterization
The Bendit tip could be used to pinpoint precise locations of the aneurysm using its torqueing and deflection features. Using the Bendit 17, we were able to successfully catheterize the right and left carotid arteries from the aortic arch up to the rabbit bifurcation or side wall aneurysm without the use of a conventional 0.014 inch (0.356 mm) guidewire or other guidewires; no delays or navigation failures occurred (figure 2A). The Bendit 17 tip could be successfully positioned in specific directions (eg, the 2:00 position) at a vessel bifurcation or in an aneurysm without a guidewire (figure 2B). The Bendit 17 tip could also be rotated around the entire circumference of the vessel above a side wall aneurysm with no spasm of the vessel (figure 2C).

(A) The Bendit 17 used to catheterize the left carotid artery in a rabbit bifurcation aneurysm without a guidewire. (B) The Bendit 17 tip pointed precisely at the 2:00 position without a guidewire. (C) The Bendit 17 is rotated around the entire circumference of the vessel above a side wall aneurysm without any vessel spasms.
Navigation through stents and near occlusion
We were able to maneuver the Bendit through stents and occluded vessels effectively without a guidewire. The Bendit 17 was navigated through the mesh of a braided LVIS (MicroVention) stent to reach a bifurcation aneurysm without a guidewire (figure 3A). In a maneuver that generally requires the use of an open cell stent, we were able to navigate the Bendit 17 through an LVIS Jr (MicroVention) braided stent to the tortuous left carotid artery without delays or changes to the stent position and without a guidewire (figure 3B). The stent did not appear to be disturbed in any way by this maneuver.
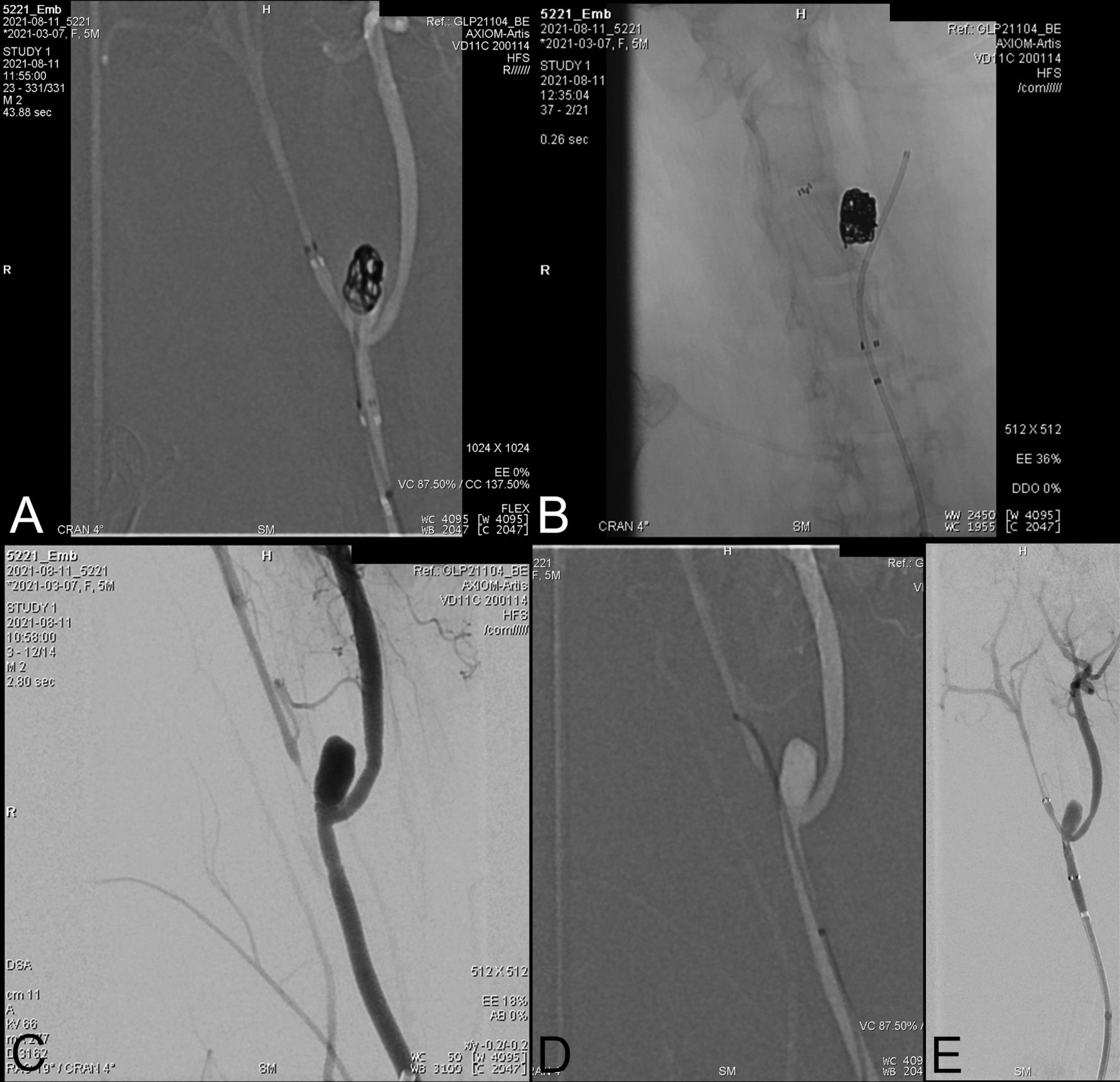
(A) The Bendit 17 can be navigated through a braided LVIS stent to reach the aneurysm, without a guidewire. (B) The Bendit 17 can be maneuvered through a braided LVIS Jr stent to enter the left carotid artery without a guidewire. (C, D) The Bendit 17 was twice able to access a nearly occluded right carotid artery and gain access to the lumen without a guidewire. The Headway 21, a comparator device with a guidewire, could not be used to cross the area of stenosis. (E) The Bendit 17 used to deploy the LVIS 4.5 stent along the right carotid artery in a steady manner.
The Bendit 17 was twice used to access a nearly occluded right carotid artery, without a guidewire to deliver an exchange guidewire (figure 3C,D). In contrast, the Headway 21, a comparator device with a guidewire, could not be made to cross this area of stenosis, despite the Bendit having been first passed through the area of stenosis. Finally, the Bendit 17 was used to deploy an LVIS 4.5 stent along the right carotid artery (figure 3E).
Endovascular coiling
Due to its unique bending and torqueing features, the Bendit 17 was used to precisely position coils in the dome of a bifurcation aneurysm (figure 4A). The Bendit 17 was then used to reposition the coils after detachment by pulling them toward the base of the aneurysm (figure 4B). The Bendit could then be used to reposition the detached coils back toward the dome of the aneurysm (figure 4C). The precise bending and torqueing features of the Bendit allow the user to place the second coil solely along the periphery of the aneurysm for more dense framing in a precise manner, as desired by the operator. Alternatively, the Bendit could be used to intentionally position the same coil at the center of the aneurysm in a stable manner. Finally, if the Bendit 17 came out of the aneurysm during coiling, it could easily and quickly be repositioned back into the side wall aneurysm, without the need for a guidewire and without withdrawing the coil.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
(A) The Bendit 17 can be used to position coils precisely in the dome of the aneurysm. (B) The Bendit 17 was used to reposition the coils within the aneurysm from (A) by pulling them toward the base. (C) The Bendit was used to reposition the coils from (B) back toward the dome of the aneurysm.
Side wall aneurysms
Three investigators were able to use the Bendit 17 to enter a small (<2 mm) side wall aneurysm without a guidewire (online supplemental figure 1A). The Bendit was used to place coils in a side wall aneurysm without the use of a guidewire (online supplemental figure 1B). Furthermore, the Bendit 21 was used to deploy two different intrasaccular devices in side wall aneurysms (online supplemental figure 1C,D). The Bendit remained in a stable position at the orifice of the aneurysm during the deployment of the two different intrasaccular devices.
Supplemental material
Histology
The Bendit microcatheters were bent in the carotid artery above the aneurysms in three rabbits, and rotated circumferentially three times, with no evidence of spasm, vessel damage or dissection, or thrombosis observed on angiography or histology. Online supplemental figure 2 shows representative images of the vessels during and after the procedure, showing no evidence of vessel damage as a result of catheter manipulation. Online supplemental figure 2A shows an explanted vessel including the carotid bifurcation after circumferential and linear advancement of the catheter, documenting tissue integrity. Online supplemental figure 2B shows a representative DSA of a vessel in vivo during manipulation with the Bendit 17 microcatheter without a guidewire, showing no evidence of tissue damage. Online supplemental figure 2C shows a cross section of an explanted vessel acutely after manipulation, showing no signs of vessel wall damage.
Discussion
Our in vivo experience with the Bendit microcatheter supports the effectiveness of its bending and torqueing capabilities for navigation and positioning, coupled with its stability in the bent position. The Bendit could be navigated through vasculature and made to enter the rabbit bifurcation and side wall aneurysms without a guidewire, and navigation can be facilitated by the injection of contrast material as the device is advanced, bent, and torqued. The Bendit was also maneuvered through stents and occluded vessels, which was not feasible with the Headway 21, a comparator microcatheter with a guidewire. Furthermore, coils could be introduced at different locations within the aneurysm and could be pushed, pulled, and repositioned at will. The Bendit has the potential to treat aneurysms for which conventional microcatheters are not suitable, such as side wall aneurysms requiring directional control and tip positioning while delivering intrasaccular devices.
In preparation for coil delivery with conventional microcatheters, it is not uncommon for the microcatheter tip to move when used with a guidewire.2 This tends to prevent coil deployment in the optimal direction and location.2 In contrast, the Bendit allows for the precise placement and repositioning of coils within the aneurysm, with the device remaining stable in the bent position. When delivering coils, this stability, along with the ability to micro-torque with more or less articulation, permits better packing density, avoids compartmentalization, and the need to re-catheterize poorly packed areas. When deflected, the Bendit can be used to intentionally pull on a coil, reposition migrated coils, or push coils to a specified target, such as the aneurysm tip. The Bendit’s fine tuning abilities enable the user to quickly fill in all empty spaces within the aneurysm, without the need to exit, reshape, and re-catheterize the aneurysm, thus preventing or decreasing compartmentalization. When the Bendit tip gets out of position, it can easily be repositioned without having to withdraw coils or use a guidewire, thus saving a great deal of time during procedures. An important consideration is to avoid over pushing devises. In all of our preliminary animal work, we intentionally pushed the coils aggressively to the maximum, without experiencing rupture. Before removing the catheter, the tip should be released into a neutral position to loosen the stability force, in order to minimize the risk of rupture, or accidentally dislodging a coil. Additionally, because these experiments were performed in aneurysms that were surgically created and matured, further studies in humans are needed to confirm these findings in a clinical setting.
The Bendit microcatheters are designed to be used with or without a guide wire; as such, they are ideal for treating side wall aneurysms that might otherwise require intraluminal flow diverting stents and antiplatelet medication for the patient.1 Furthermore, the WEB and other intrasaccular devices were developed specifically for the treatment of wide necked bifurcation aneurysms1 and generally cannot be used on side wall aneurysms because of their tendency to eject present catheters. Nevertheless, the Bendit 21 can be used to deliver intrasaccular devices such as the WEB 17 and the Contour Neurovascular System to wide neck side wall aneurysms. The stability of the tip in the bent position prevents the Bendit from being ejected from the aneurysm during device deployment and eliminates the need for additional devices, such as a stent or balloon to protect the aneurysm orifice. In the present study, after aggressive manipulation of the device within the vessel, there was no evidence of spasm, vessel damage or dissection, or thrombosis observed on angiography or histology (online supplemental figure 2). Therefore, the Bendit has the potential to expand indications for different intrasaccular devices to include side wall aneurysm embolization.
The Headway Duo is a comparator microcatheter that has flow directed properties and has also been navigated in cerebral vasculature without a guidewire.13 However, the Headway Duo lacks the Bendit’s real time bending and torqueing abilities. Furthermore, in our investigation, the Bendit 17 showed superior performance to the Headway 21 in being able to enter a nearly occluded right carotid artery. It is noteworthy, however, that the Headway 21 microcatheter used for the comparison has an outer diameter of 1.6 F vs the 2.5 F diameter of the Bendit 17. The SwiftNINJA microcatheter (Merit Medical) is also steerable, although its bending motions are restricted to two dimensions, as the device is not able to torque.8 10–12
The Bendit is a versatile device that supports coaxial/multiaxial telescoping and can be used with or without a guidewire and without the need for roadmapping. Because of the combined tube structure that allows the device to maintain its torsional rigidity, the Bendit devices can also be used with or without a guidewire. In this way, the device can be fully navigated from the puncture site to the target destination. The Bendit 17 has an internal diameter of 0.0165 inches (0.42 mm), which is achieved with a smaller outer diameter (2.5 F (0.033 inches or 0.83 mm)) relative to the Bendit 21 (3.1 F (0.041 inches or 1.03 mm)), resulting in a lower profile for navigation into small vessels.
Limitations
This study’s limitations include the qualitative study design, the small number of animals used for testing, and the different vascular anatomy and branching patterns between rabbits and humans. Thus the clinical safety and efficacy of the device need further assessment. Furthermore, with the exception of the Headway 21 comparison, this study had limited comparison with existing techniques and addressed difficult to quantify tests of catheter navigation, stability, and tip manipulability.
Conclusions
In this study, we described and investigated the effectiveness of the Bendit 17 and Bendit 21 microcatheters, which enable bending and torqueing during navigation and delivery, with or without a guidewire. Our preclinical investigations of the Bendit demonstrated its ability to be maneuvered through tortuous vessels, braided stents, and occlusions, and its ability to deliver and move coils. We also demonstrated its ability to treat side wall aneurysms and allow for the re-catheterization of an aneurysm during coiling without a guidewire.
Supplemental material
Data availability statement
No data are available. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
The study was approved by the committee for animal experiments from Land Salzburg, Austria (20901-TVG/136/10–2021).
Acknowledgments
The authors acknowledge Superior Medical Experts for literature research and drafting assistance.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors AB, EB, CH, and MK-O contributed to the design of the work, creation of the models, performance of the animal experiments, and interpretation of the results. AB, OC, and MK-O participated in drafting the article. EB and CH contributed to image collection, and critically reviewing the manuscript. All authors approved the final version to be published, and agree to be accountable for all aspects of the work. AB is the guarantor of the work.
Funding The study and manuscript development was sponsored by Bendit Technologies.
Competing interests AB is the CMO, a board member, and a shareholder of Bendit. OC is the inventor, the CTO, a board member, and a shareholder of Bendit.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.