Article Text

Abstract
Background Selection of appropriate surgical strategy for the treatment of intracranial aneurysms (IA) during pregnancy requires careful consideration of the potential risks to the mother and fetus. However, limited data guide treatment decisions in these patients. We compared the safety profiles of endovascular coiling (EC) and neurosurgical clipping (NC) performed for the treatment of ruptured and unruptured IA during pregnancy and the postpartum period.
Methods Pregnancy-related or postpartum hospitalizations undergoing surgical intervention for IA were identified from the Nationwide Readmissions Database 2016–2018. Safety outcomes included periprocedural complications, in-hospital mortality, discharge disposition, and 30-day non-elective readmissions.
Results There were 348 pregnancy-related or postpartum hospitalizations that met the study inclusion criteria (mean±SD age 31.8±5.9 years). Among 168 patients treated for ruptured aneurysms, 115 (68.5%) underwent EC and 53 (31.5%) underwent NC; whereas among 180 patients treated for unruptured aneurysms, 140 (77.8%) underwent EC and 40 (22.2%) underwent NC. There were no statistically significant differences in the baseline characteristics between patients undergoing EC versus NC for either ruptured or unruptured aneurysm groups. The outcomes were statistically comparable between EC and NC for both ruptured and unruptured IA, except for a lower incidence of ischemic stroke in patients undergoing EC for ruptured aneurysms (OR 0.12, 95% CI 0.02 to 0.84).
Conclusions Most pregnant and postpartum patients are treated with EC for both ruptured and unruptured IA. For treatment of ruptured IA, EC is independently associated with a lower risk of perioperative ischemic stroke, but other in-hospital complications and mortality are comparable between EC and NC.
- Aneurysm
- Coil
- Hemorrhage
- Intervention
- Subarachnoid
Data availability statement
Data are available in a public, open access repository. Data in this study were obtained from the Nationwide Readmissions Database, which is a publicly available database and can be obtained after completing the HCUP data use agreement.
Statistics from Altmetric.com
Key messages
What is already known on this topic
Endovascular coiling (EC) or neurosurgical clipping (NC) can be used for the treatment of IA; however, selection between these two surgical strategies in the unique setting of pregnancy requires careful consideration of the potential risks to the mother and fetus. There are limited data that guide the treatment decisions in these patients.
What this study adds
We found that most pregnant and postpartum patients are treated with EC for both ruptured and unruptured IA. We also observed that EC is associated with a lower rate of ischemic stroke in patients with ruptured IA.
How this study might affect research, practice, or policy
Given the lower rate of ischemic stroke with the use of EC, a staged procedure with emergent endovascular treatment to secure the ruptured aneurysm during pregnancy followed by a more definitive treatment with either EC or NC after delivery should be considered in the appropriate clinical scenario and explored in the future studies.
Introduction
Rupture of intracranial aneurysms (IA) during pregnancy carries significant morbidity and mortality for both mother and fetus. The incidence of non-traumatic subarachnoid hemorrhage (SAH) is estimated to range from 3 to 10 per 100 000 pregnancies.1 The hemodynamic and hormonal changes during pregnancy favor the formation, growth, and potential rupture of the IA,2 especially during the third trimester.3 The two most common methods for treatment of IA are endovascular coiling (EC) and neurosurgical clipping (NC). Both techniques have comparable efficacy, safety profiles, and 1-year morbidity and mortality rates.4 However, patients treated with EC may have shorter length of hospital stay and a lower rate of postoperative new neurological deficits.4 5 Management of IA during pregnancy is especially challenging due to the potential fetal risks associated with the exposure to anesthesia, contrast, and radiation; limits on maternal hyperventilation to lower intracranial pressure in the case of ruptured IA; and the obstetric bleeding risks associated with altered maternal coagulation cascade and the potential use of systemic anticoagulation during EC.3 To date, there have been no evidence-based guidelines to assist physicians with the choice of EC or NC when treating IA during pregnancy. In this study, we compare the safety profiles of EC and NC in the treatment of unruptured and ruptured IA during pregnancy and postpartum period.
Methods
Data source
Data in this study were obtained from the Nationwide Readmissions Database (NRD) 2016–2018, developed by the Agency for Healthcare Research and Quality for the Healthcare Cost and Utilization Project (HCUP). The NRD is an all-payer inpatient care database in the US containing approximately 57% of the total national hospitalizations. Sampling weights are available to obtain nationally representative estimates. The database contains a verified patient linkage number that can be used to track all admissions of an individual across different hospitals within a state and in a given calendar year. The NRD is a publicly available dataset that can be obtained after completion of the HCUP data use agreement.6 As the NRD contains deidentified retrospective data, ethical approval was not needed from the Institutional Review Board.
Study population
Each hospitalization in the NRD has a primary discharge diagnosis, up to 40 secondary diagnoses, and in-hospital procedures that are coded using the International Statistical Classification of Diseases and Related Health Problems, Tenth Revision (ICD-10) diagnosis and procedure codes, respectively. We used the ICD-10 codes to identify pregnancy- and postpartum-related adult hospitalizations (with age ≥18 years) that underwent either NC or EC for intracranial aneurysms. Hospitalizations with a concomitant diagnosis of SAH were classified as having ruptured aneurysms. Hospitalizations with diagnoses of arteriovenous malformation, cerebral arteritis, and traumatic SAH were excluded.
Covariates and study outcomes
The NRD contains information about the patient demographics, length of stay, in-hospital mortality, discharge disposition, total hospital charges, primary expected payer including Medicare, Medicaid, private insurance, and others, and hospital characteristics like bed size and teaching status. The ICD-10 diagnosis codes were used to identify the clinical features at presentation, the Charlson Comorbidity Index (CCI) score,7 and medical complications during the hospitalization. The ICD-10 procedure codes were used to identify interventions including delivery, EC, NC, ventriculostomy, prolonged ventilation, tracheostomy, and gastrostomy tube placement during the hospital stay. To determine if EC or NC was performed prior to or after delivery, the variable “PRDAYn” was used to obtain the day of EC/NC and the day of delivery. For hospitalizations where delivery information was not available, the ICD-10 diagnosis codes for pregnancy, labor/delivery, and puerperium were used to determine if the EC/NC was performed ante-, intra-, or postpartum. online supplemental table 1 includes the list of ICD-10 codes used to define the study population and covariates.
Supplemental material
The outcomes of interest included in-hospital mortality, discharge disposition, in-hospital complications, and 30-day non-elective readmissions. The in-hospital complications analyzed included ischemic stroke, prolonged mechanical ventilation, tracheostomy, acute kidney injury, gastrostomy tube placement, and infections. Discharge disposition was dichotomized as routine if the patient was discharged to home and non-routine if they were discharged to a short-term hospital, rehabilitation facility, home healthcare, or hospice.
Statistical analysis
Sampling weights were utilized to generate national estimates using the survey design methodology. Continuous variables were represented as mean±standard deviation (SD) and categorical variables as number and proportion percentage. The baseline characteristics were compared between the patients with EC versus NC using the chi-square test or two-tailed Student’s t test, as appropriate. Univariate and multivariable logistic and linear regression analyses were used to compare the study outcomes between the two groups. Multivariable models were adjusted for age, primary insurance, income quartile, stage of pregnancy, CCI score, and hospital characteristics. For readmission analysis, only the first hospitalization of the year for each individual patient with survival to discharge and known discharge disposition was included. Hospitalization records were excluded if the patient was a resident of a different state, as the readmissions are not tracked across the state lines, or if the discharge month was December, as the readmissions are not tracked across a calendar year so the 30-day readmission data would be lacking for those cases. All reported P values were two-sided with P<0.05 considered significant. All analyses were performed using Stata version 16.0 (StataCorp, College Station, TX, USA).
Results
During the study period, there were 11 829 044 hospitalizations with pregnancy or postpartum-related diagnoses. The study population consisted of 348 patients who underwent surgical intervention for IA during pregnancy or during the postpartum period up to 1 year after delivery. Of these, 168 patients were treated for ruptured aneurysms and the remaining 180 patients for unruptured aneurysms. The mean (SD) age of the study cohort was 31.8 (5.9) years. Among patients treated for ruptured aneurysms, 115 (68.5%) underwent EC and 53 (31.5%) underwent NC; whereas among patients with unruptured aneurysms, 140 (77.8%) underwent EC and 40 (22.2%) underwent NC. The baseline characteristics of patients undergoing EC versus NC were comparable for both ruptured and unruptured aneurysm groups (tables 1 and 2).
Baseline characteristics of patients with ruptured aneurysms
Baseline characteristics of patients with unruptured aneurysms
Among 168 patients treated for ruptured aneurysms, 17 (10.1%) had in-hospital mortality and 51 (30.0%) had non-routine discharge. The most common complications included prolonged mechanical ventilation in 38 (22.6%) patients, infections in 34 (20.2%) patients, ischemic stroke in 20 (11.9%) patients, tracheostomy in 11 (6.5%) patients, and acute kidney injury in 11 (6.5%) patients. Fewer than 5% of the patients underwent percutaneous gastrostomy tube placement. These outcomes were comparable between the EC and NC groups, except patients with EC were less likely to develop ischemic stroke (odds ratio (OR) 0.12, 95% CI 0.02 to 0.84) (figure 1). The length of stay was comparable between the two groups (mean±SD 19.1±17.2 vs 21.6±20.4 days, β-coefficient −1.17, 95% CI −8.56 to 6.23). Fewer than 5% patients had a non-elective readmission within 30 days of discharge. None of the readmissions were due to procedural complications, 75% of the readmissions were due to pregnancy-related conditions, and the remaining 25% were due to the neurological sequelae.

Comparison of clinical outcomes in patients with endovascular coiling (EC) versus neurosurgical clipping (NC) in patients with ruptured aneurysms. Data are shown as odds ratios (ORs) and 95% confidence intervals (CIs). All outcomes are adjusted for age, primary insurance, income quartile, stage of pregnancy, Charlson Comorbidity Index score, and hospital characteristics.
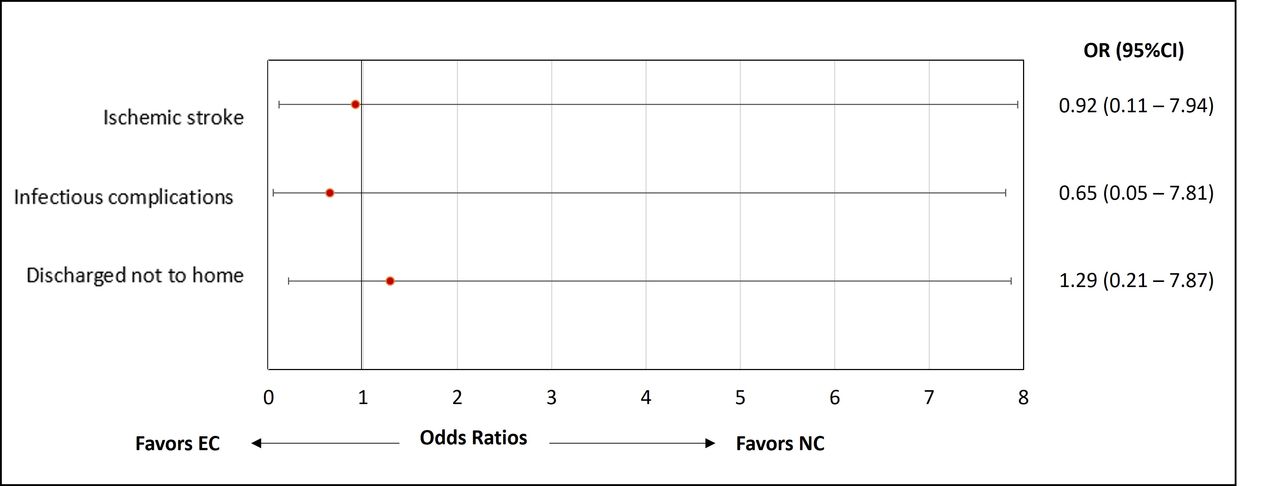
Among 180 patients treated for unruptured aneurysms, 20 (11.1%) had non-routine discharge, 11 (6.1%) had infectious complications, and 10 (5.6%) + had ischemic stroke. There were no statistically significant differences in these outcomes between the EC and NC groups (figure 2). The length of stay was comparable between the two groups (mean±SD 6.0±7.9 vs 6.1±7.7 days, β-coefficient −0.57, 95% CI −4.92 to 3.77).
{kind=link}
{kind=link}
Comparison of clinical outcomes in patients with endovascular coiling (EC) versus neurosurgical clipping (NC) in patients with unruptured aneurysms data are shown as odds ratios (ORs) and 95% confidence intervals (CIs). All outcomes are adjusted for age, primary insurance, income quartile, stage of pregnancy, Charlson Comorbidity Index score, and hospital characteristics.
Discussion
In this study we compared the safety profiles of EC versus NC for the management of IA during pregnancy and the postpartum period and found that the in-hospital safety outcomes for both techniques were comparable, except for a lower incidence of ischemic stroke that correlated with the use of EC among patients admitted with ruptured aneurysms.
The decision as to whether to observe versus surgically treat an unruptured IA requires careful balancing of the risk of rupture against the risk of complications from the procedure. To help guide the decision for treatment, different scoring systems have been developed, which incorporate patient- and aneurysm-related characteristics.8 If treatment is pursued, the two most common modalities include EC and NC. To date, only one randomized clinical trial has compared these two treatments for unruptured IA and found that even though patients with NC were more likely to have new neurological deficits and longer length of hospital stay, there were no significant differences in the 1-year morbidity or mortality rates between the two techniques.4 In agreement with the latter, several observational studies and meta-analyses also found that both techniques had comparable long-term outcomes.9 10 Regarding the emergent treatment of ruptured IA, the International Subarachnoid Aneurysmal Trial showed that patients undergoing EC have better functional outcomes, assessed using the Glasgow Coma Scale and modified Rankin Scale scores,11 a finding that was confirmed in other studies.12 13 In addition, patients undergoing EC have been shown to have similar 30-day mortality rates but possibly higher rates of recurrence and rebleeding.11 14 Rates of in-hospital mortality and average length of stay in this study were in line with prior data from non-pregnant adults.15 16
Management of unruptured IA during pregnancy is complicated by the hemodynamic and hormonal changes that may be associated with an increased risk of aneurysm growth and rupture,2 3 14 17 18 as well as the potential maternal and fetal complications from a surgical intervention. When to intervene for unruptured IA during pregnancy remains unknown; however, one may consider deferring treatment until the postpartum period unless there is a compelling indication for urgent intervention.18 Consistent with the prior literature, we found that EC was used more frequently than NC for the treatment of unruptured IA during pregnancy and postpartum period.3 These preferences may be due to the less invasive nature of EC and the higher risk of complications including rebleeding, symptomatic vasospasm, and postpartum cardiomyopathy reported with NC.19 However, no studies to date have performed a head-to-head comparison of the efficacy or safety profiles of EC and NC in the setting of pregnancy. In this study we did not observe any statistically significant differences in the medical complications (ischemic stroke, prolonged mechanical ventilation, and infections) or in-hospital mortality rates between the two techniques.
Ruptured IA are life-threatening to the mother and fetus and should be treated promptly.20 Aneurysmal SAH is the third most common non-obstetric cause of maternal mortality.19 21 More than three-quarters of IA rupture during the third trimester,3 likely due to the hemodynamic and hormonal changes as pregnancy progresses. The estimated maternal and fetal mortality from ruptured IA without intervention can be as high as 63% and 27%, respectively.22 Therefore, urgent treatment of ruptured IA during pregnancy and the ostpartum period is necessary.3 As with all aneurysmal SAH cases, an interdisciplinary team is needed; and during pregnancy, maternal–fetal medicine physicians and obstetric anesthesiology, where available, should also be involved.3 Depending on the fetal condition and gestational age, an emergent Caesarean delivery may be indicated.1 When EC is selected, potential fetal risks should be reduced by using abdominal shielding,23 minimizing the use of contrast as far as able,24 and proper positioning of the mother during and after the procedure to maximize venous return and placental blood flow.25 No prior studies have compared EC and NC for the treatment of ruptured IA during pregnancy. In this study we found a trend towards a lower rate of medical complications (ischemic stroke, prolonged mechanical ventilation, tracheostomy, acute kidney injury, and infections) and higher in-hospital mortality in patients undergoing EC; however, none of these results reached statistical significance apart from perioperative ischemic stroke.
Ischemic stroke after aneurysmal SAH is associated with significant morbidity and mortality. Stroke occurrence following SAH may be due to initial injury from aneurysm rupture, an underlying condition predisposing to both SAH and ischemic stroke, delayed ischemia from arterial vasospasm, or iatrogenic injury caused by NC or EC.26 Our finding of a lower rate of ischemic stroke in patients treated with EC as compared with NC for ruptured IA has been consistently reported in the prior studies including in non-pregnant patients.26 27 In our study this finding remained significant in the multivariable model, including the adjustment for whether the procedure was performed prior to or after delivery and other potential confounders. Furthermore, stratified analysis showed that the difference in the rates of ischemic stroke was even higher in the subgroup of patients with antepartum procedures versus those who had postpartum procedures. This finding suggests a higher significance of the difference in stroke rate between EC and NC during pregnancy as compared with the postpartum period. This also potentially suggests that a staged strategy with emergent endovascular treatment to secure the ruptured aneurysm to protect against rebleed during pregnancy followed by definitive treatment with NC or EC after delivery may be considered in the appropriate clinical scenario.28
Overall, the selection between EC and NC for the treatment of unruptured or ruptured IA during pregnancy is dependent on the individual patient- and aneurysm-related factors as well as the provider and institutional preferences. Although EC is gaining popularity,3 21 it requires systemic anticoagulation, which might be associated with a greater risk of bleeding, especially if an urgent Caesarean section is needed.3 17 Furthermore, EC carries the risk of fetal exposure to radiation with potential for congenital abnormalities and even death, particularly during the first trimester.29 Conversely, NC might have risks associated with prolonged procedure times.1 30 These differences may be inherent to the procedure itself as EC has shorter operating times12; however, larger and preferably randomized studies are needed to further explore these relationships, specifically in this subset of patients.
The findings of this study are novel and provide real-world data regarding the comparative safety profiles of EC versus NC for the treatment of ruptured and unruptured IA during pregnancy. However, our results should be interpreted in the light of the following limitations, most of which are inherent to using an administrative database. First, we did not have radiological data or detailed clinical information regarding the IA size, location, or SAH severity (in cases of ruptured IA), all of which could potentially influence both the choice of procedure and outcomes and hence bias our findings. Second, physician or institutional preferences for the choice of procedure could be another potential source of selection bias that could not be accounted for in this study. Third, non-routine discharge included discharge to short-term hospitals, rehabilitation facilities, home healthcare, or hospice and these different discharge outcomes could not be analyzed separately. Fourth, we did not have data regarding fetal outcomes. Finally, we did not have data regarding the functional neurological outcomes or long-term morbidity.
In conclusion, surgical treatment of IA during pregnancy and the postpartum period is safe and the in-hospital outcomes in these patients are comparable to those among non-pregnant adults. Most pregnant and postpartum patients are treated with EC for both ruptured and unruptured IA. For treatment of ruptured IA, EC is independently associated with a lower risk of perioperative ischemic stroke, but other in-hospital complications and mortality are comparable between EC and NC. Future large studies are needed to further evaluate the comparative utility of these procedures and to define when unruptured IA should be intervened on in this patient population.
Supplemental material
Data availability statement
Data are available in a public, open access repository. Data in this study were obtained from the Nationwide Readmissions Database, which is a publicly available database and can be obtained after completing the HCUP data use agreement.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
AG and AE contributed equally.
Contributors AG was involved in study concept/design, statistical analysis, drafting, revision of the manuscript and is responsible for the overall content. AE was involved in the interpretation of data and drafting of the manuscript. HR was involved in drafting and critical revision of the manuscript. SO-G was involved in study concept/design and critical revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests Santiago Ortega-Gutierrez receives grant funding from NIH, Stryker, medtronic and VizAi. He is consultant for Medtronic, Stryker and Microvention.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.