Article Text

Abstract
Objective/background Symptomatic subacute/chronic large artery intracranial occlusive disease represents a common medical dilemma. We now report a multicenter experience of endovascular recanalization of intracranial atherosclerotic occlusions refractory to medical therapy.
Methods Retrospective multicenter case series of consecutive endovascularly treated patients presenting with symptomatic (transient ischemic attack (TIA) or stroke) subacute (>48 h) or chronic complete occlusion of an intracranial artery of presumed atherosclerotic etiology. All of the patients were considered to be in the high risk category with symptomatic intracranial occlusions and progression or recurrence of their symptoms despite the best medical therapies.
Results 24 patients (median age 63 years; mean pretreatment National Institutes of Health Stroke Scale (NIHSS) score 10; 66% men) presenting with recurrent TIAs (n=1) or strokes (n=23) were treated in two academic centers from April 2005 to June 2012. Median time from symptoms/documented occlusion to treatment was 5 days. Periprocedural complications included one symptomatic intracranial hemorrhage, one reperfusion syndrome, three asymptomatic dissections, and one asymptomatic perforation. There were no periprocedural strokes. Immediate postprocedural improvement (NIHSS decrease ≥4 at hospital discharge) occurred in 43% (10/23) of patients. There were no recurrent TIAs or strokes in the 22 patients with clinical follow-up at 90 days. At 90 days, there were two deaths (unrelated to the procedure) and 9/22 patients with an available modified Rankin Scale (mRS) score achieved a good outcome (mRS score of 0–2).
Conclusions Endovascular recanalization can be performed with an acceptable safety profile in selected patients with symptomatic complete subacute to chronic intracranial atherosclerotic occlusion. Additional studies are warranted to investigate whether this treatment compares favorably with best medical management.
- Stroke
- Stent
- Intervention
- Atherosclerosis
Statistics from Altmetric.com
Introduction
Symptomatic subacute/chronic large artery intracranial occlusive disease (LAICOD) has been shown to be an independent predictor of death, poor outcomes, high recurrent stroke rates, and a major stroke problem worldwide, and remains a common medical dilemma.1 ,2 Studies have shown that large numbers of these patients will continue to be symptomatic despite maximal medical therapy.3 In particular, symptomatic LAICOD with chronic hemodynamic compromise are at high risk for subsequent stroke.4–8 Currently, no consensus exists on the optimal treatment of intracranial occlusive disease, especially in the setting of an evolving infarct and worsening symptoms. Vessel recanalization appears to have a powerful effect on clinical outcomes in acute ischemic stroke9; however, little is known about the feasibility and safety of this technique in subacute to chronic LAICOD.
The purpose of this study was to report on a multicenter experience of endovascular recanalization of non-acute intracranial atherosclerotic occlusions, which continued to be symptomatic despite maximal medical therapy.
Materials and methods
Two large regional referral stroke centers participated in this retrospective analysis of consecutive patients presenting with symptomatic (transient ischemic attack (TIA) or stroke) complete occlusion of an intracranial artery of presumed atherosclerotic etiology in whom endovascular therapy was performed beyond 48 h from the time last seen well. All of the patients were considered to be in the high risk category and had symptomatic intracranial occlusions with progression of their symptoms despite maximal medical therapy. We considered maximal medical management to be therapeutically dosed anticoagulation or dual antiplatelet therapy, cholesterol lowering agent, optimal blood pressure, and glucose control, as well as smoking cessation. All patients (except patient No 12) were thought to have progression of their symptoms based on the treating physician's judgment, which for the most part included a change in the score of the National Institutes of Health Stroke Scale (NIHSS) of ≥4 points, or recurrence of their symptoms despite medical management. They also had shown signs of hemodynamic failure, either through perfusion CT/MRI imaging, history, or physical examination.
In the case of patient No 12, a poor clinical examination (NIHSS score of 28) in the setting of a large vessel occlusion and relatively small core prompted endovascular therapy. Imaging selection was based on visual inspection of MRI or CT perfusion (CTP) scans (CTP for patients with anterior circulation disease only) demonstrating mismatch between presumably irreversibly compromised brain (diffusion weighted imaging (DWI) or CTP–cerebral blood volume lesion) and inadequately perfused brain (cerebral blood flow, mean transit time, or time to peak MRI, or CTP maps). None of the patients had evidence of intracranial hemorrhage or CT evidence of hypodensity involving greater than a third of the affected territory.
The majority of the patients had vertebrobasilar occlusions. All of the patients who underwent stenting of the vertebral artery occlusion either had contralateral vertebral artery disease (occlusion or significant stenosis) or a contralateral hypoplastic vertebral artery. The criteria that were used to select patients with posterior circulation occlusion included MRI-DWI to NIHSS mismatch (eg, clinical–core mismatch) in most of the patients (based on the treating physician's judgment as no set DWI or NIHSS was used) and clinical and radiographic findings that suggested hemodynamic failure, such as worsening symptoms in the upright position, worsening symptoms with lower blood pressure, or watershed pattern infarct on MRI.
The diagnosis of intracranial atherosclerosis as the primary etiology for the treated stenosis was based on a constellation of findings including: (1) presence of at least one major vascular risks factor (eg, hypertension, diabetes mellitus, dislipidemia, or smoking); (2) presence of multifocal intracranial stenosis with angiographic appearance consistent with intracranial atherosclerotic disease; (3) lack of improvement of the stenotic area on repeat imaging (suggesting intrinsic non-reversible lesion); (4) absence of any clinical, laboratory, or imaging findings suspicious for other potential causes of intracranial stenosis, such as vasculitis, Moya–Moya syndrome, reversible cerebral vasoconstrictive syndrome, cerebral vasospasm, and intravascular lymphoma; and/or (5) evidence of calcification at the level of the stenosis.
Cases were identified through a search of prospectively acquired endovascular databases at each of the institutions. The following baseline and treatment variables were studied: age, gender, and medical comorbidities. Angiographic images were analyzed and graded at each participating center. Patients were treated between April 2005 and June 2012. Institutional review board approval at each center was obtained according to each center's retrospective studies institutional review board policies and data analysis was carried out in a de-identified manner.
After occlusion of an intracranial vessel was identified, various recanalization strategies were used at the discretion of the operator. There was one case that was treated with angioplasty only; the other 23 cases involved stent placement. Flow through the previously occluded vessel was graded using the Thrombolysis in Cerebral Ischemia (TICI) grading system at each institution. Post-treatment imaging with CT or MRI was performed in all patients according to the local standard of care. All patients were discharged on dual antiplatelets, consisting of aspirin and clopidogrel, for a minimum of 6 months. Primary endpoints included successful recanalization (defined as TICI ≥2b) and good functional outcome (defined as a modified Rankin Scale (mRS) score of ≤2 at 3 months). Secondary endpoint included rates of symptomatic postprocedure parenchymal hematomas (PH, including both PH-1 and PH-2 according to the ECASS criteria)10 and mortality. Functional outcomes were obtained in the outpatient clinic, at follow-up, or by telephone. In cases when outcomes following discharge were not available due to loss of follow-up, the discharge mRS was carried forward.
Statistical analysis
Statistical analysis was performed using the STATA IC V.10 software (STATCorp LP, College Station, Texas, USA). Descriptive statistics were obtained.
Results
Twenty-four patients and 25 intracranial vessels were treated at two stroke centers (table 1). The pertinent clinical and treatment characteristics are summarized in table 2. Median age was 63 (40–88) years and the mean pretreatment NIHSS score was 10 (0–29). Sixty-six per cent (n=16) of patients were men. One patient had recurrent TIAs and the rest of the patients had recurrence or worsening stroke symptoms at the time of presentation. Median time from documented occlusion to treatment was 5 days. Occlusion sites included: internal carotid artery terminus (n=2), middle cerebral artery–M1 (n=4), basilar artery (n=9), and intracranial vertebral artery (n=9). One patient had both intracranial vertebral artery and basilar artery occlusions, both of which were treated, and one patient had occlusion of the distal cavernous and the origin of the internal carotid artery occlusions that were treated. Bare metal balloon mounted stents were used in 16 cases, drug eluting stents in seven cases, and one patient had angioplasty only.
Baseline patient characteristics and outcome
Baseline clinical variables and treatment modalities
Post-recanalization angiography demonstrated TICI 2b reperfusion in two cases and TICI 3 in 23 cases. Immediate post-treatment residual stenosis was <20% in 23 cases and 40% in one case. Periprocedural complications included one case of symptomatic intracranial hemorrhage, one case of reperfusion syndrome (seizures and cerebral edema), three asymptomatic dissections, and one asymptomatic perforation requiring coil sacrifice of the posterior cerebral artery. There were no periprocedural ischemic strokes.
Immediate postprocedural improvement (NIHSS decrease of ≥4 at hospital discharge) occurred in 43% (10/23) of patients. Re-stenosis (>50% stenosis+>20% absolute luminal loss) occurred in 2/16 patients with CT angiography or conventional angiography follow-up (asymptomatic). Average time to imaging follow-up was 4 months. The remaining patients did not have any follow-up imaging or were lost to follow-up. There were no recurrent TIAs or strokes in the 23 patients with clinical follow-up at 90 days. At 90 days, there were two deaths (unrelated to the procedure), and 41% (9/22) of patients with available mRS scores achieved a good clinical outcome (mRS score 0–2) and 64% (14/22) with available mRS scores achieved an acceptable outcome (mRS 0–3) (table 3, figure 1).
Clinical outcome and complications
{kind=link}
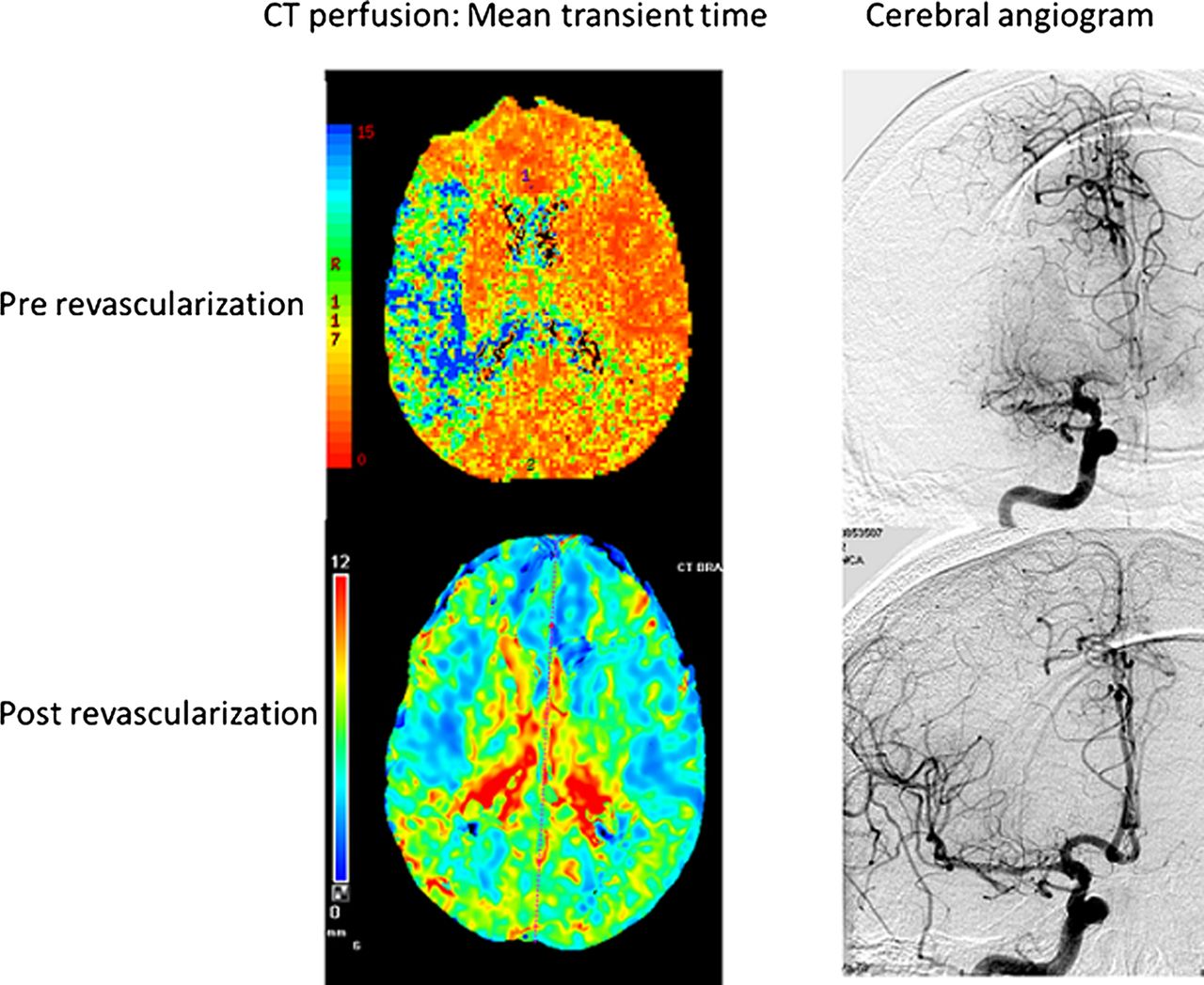
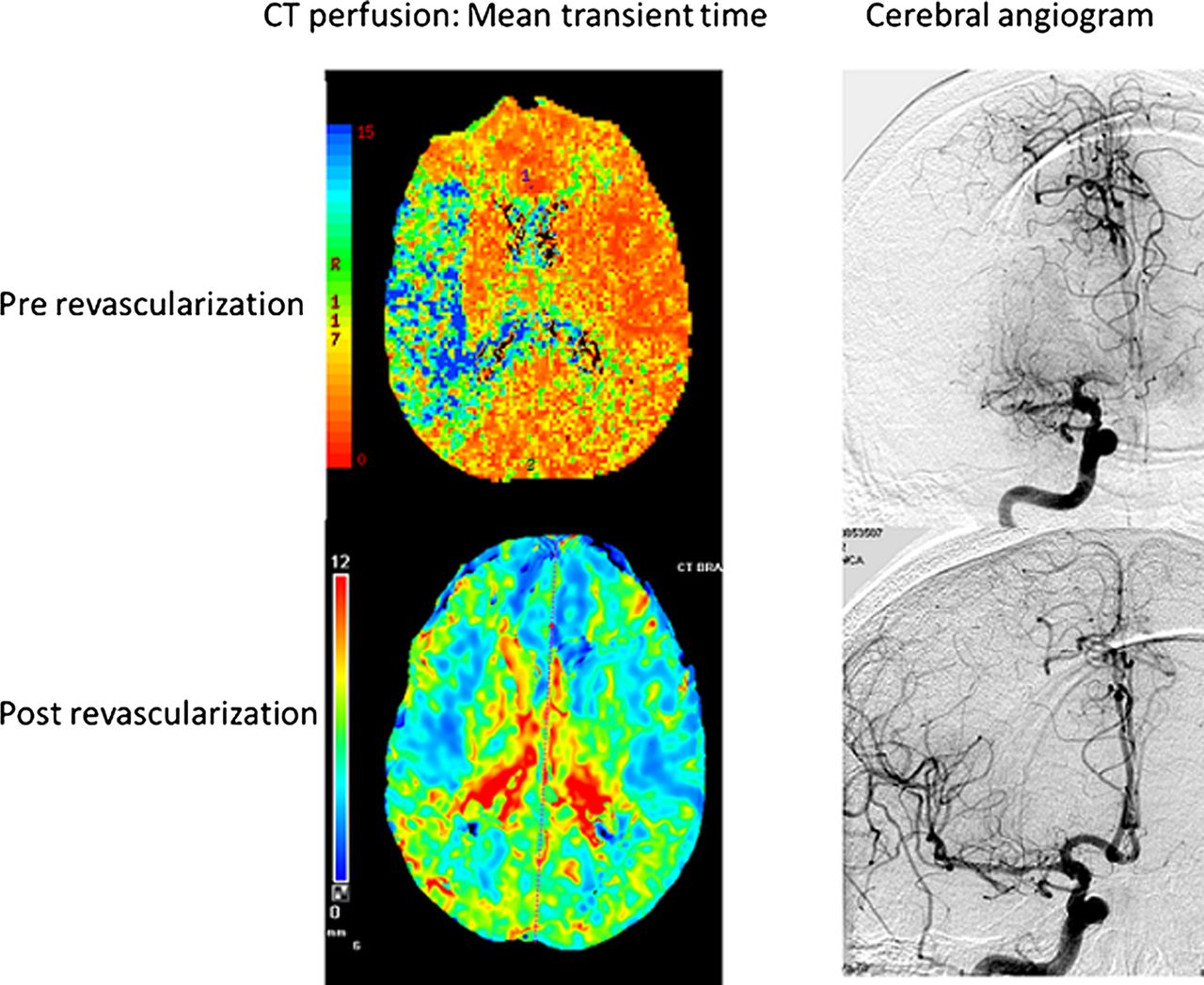
Patient No 4. This patient presented with progressive right middle cerebral artery syndrome despite medical management for 4 days. The National Institutes of Health Stroke Scale score was 4–12 prior to revascularization. The 90 day modified Rankin scale score was 2, with no recurrent symptoms post revascularization.
Discussion
This case series suggests that delayed recanalization of clinically unstable intracranial occlusions appears to be safe and efficacious in selected patients. To the best of our knowledge, this is the largest reported case series on endovascular treatment of subacute to chronic intracranial LAICOD.
There is not sufficient data regarding the optimal treatment of patients with large vessel intracranial occlusions who continue to be symptomatic despite best medical managements.2 Patients with acute embolic occlusions that leave little time for collateral formation as well as patients with atherothrombotic occlusions and poor collateral reserve are likely to deteriorate rapidly and have poor clinical outcome unless rapid revascularization treatment is instituted before irreversible ischemic injury occurs.11 However, there may be a subset of patients who have slower infarct growth and may benefit from delayed recanalization.12 Although delayed revascularization of posterior circulation stroke is reported and generally accepted,13 physicians are reluctant to treat delayed anterior circulation stroke patients with angioplasty and stenting because of technical difficulties and side effects, such as reperfusion injury or hemorrhagic transformation. However, symptomatic hemorrhage and cerebral edema occurred in only two patients in this case series.
It should be emphasized that revascularization of delayed symptomatic LAICOD is a high risk procedure; therefore, selecting the subgroup of patients who could benefit from this treatment is critical. Clearly, LAICOD is a heterogeneous disease and not everyone with subacute to chronic intracranial occlusions is a candidate for direct endovascular revascularization.
It is essential to highlight that all of these patients were unstable with progressive or fluctuating symptoms despite maximally optimized medical management. The recently reported SAMMPRIS trial demonstrated that intracranial revascularization with balloon angioplasty and stenting results in higher morbidity and mortality compared with aggressive medical therapy in clinically stable patients.14 The SAMMPRIS results are consistent with previous randomized clinical trials and a recent meta analyzes demonstrating that there is no benefit from stenting of the coronary arteries over medical therapy in clinically stable patients (eg, stable angina).15 ,16 Our patient population, however, was pathophysiologically equivalent to patients with unstable angina where stent revascularization has clearly demonstrated a benefit.
The small number of patients and the inherent flaws of a retrospective case series along with lack of a control arm limit this study. Another limitation is the heterogeneity of the patients in this case series and the fact that the majority of our patients had posterior circulation large vessel occlusions. It is believed that posterior circulation ischemia patients may have a lower reperfusion risk compared with anterior circulation occlusions.13 Prospective randomized control trials are therefore needed to investigate whether this treatment compares favorably with the best medical management. In addition, further data are needed to better select a subgroup of patients who would be eligible for this treatment. Other strategies for the treatment and prevention of LAICOD have been unsuccessful.2 Extracranial–intracranial arterial bypass surgery has failed to show any benefit in reducing ischemic stroke compared with medical management.17 Komotar et al18 failed to show any benefit of indirect bypass in the treatment of patients with medically refractory athero-occlusive disease and hemodynamic failure. Advanced endovascular treatment on the other hand offers an alternative option with an acceptable safety profile, as shown in this case series.
References
Footnotes
-
Contributors AA contributed substantially to the conception and design, acquisition of the data, analysis and interpretation of the data, drafting the article and revising the content, in addition to final approval of the paper. TJ, RG, and RGN contributed substantially to the analysis and interpretation of the data, revising the content, and final approval of the article. APJ contributed substantially to the conception and design, revising the content, and final approval of the article. AN contributed substantially to acquisition of the data, revising the content, and final approval of the article.
-
Competing interests None.
-
Ethics approval The study was approved by the institutional review boards of the University of Pittsburgh Medical Center and Emory Hospital.
-
Provenance and peer review Not commissioned; externally peer reviewed.