Article Text

Abstract
Background Carotid artery dissection is an important cause of stroke in young patients. Selection criteria for endovascular repair have not been well defined and limited data exist on long-term outcomes of stent reconstruction.
Objective To report the immediate and long-term clinical and radiographic outcomes of patients treated with stent placement for progressively worsening symptomatic carotid arterial dissection despite antithrombotic therapy.
Methods A single institution neuro-endovascular database was accessed to identify consecutive cases in which carotid artery dissection was treated with endovascular repair between 2006 and 2012. Clinical, demographic, radiographic, and procedural data were obtained through chart review.
Results A total of 22 patients were identified and included 27 carotid artery dissection repairs with stent implantation. The mean age was 43 years (±8.7) with 13 patients being women. Traumatic dissections were seen in 9 (40.9%) patients and spontaneous dissections in 13 (59.1%) patients. All patients were symptomatic and were started on antithrombotic therapy on diagnosis. Most common indications for treatment included recurrent ischemia despite antithrombotic therapy in 15 (55.5%) arteries and enlarging dissecting aneurysm in 4 (14.8%) arteries. Mean degree of stenosis was 79.1%. Mean number of stents used was 1.88 (range 1–4). There was 1 (4.5%) asymptomatic peri-procedural thromboembolic event. Median clinical follow-up was 14 months (range 3–40) and median imaging follow-up was 14 months (range 3–38). There was 1 (4.5%) case of recurrent transient ischemic attack. There was no death, significant restenosis or stroke in the territory of the treated vessel during the duration of the follow-up.
Conclusions Endovascular stent reconstruction for the treatment of selected patients with progressively worsening carotid dissection despite medical management is feasible with acceptable immediate and long-term clinical and radiographic outcomes. To be able to draw more robust conclusions, further evaluation with larger number of patients and longer follow-up is needed.
- Dissection
- Stent
- Stroke
- Artery
- Intervention
Statistics from Altmetric.com
Introduction
Carotid artery dissection is an important cause of stroke in younger patients and results from a tear in the intimal layer of the artery leading to stenosis or dissecting aneurysm or both.1–4 The incidence of spontaneous carotid artery dissection ranges from 2.5 to 3 per 100 0005 and it accounts for up to 25% of strokes in individuals aged less than 45 years and up to 2% of ischemic strokes overall.4 ,6 ,7 The reported mortality from spontaneous dissection is around 3–4%8 and that from traumatic dissections is about 10%.9 ,10
Data to guide optimal therapy for carotid dissection are limited. Although antithrombotic agents have been used as first-line therapy and have been generally considered sufficient for the treatment of carotid dissections,11 no rigorous appraisal of benefit has been reported. There are no randomised controlled trials comparing antiplatelet therapy to anticoagulation or either of them to placebo.3 ,12–14 In a Cochrane systematic meta-analysis of non-randomised studies, there was no significant difference found in the risk of stroke or death between anticoagulant and antiplatelet therapy.15
Endovascular therapy using stent reconstruction has been utilised as a safe and effective option for certain circumstances. The indications in prior multiple case series have included recurrent ischemia despite antithrombotic therapy, enlarging dissecting aneurysm, hemodynamic compromise related to the dissection, and tandem middle cerebral artery occlusion associated with complete occlusion of the internal carotid artery (ICA).16–20 Most reported series contain smaller numbers of patients with limited radiological and clinical follow-up. The largest reported series to our knowledge has been 44 patients but it also included asymptomatic patients.21 In a recent meta-analysis, the largest series reporting details regarding mechanism, location of dissections, type of stents used and clinical and imaging follow-up of at least 1 year included only 14 patients.22 We sought to review our experience and report immediate and long-term outcomes.
Methods
Consecutive patients treated with endovascular stenting for carotid dissection (spontaneous and traumatic) at our institution between January 2006 and July 2012 were identified from a prospectively maintained database. For these patients, we collected demographic and past medical history data (including age, sex, history of prior dissection in other vessels, hypertension, diabetes mellitus, cigarette smoking, coronary artery disease, congestive heart failure, atrial fibrillation, and family history of connective tissue disorders or spontaneous dissections). We reviewed pre and post procedural imaging, clinical course, and procedural details and follow-up evaluations. Dissections were classified as post traumatic if there was a history of high-energy non-penetrating injury like major blunt trauma or major accelerating–decelerating injury; in the absence of such trauma, they were classified as spontaneous.
Patient selection
At our institution, the diagnosis of clinically suspected dissection is confirmed by imaging characteristics on CT angiography (CTA) or MR angiography (MRA) or digital subtraction angiography (DSA). Patients were placed on antithrombotic therapy as decided by the treating physician and could either include antiplatelet therapy or anticoagulation using warfarin with an INR goal of 2–3. No specific blood pressure parameter was used and in the acute setting it was tailored according to the cerebral ischemic process at the discretion of the primary treatment team. Patients were selected for endovascular reconstruction only if they demonstrated features of progressively worsening dissection despite being on antithrombotic therapy (box 1). The timing of treatment was called acute if the patient was treated during the hospitalisation for the inciting event (trauma and/or cerebral ischemia) and chronic if the decision to treat was taken on an outpatient follow-up clinical or imaging evaluation.
Patient selection considerations for endovascular treatment
-
Recurring cerebral ischemia (strokes or transient ischemic attacks (TIAs)) despite antithrombotic therapy
-
Enlarging pseudo-aneurysm with or without worsening stenosis, despite antithrombotic therapy
-
Non-healing severe (>70%) stenosis despite antithrombotic therapy (on a scan done 3 or more months after the initial event) with either or both of the following:
-
Prior cerebral ischemia (TIA or stroke) attributable to that lesion
-
Persistence of non-ischemic symptoms (pressure or flow related) attributable to that lesion (eg, tinnitus)
-
-
Worsening stenosis on follow-up imaging, despite antithrombotic therapy in a patient with history of TIA/stroke/pressure or flow-related symptoms attributable to that lesion
-
Severe stenosis of hemodynamic significance (degree of stenosis >70% or presence of hypoperfusion on CT perfusion) stenosis with completely occluded contralateral carotid.
-
Tandem internal carotid and middle cerebral artery occlusion due to carotid dissection in the setting of acute stroke within 8 h from onset
-
Clinical evidence of hemodynamic insufficiency or hypoperfusion on perfusion imaging in a symptomatically unstable patient
Procedural protocol
Antithrombotic regimen
Patients received dual antiplatelet therapy (aspirin 325 mg and clopidogrel 75 mg) daily for at least 5 days. Patients who could not receive dual antiplatelet therapy for that period were loaded with oral aspirin 600 mg and clopidogrel 150–300 mg on the day of the procedure. For patients who were taking warfarin on a long-term basis, it was discontinued 5 days before the procedure. Dual antiplatelet therapy was continued for at least 3 months after the procedure beyond which only a single antiplatelet agent (aspirin 325 mg daily) was continued.
Procedural technique
Procedures were performed with patients under general or monitored anaesthesia care. Intravenous heparin was given during the procedure to maintain an activated clotting time between 250 and 300 s. A trans-femoral arterial approach was used and a 6–8 French sheath was positioned in the common carotid artery. Microcatheter access distal to the lesion was obtained in all cases and angiography was performed to confirm intraluminal position. The use of distal embolic protection was operator dependent and was used when the severity of the stenosis did not preclude passage of the protection device. Pre-stent angioplasty was done in selected cases when it was deemed necessary to improve lumen diameter for the safe passage of the stent delivery system. Stent implantation was performed per standard protocols.
Clinical and radiological outcome analysis
Duration of clinical and imaging follow-up was defined as the time to last outpatient follow-up and the time to last imaging (CTA/DSA) respectively. If there was any worsening or occurrence of any new neurological deficit after the procedure then standard definitions of transient ischemic attack (TIA) and stroke were used to define these events. The occurrence of any recurrent stroke, TIA, cardiovascular event or death was recorded. Functional status was defined by modified Rankin Scale (mRS). CT angiograms were reviewed for re-stenosis (defined as new or worsening in-stent or peri-stent luminal narrowing) and dissecting aneurysm status.
Image analysis
All images (CTA/MRA/DSA) were reviewed. The DSA images were analysed to record the characteristics of the dissected vessel for the location, degree of stenosis (defined by the NASCET Criteria), type of stenosis (smooth or irregular), presence or absence of intimal flap, false lumen, presence of thrombus and/or distal emboli and presence and characteristics of dissecting aneurysm. All arteries were analysed for tortuosity and were classified as one of the following four: no significant tortuosity, mild to moderate kinking (angle between the two segments forming the kink measured >30°, severe kinking (angle between the two segments forming the kink measured <30°), coiling (or 360° loop).23 All dissecting aneurysms were further studied for their location, size (large if >10 mm), shape (saccular, cylindrical or fusiform), immediate post-stent status and appearance on follow-up imaging. A dissecting aneurysm was considered to be increasing in size if there was any increase in the size compared with last imaging analysis.
Results
Patient characteristics
Stenting was performed in 27 arteries in 22 patients of which there were 13 women (59.1%) and 9 men (40.9%) with a mean age of 43.1 ± 8.7 years (range 21–66 years). Of these 22 patients, 9 (40.9%) had traumatic dissections (history of high-energy non-penetrating injury like major blunt trauma or major accelerating–decelerating injury) and 13 (59.1%) patients were classified as having spontaneous dissections, of which 3 had a history of trivial trauma (1 with severe coughing, 1 with straining due to severe constipation and 1 with prolonged biking). Bilateral dissections were seen in 5 (22.7%) patients, of which 3 had traumatic dissections and 2 had spontaneous dissections. Of the 27 dissected arteries treated, 15 (55.5%) caused recurrent ischemia despite antithrombotic therapy, 4 (14.8%) had an enlarging dissecting aneurysm with prior history of ischemic symptoms from that lesion (figure 1), 2 (7.4%) had worsening stenosis with prior history of ischemic symptoms from that lesion (figure 2), 2 (7.4%) had stenosis of hemodynamic significance on angiography with a completely occluded contralateral carotid, 1 (3.7%) had tandem occlusion of the ICA and middle cerebral artery, and 1 (3.7%) had hypoperfusion on perfusion imaging with a stenosis with hemodynamic significance on angiography. Two patients (14.8%) had non-healing severe (>70%) stenosis despite antithrombotic therapy (on a scan done 3 months after the initial event), with one of these patients having a history of prior cerebral ischemia (TIA or stroke) attributable to that lesion. Indications for treatment are listed in table 1. The timing of treatment was acute for 13 (48.1%) cases. Regarding associated comorbidities, 8 (36.3%) patients had a history of hypertension, 2 with concurrent coronary artery disease and hyperlipidaemia, and 1 with concurrent diabetes. All of these eight patients had spontaneous dissections. Nine (40.9%) patients had a history of smoking.
Clinical summary of all patients

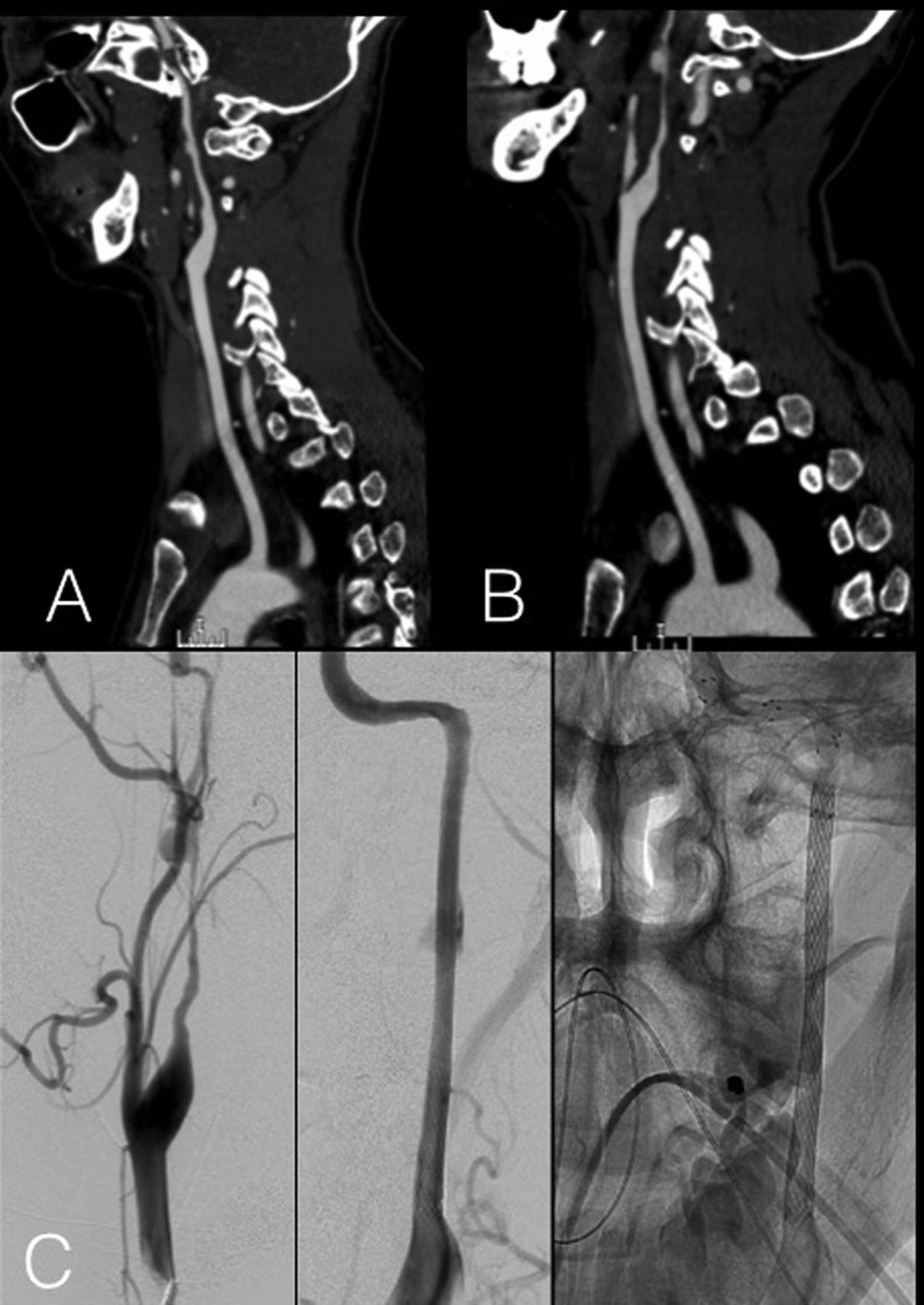
Patient 22 admitted after a major motor vehicle accident and was found to have a left hemispheric infarct. (A) Initial CT angiogram showing irregularly contoured left internal carotid artery (ICA) with stenosis which extends from proximal ICA (after the bulb) to the petro-laceral segment. Also seen is a dissecting aneurysm at the distal cervical segment of the ICA. The patient was started on antithrombotic therapy but 15 days later had a recurrence of ischemic symptoms in the territory of this artery. (B) CT angiogram shows worsened stenosis and expanding dissecting aneurysm. (C) Digital subtraction angiography done subsequently confirms the severe (99% with string sign) stenosis of the left ICA which was treated by three stents from the petrous portion of the ICA to the bulb with normalization of the contour and calibre. This patient also had dissection of the contralateral ICA (not shown).

{kind=link}
{kind=link}
Patient 7 with spontaneous right internal carotid artery (ICA) dissection presented with right hemispheric transient ischemic attack and continued to have recurrent right ocular ischemia despite anticoagulation. (A) First diagnostic angiogram (anterior posterior and lateral views) showing a long cervical ICA dissection with a 360° loop of the ICA. (B) Digital subtraction angiography repeated due to recurrence of symptoms shows worsened stenosis with almost 99% stenosis at the horizontal petrous segment with a string sign. (C) Artery was reconstructed using three stents—one open cell stent across the petrous segment of the ICA and two closed cell stents in the cervical ICA.
Characteristics of the dissected segment
Of the 27 arteries (18 right, 9 left), dissections were limited to the extracranial internal carotid in 14 (51.8%), had involvement of extracranial artery with intracranial extension in 12 (44.4%) and exclusively involved the common carotid in 1 (3.8%). Mean length of the dissected segment was 36.4 mm (range 5–105 mm). Mean degree of stenosis was 79.1%. Intimal flap was seen in 14 (51.8%) arteries and intraluminal thrombus was present in 3 (11.1%) arteries (1 spontaneous dissection and 2 traumatic dissections), of which 1 also had distal emboli (patient 3). A total of 24 dissecting aneurysms were present in 21 arteries, of which 14 were large (>10 mm) and 10 were small (<10 mm). They were classified as saccular in 11 cases, cylindrical in 12 and fusiform in 1 case (table 2).
Characteristics of the dissected vessel in spontaneous and traumatic dissections
Treatment characteristics
The mean number of stents used was 1.88 (range 1–4); a single stent was placed in 10 arteries and multiple stents were placed in 17 arteries. At least one closed cell stent was placed in all arteries with additional use of open cell stent in 10 arteries. All stents were self-expanding except on one occasion when a balloon mounted stent (patient 2) was used in addition to a self-expanding stent. A flow-diverting stent was used in one case (patient 21). For pre-procedure antiplatelet therapy, loading doses of antiplatelets were given for 17 procedures and daily dual antiplatelets for at least 5 days were given for 9 procedures. In only one patient (patient 3), no antiplatelets were administered prior to the procedure; rather they were given immediately after the procedure. This was a patient who presented after receiving intravenous tissue plasminogen activator (tPA) at another hospital within 6 h of his stroke symptoms. The stenting was not preplanned but had to be performed to gain access to distal embolic occlusion of the intracranial ICA. Since antiplatelet coverage was not felt to be adequate, the patient did not have the additional stenting for associated dissecting aneurysm treatment in the same procedure and a repeat procedure was performed 24 h later for stent placement and coiling of the dissecting aneurysm. General anaesthesia was used in six procedures whereas conscious sedation (or monitored anaesthesia care) was administered in all other procedures. Pre-stent angioplasty was done in four cases based on the operator's assessment of the need to obtain adequate lumen diameter for the safe passage of the stent delivery system. In all these cases except one, a distal protection device was used and a post-stent balloon angioplasty was performed. A distal protection was used in four other arteries and a post-stent angioplasty was additionally performed in six other instances.
Number and type of stents and coils used
The decision to use multiple stents was made to provide adequate coverage across the entire length of the lesion. Self-expanding stents were used in most cases. Closed cell stents were preferred for the cervical ICA except in very tortuous arteries where open cell stents were used. For intracranial ICA segments, open cell stents were preferred. The different stents used were Carotid Wallstent (Boston Scientific), Xpert (Abbott Vascular Devices), Xact (Abbott Vascular Devices), Nexstent (Boston Scientific), Precise (Codman Neurovascular), Neuroform (Boston Scientific), Liberte balloon-mounted (Boston Scientific), Veriflex balloon-mounted (Boston Scientific), Wingspan (Boston Scientific) and Enterprise (Codman Neurovascular). In one patient, a pipeline flow diverting stent (eV3) was deployed. One patient with tandem middle cerebral artery occlusion due to embolism was treated with intra-arterial tPA followed by mechanical thrombus disruption using MERCI Retrieval device (Concentric Medical). Only one dissecting aneurysm was treated with coil embolisation, with four coils delivered into the aneurysm lumen using a microcatheter placed over a guidewire through the struts of the deployed stent. The four coils included one Microplex18 4 mm×9 cm, Compass Complex, two Hydrocoil 10.3 mm×10 cm hydrosoft helical and one Hydrocoil 10.2 mm×10 cm hydrosoft helical.
Clinical and radiological outcomes
Immediate outcomes
Immediate post-stent residual was less than 30% in all but two cases in which the residual stenosis was 50% (patients 1 and 14). There were no strokes or TIAs in the peri-procedural period (table 3).
One procedure (patient 11) was associated with an embolic complication involving the ophthalmic artery which was treated with intra-arterial thrombolysis with complete recanalisation of the ophthalmic artery and no clinical sequelae. This patient also had mild atherosclerotic carotid disease and was one of the patients who had a pre and post stent angioplasty done and in whom a filter device was used.
Long-term outcomes
The median clinical follow-up was 14 months (range 3–40) and median imaging follow-up was 14 months (range 3–38). Compared with the immediate post-procedural residual stenosis, the degree of stenosis did not worsen in any of the stented arteries. Except one patient (patient 5) who had a TIA, there were no cases of TIA or stroke in the territory of the treated vessel or death during the duration of the follow-up. This patient had presented initially with left hemispheric TIA and right amaurosis despite being on anticoagulation. She underwent single stent placement in the left internal carotid followed a week later by placement of two stents for the right internal carotid dissection after which she was discharged on dual antiplatelet therapy. A week later she presented with left hemispheric TIA similar to initial presentation after which a catheter cerebral angiogram was performed which showed residual dissecting aneurysms and proximal displacement of the stent into the larger fusiform dissecting aneurysm. The decision to place additional stents was made to provide adequate coverage across the segment with the dissecting aneurysm. During the procedure, the previously placed stent became further displaced into the aneurysm and the distal wire caused an iatrogenic new dissection. This was treated with placement of additional stents. The patient did not have any clinical sequelae and at 1-year follow-up she had no clinical events, patent stents and a reduction in size of the dissecting aneurysm.
Resolution of dissecting aneurysms
Only one of the aneurysms (patient 3) was treated with coil embolisation in addition to stenting the carotid artery. Of the remaining 23 aneurysms for which no coiling was performed, all showed immediate post-stent reduction in their size with complete resolution in 5, partial resolution >50% in 10 and <50% resolution in 8 aneurysms. All of these completely resolved on a follow-up CTA performed 3–6 months after the procedure.
Discussion
Carotid artery dissections result from a tear in the intima and have been classified traditionally as traumatic (after high-energy non-penetrating injury or major accelerating–decelerating injury) or spontaneous (without any known trauma or after trivial trauma).2 ,4 ,24 ,25 Regardless of the etiologic mechanism, a tear in the intima leads to accumulation of blood which separates the arterial layers. Sub-intimal accumulation of blood causes luminal narrowing whereas sub-adventitial accumulation results in dissecting aneurysm formation. Moreover, disruption of the endothelium provides an environment for the formation of thrombus which can potentially embolise and cause cerebral ischemia.4 ,26
Antithrombotic treatment with antiplatelet or anticoagulation is currently the most accepted initial treatment strategy for carotid dissection. A recently published non-randomised arm of the Cervical Artery Dissection in Stroke Study (CADISS-NR) trial, comparing anticoagulation and antiplatelets for prevention of recurrent stroke after carotid and vertebral dissection, showed no evidence for superiority of anticoagulation or antiplatelet therapy in prevention of stroke.27 Natural history studies have shown a relatively benign course for a majority of patients on antithrombotic treatment. Healing of dissection occurs within 3–6 months with resolution of stenosis in up to 90% of cases.6 ,11 ,28 However, there are a minority of situations associated with progressive worsening of dissection manifested by recurrent ischemia despite antithrombotic treatment and/or enlarging dissecting aneurysm.14 ,29 In addition, progressively worsening stenosis or non-healing stenosis of a severe degree (>70%) on follow-up imaging has been shown to be twice as likely to be associated with recurrent stroke than transient stenosis.30 These situations warrant vessel reconstruction to prevent clinical deterioration.
Endovascular stenting is a viable option in these selected cases and has been shown to be safer than surgical reconstruction of the artery which either involves ligation of the artery and resection of the dissecting aneurysm or cervical artery to ICA bypass.21 ,22 ,31–33 In a recent systematic review of studies reporting endovascular treatment of carotid dissection that included 31 published reports, the technical success rate of stenting was 99%, and the procedural complication rate was 1.3%.14 ,29 Mean radiological follow-up was 12.8 months (range 2–72 months) and revealed in-stent stenosis or occlusion in 2% of patients. Mean clinical follow-up was 17.7 months (range 1–72 months), and neurological events were seen in 1.4% of patients. Another systematic review of published series of endovascular treatment of extra-cranial carotid dissections found a technical success rate of 100% with an overall rate of adverse events of 11% and no mortality.29 Our results are consistent with previously published reports involving endovascular therapy. Procedural success was achieved in all cases without any peri-procedural TIA, stroke or death. One episode of asymptomatic embolism was successfully treated without any clinical impact. On a mean post-procedural clinical follow-up of 18.3 months, only one patient had recurrent TIA; a repeat angiogram was done which showed stenosis distal to the stented segment for which an additional stent placement was attempted that resulted in an iatrogenic dissection which was then further treated with implantation of multiple stents. On a mean radiological follow-up of around one and a half years, there were no instances of recurrent stenosis or retreatments. There was no difference between the spontaneous and traumatic dissection groups in terms of deaths, strokes or stent patency for the period of available follow-up.
Summary of endovascular procedure, clinical and radiographical outcomes
Although a benign course of dissecting aneurysms has been reported on antithrombotic treatment,8 ,34 there have been reports of high combined major stroke and death rate related to dissecting aneurysms.35 A dissecting aneurysm that increases in size on conservative management could be considered ominous and such aneurysms have been considered for interventional management.22 ,30 ,36 A large proportion of the treated arteries in our series were associated with dissecting aneurysms. An expanding dissected aneurysm was the reason for intervention in four cases. All of them showed complete resolution within 6 months of stenting. All but one aneurysm was treated with stenting alone, which supports previously published reports that stenting without coil embolisation might be sufficient for treating extra-cranial carotid artery dissecting aneurysms.
Use of a distal protection device for stenting carotid dissection remains controversial. In one series a protection device was almost always used21 whereas other authors preferred to perform stenting without its use.16 ,31 The argument against not using a distal protection device is that the risk of worsening the dissection or creating a new intimal tear is greater than the potential for embolisation given the lack of bulky plaque underlying the stenosis. In the current series, distal protection device use was at the discretion of individual operators. Interestingly, only one peri-procedural embolic complication occurred, which was in a patient in whom distal protection was used.
Our study is limited by retrospective design and relatively limited follow-up. Additionally, we do not have data regarding antiplatelet resistance testing for patients who were on antiplatelets and our radiological follow-up is with CTA, which is limited by metal and bone artifacts. Consideration of an invasive therapy should include a detailed analysis of risks and benefits and needs to be individualised on a patient-specific basis. This series suggests that our current practice of initially treating all patients with antithrombotic therapy and then escalating to endovascular therapy based on specific indications and careful patient selection is safe and effective. Undoubtedly, randomised controlled trial data comparing endovascular treatment with antithrombotic therapy are needed to answer this question.
References
Footnotes
-
Contributors All authors contributed towards conception and design, reviewing literature, drafting the article, revising it critically for important intellectual content and final approval of the version to be published.
-
Competing interests None.
-
Ethics approval IRB.
-
Provenance and peer review Not commissioned; externally peer reviewed.